Communicating Family Planning in Reproductive Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lactational Amenorrhea Method
Lactational Amenorrhea Method Dr. Raqibat Idris [email protected] From Research to Practice: Training in Sexual and Reproductive Health Research 2017 Objectives of presentation • Define Lactational Amenorrhea Method (LAM) • Understand the mechanism of action of LAM • Know the efficacy of LAM • Know and describe the 3 criteria for LAM • Know the indication and contraindications for LAM • Know the focus and timing of counselling for LAM • List the advantages, disadvantages and health benefits of LAM • Know the elements of programming necessary for the provision of quality LAM services Introduction Breastfeeding delays the return of a woman’s fertility in the first few months following childbirth. Women who breastfeed are less likely to ovulate in this period. When compared with women who breastfeed partially or who do not breastfeed at all, women who breastfeed more intensively are less likely to have a normal ovulation before their first menstrual bleed postpartum (Berens et al., 2015). In a consensus meeting in Bellagio, Italy in 1998, scientists proposed that women who breastfeed fully or nearly fully while they remain amenorrhoeic in the first 6 months postpartum experience up to 98% protection from pregnancy. This formed the basis for the Lactational Amenorrhea Method and has since then been tested and confirmed by other studies (Berens et al., 2015; Van der Wijden et al., 2003; WHO, 1999). Berens P, Labbok M, The Academy of Breastfeeding Medicine. ABM Clinical Protocol #13: Contraception During Breastfeeding, Revised 2015. Breastfeeding Medicine. 2015 Feb;10(1):3-12. The World Health Organization multinational study of breast-feeding and lactational amenorrhea. III. -

Sex-Selective Abortions, Fertility, and Birth Spacing*
Sex-Selective Abortions, Fertility, and Birth Spacing* Claus C Portner¨ Department of Economics Albers School of Business and Economics Seattle University, P.O. Box 222000 Seattle, WA 98122 [email protected] www.clausportner.com & Center for Studies in Demography and Ecology University of Washington November 2016 *I am grateful to Andrew Foster and Darryl Holman for discussions about the method. I owe thanks to Shelly Lundberg, Daniel Rees, David Ribar, Hendrik Wolff, seminar participants at University of Copenhagen, University of Michigan, University of Washington, University of Arhus,˚ the Fourth Annual Conference on Population, Repro- ductive Health, and Economic Development, and the Economic Demography Workshop for helpful suggestions and comments. I would also like to thank Nalina Varanasi for research assistance. Support from the University of Wash- ington Royalty Research Fund and the Development Research Group of the World Bank is gratefully acknowledged. The views and findings expressed here are those of the author and should not be attributed to the World Bank or any of its member countries. Partial support for this research came from a Eunice Kennedy Shriver National Institute of Child Health and Human Development research infrastructure grant, 5R24HD042828, to the Center for Studies in Demography and Ecology at the University of Washington. Prior versions of this paper were presented under the title “The Determinants of sex-selective Abortions.” Abstract This paper addresses two main questions: what is the relationship between fertility and sex se- lection and how does birth spacing interact with the use of sex-selective abortions? I introduce a statistical method that incorporates how sex-selective abortions affect both the likelihood of a son and spacing between births. -

Pre and Interconception Health, Intentionality and Birth Spacing: Emerging Issues
PRE AND INTERCONCEPTION HEALTH, INTENTIONALITY AND BIRTH SPACING: EMERGING ISSUES Monday, May 21 1:30 PM - 3:00 PM #prematuritycollab Pre- and Interconception Health, Intentionality, and Birth Spacing: Emerging Approaches Prematurity Prevention Summit Building a Birth Equity Movement Welcome • Co-chairing the Prematurity Collaborative Clinical and Public Health Practice Workgroup ‣ With Vanessa Lee, MPH (HRSA) • Great group of people; very dedicated • Focus on 3 main topics: ‣ 17-P ‣ LDASA ‣ Intentionality and birth spacing Background • Approximately half of pregnancies in US are unintended ‣ Better in teens, but still unacceptably high • Intentionality is important ‣ Unintended pregnancy associated with adverse maternal and child outcomes ‣ Negative impact on physical and mental health ‣ Disproportionate impact › Higher rates in lower SES and lower levels of achieved education ‣ Expensive… › 2010 estimate: $21 billion in public expenditure for unintended pregnancy Background – Birth Spacing • Based on data suggesting short interpregnancy intervals associated with worse outcomes ‣ Including prematurity ‣ Others: fetal growth restriction, NICU admission, perinatal death • Intervals “debated”…. ‣ < 24 months, especially < 18 months • “Recommendations” to avoid short intervals ‣ Healthy People 2020 objective: 10% reduction in pregnancies within 18 months ‣ WHO: minimum birth-to-pregnancy spacing of 2 years ‣ ACOG: short intervals mentioned as a risk factor for preterm delivery and adverse neonatal outcomes • Widespread emphasis ‣ Made sense -

NFP Related Research ……………………………………………
1 Winter/Spring 2000 ● Vol. 11, Nos. 1 and 2 Richard J. Fehring, DNSc, RN, Marquette University College of Nursing In this issue NFP Related Research ……………………………………………. 2 Pregnancy and Breastfeeding …………………………………….. 8 Contraception ……………………………………………………… 11 Research Briefs …………………………………………………….. 14 Under the Microscope ……………………………………………... 19 The Effectiveness of Natural Family Planning, Robert T. Kambic, MSH Current Medical Research is a publication of the Natural Family Planning Program of the United States Conference of Catholic Bishops.© Washington, DC: USCCB, 2011. The managing editor is Theresa Notare, PhD, Assistant Director. Permission is granted to reproduce in whole or in part, in print and/or electronically, with the following statement: Current Medical Research, NFPP/US Conference of Catholic Bishops, Washington, DC, volume # (year): page#. Used with permission. 2 Natural Family Planning United States Physicians Underestimate Effectiveness of Natural Family Planning A recent study conducted by researchers at the University of Missouri-Columbia, found that 79% of physicians in Missouri estimated the best possible effectiveness of natural family planning for avoiding pregnancy to be less than 91%. Sixty-five percent of those surveyed ranked the actual effectiveness of NFP to be 70% or less.1 The purpose of the study was to determine physicians' knowledge and practices of modern methods of NFP. The researchers assumed that modern methods of NFP are important for medical practice in order to help women and couples avoid or achieve pregnancy. A one page questionnaire on knowledge and practice of NFP was created by the researchers and mailed to 840 randomly selected physicians in Missouri. While 69% of the 547 respondents saw women for reproductive needs, only 46% mentioned NFP to at least some women when discussing family planning issues. -

Glossary of Common MCH Terms and Acronyms
Glossary of Common MCH Terms and Acronyms General Terms and Definitions Term/Acronym Definition Accountable Care Organizations that coordinate and provide the full range of health care services for Organization individuals. The ACA provides incentives for providers who join together to form such ACO organizations and who agree to be accountable for the quality, cost, and overall care of their patients. Adolescence Stage of physical and psychological development that occurs between puberty and adulthood. The age range associated with adolescence includes the teen age years but sometimes includes ages younger than 13 or older than 19 years of age. Antepartum fetal Fetal death occurring before the initiation of labor. death Authorization An act of a legislative body that establishes government programs, defines the scope of programs, and sets a ceiling for how much can be spent on them. Birth defect A structural abnormality present at birth, irrespective of whether the defect is caused by a genetic factor or by prenatal events that are not genetic. Cost Sharing The amount an individual pays for health services above and beyond the cost of the insurance coverage premium. This includes co-pays, co-insurance, and deductibles. Crude birth rate Number of live births per 1000 population in a given year. Birth spacing The time interval from one child’s birth until the next child’s birth. It is generally recommended that at least a two-year interval between births is important for maternal and child health and survival. BMI Body mass index (BMI) is a measure of body weight that takes into account height. -

Packages of Interventions for Family Planning, Safe Abortion Care, Maternal, Newborn and Child Health WHO/FCH/10.06
Packages of Interventions for Family Planning, Safe Abortion care, Maternal, Newborn and Child Health WHO/FCH/10.06 Acknowledgement This document has been developed by the World Health Organization. It includes inputs from UNICEF, UNFPA, The World Bank and different members of The Partnership for Maternal, Newborn and Child Health (PMNCH). Bilateral partners also made valuable contributions. © World Health Organization 2010 All rights reserved. Publications of the World Health Organization can be obtained from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters. All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. -
Natural Family Planning
your guide to natural family planning Helping you choose the method of contraception that is best for you natural family planning naturalnatural family family planning planning naturalnatural familynatural family planning planning natural family planning natural family planning familynatural family planning natural family planning natural familynatural planning family planning natural family planning planningnatural family planning natural family planning familynatural planning familynatural family planning planning 2 3 What is the menstrual cycle? Natural family The menstrual cycle is the time from the first day of your period to the day before your next period starts. The average length of the menstrual planning cycle is around 28 days, although many women have longer or shorter cycles and this is normal. This booklet gives information on how natural Regardless of how long or short the cycle is, family planning can help you to avoid pregnancy. ovulation (when the ovaries release an egg) will usually happen around 10–16 days before the Fertility awareness involves being able to identify start of the next period. During your menstrual the signs and symptoms of fertility during cycle: the menstrual cycle so you can plan or avoid O Eggs develop in your ovaries and usually one is pregnancy. released. O The mucus in the cervix (entrance to the uterus – womb) changes to allow sperm to Contents What is the menstrual cycle? .......................................................3 How can I work out how long my menstrual cycle How does natural -

Assessing the Impact of Birth Spacing on Child Health Trajectories
Global Development Policy Center HCI WORKING PAPER 001 • SEPT 2018 HUMAN CAPITAL INITIATIVE Assessing the Impact of Birth Spacing on Child Health Trajectories MAHESH KARRA ABSTRACT We investigate the effect of birth spacing between siblings on child health trajectories and invest- ments using longitudinal data from the Young Lives Study. We analyzed a birth cohort of over 7,000 children with data collected between 2002 and 2013 from four low- and middle-income countries. We found increased height among children who were more widely spaced relative to children who were narrowly spaced (within two years from an older sibling). However, we also found evidence of Mahesh Karra is an Assistant compensatory growth (converging height and HAZ scores) for closely spaced children as they aged. Professor of Global Development There was a positive association between birth spacing and prenatal investments, which suggests Policy at the Frederick S. that the emergence of height gaps could have been driven by parental behavior in addition to bio- Pardee School of Global Studies logical factors. However, we found little evidence that compensatory growth was driven by remedial at Boston University and health investments in closely spaced children after birth, suggesting catch-up growth as a biological Associate Director of the Human phenomenon. Available data suggests financial constraints and caregiver perceptions of child health Capital Initiative at the Global Development Policy Center. as possible explanations for lack of remedial investments. Keywords: birth spacing, health, nutrition, child investments, compensatory growth, height HCI@GDPCenter www.bu.edu/gdp Pardee School of Global Studies/Boston University 1 Introduction The importance of birth spacing for maternal and child health has been a long-standing source of interest to researchers and policymakers (World Health Organization, 2005). -

Natural Family Planning Fact Sheet
Natural Family Planning Fact Sheet ____________________________________________________________________________ 24-hour Emergency Number/Location WHAT’S INSIDE: SOURCES: What is the natural family planning? Office on Women’s Health Basal body temperature method Calendar Method Birth Control Methods: Frequently Cervical Mucus Method Asked Questions How effective are natural family Fertility Awareness planning methods? Advantages of natural family Centers for Disease Control and planning Prevention Drawbacks of natural family planning Unintended Pregnancy Prevention: Contraception U.S. Department of Health & Human Services 200 Independence Avenue, S.W. Washington, D.C. Oklahoma State Department of Health ODH Form 337 MCH/Perinatal & Reproductive Health Division/Family Planning Program Revised Oct 2014 Office of Population Affairs Natural Family Planning Fact Sheet How effective is natural family planning? Of 100 couples who use natural family planning methods each year, anywhere from 1 to 25 will become pregnant. Natural family planning can be an effective type of birth control if all three methods are used and if all are always used correctly. What is natural family planning? A woman with a normal menstrual cycle has about 8 days a month when she can get pregnant. These include the five days before she ovulates (when an egg is released), the day she ovulates, and about one to two days after ovulation. Natural family planning (sometimes known as fertility awareness or the rhythm method) is an approach to birth control some couples use to predict when these fertile days happen. It involves paying close attention to the menstrual cycle by using methods that include: Basal Body Temperature Method Calendar Method Cervical Mucus Method When all three methods are used together, it is known as the symptothermal method. -
Healthy Timing and Spacing of Pregnancies: a Family Planning Investment Strategy for Accelerating the Pace of Improvements in Child Survival
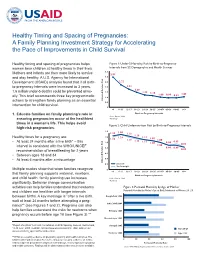
Healthy Timing and Spacing of Pregnancies: A Family Planning Investment Strategy for Accelerating the Pace of Improvements in Child Survival Healthy timing and spacing of pregnancies helps Figure 1: Under-5 Mortality Risk by Birth-to-Pregnancy women bear children at healthy times in their lives. Intervals from 52 Demographic and Health Surveys 3.5 Mothers and infants are then more likely to survive 2.97 and stay healthy. A U.S. Agency for International 3.0 Development (USAID) analysis found that if all birth- 2.5 2.22 to-pregnancy intervals were increased to 3 years, 2.0 1.81 1.49 1.6 million under-5 deaths could be prevented annu- 1.5 1.22 1.14 1.00 0.96 0.92 1.05 ally. This brief recommends three key programmatic 1.0 actions to strengthen family planning as an essential Risk Adjusted Relative 0.5 intervention for child survival. 0 <6 6–11 12–17 18–23 24–29 30–35 36–47* 45–59 60–95 96+ 1. Educate families on family planning’s role in Birth-to-Pregnancy Intervals Source: Rutstein, 2008 ensuring pregnancies occur at the healthiest *Ref Group times in a woman’s life. This helps avoid Figure 2: Child Undernutrition Risk by Birth-to-Pregnancy Intervals high-risk pregnancies. 1.4 1.30 1.25 1.12 1.16 Healthy times for a pregnancy are: 1.2 1.29 1.11 1.22 1.07 1.19 1.13 1.00 • At least 24 months after a live birth* – this 1.0 1.11 0.90 0.95 1.06 0.82 interval is consistent with the WHO/UNICEF 1.00 0.8 0.90 0.89 recommendation of breastfeeding for 2 years 0.82 • Between ages 18 and 34 0.6 • At least 6 months after a miscarriage 0.4 Adjusted Relative Risk Adjusted Relative 0.2 Stunted Underweight Multiple studies show that when families recognize 0 <6 6–11 12–17 18–23 24–29 30–35 36–47* 45–59 60–95 96+ that family planning supports maternal, newborn, Birth-to-Pregnancy Intervals and child health, family planning use increases Source: Rutstein, 2008 *Ref Group signifi cantly. -

Bulletin of WOOMB International
Bulletin of ISSN 2202-7599 WOOMB International Ltd Vol 48 No 1 March 2021 Credidimus caritati we have put our faith in love WOOMB International Ltd continuing the work of Drs John and Evelyn Billings of bringing the Billings Ovulation Method® to the world. Table of Contents Page In this Edition Editor 2 Spiritual Direction for Billings Ovulation Method® Fr Joseph Hattie, OMI 3 teachers The Difference Anon 5 Questions about the application of Early Day Rule 2 Question to Senior Teachers 6 Snippets of Inspiration Various authors 7 Abstinence Makes the Heart Grow Fonder - Men in Dr Nicholas Tonti-Filippini 9 Love (extract) Vale Professor Len Blackwell 11 Meet Fr Joseph Hattie OMI 12 Doctor decries misrepresentation of effectiveness of 14 Fertility Awareness Methods News from the Directors 15 News Around the World 16 Message on the Feast of the Holy Family Pope Francis 19 20 Natural Family Planning and the Conjugal Relationship E. L. Billings (extract) 22 The Sub-Fertile Couple (extract) Rev Maurice Catarinich Your subscription/donation WOOMB International continues the work of its founders by promoting the Billings Ovulation Method® and ensuring that wherever it is taught globally, it is the authentic Method without variation, and that only WOOMB International approved teaching and training materials are used.The Bulletin provides a medium for sharing articles and news from around the world. We welcome your annual subscription of AUD$25 which will ensure its continuing production. Bulletin Subscription: AUD $25 Donation: $_____ Make a secure online donation today at www.givenow.com.au/billingslife. In the message space write: “WOOMB International Bulletin Subscription/Donation”. -

Fertility Awareness Methods Do Not Work If You Do Not Have Regular Periods
Fertility Awareness What is Fertility Awareness? Fertility Awareness allows you to prevent pregnancy without using any drugs or devices. Natural Family Planning (NFP) is another name for Fertility Awareness. What makes Fertility Awareness unique? Fertility awareness differs from other types of birth control. Birth control prevents sperm from meeting eggs. Most birth control must be used each time you have sex. Fertility awareness tells you when you are most likely to become pregnant. These are your fertile days. Fertility awareness requires you to avoid vaginal sex on your fertile days. Things to Know Fertility awareness does NOT require you to use pills or condoms or to have devices in your body. Fertility awareness is a safe method of birth control. Fertility awareness is acceptable to some religions that oppose birth control. Fertility awareness does NOT protect against HIV and other sexually transmitted infections (STI). You cannot have vaginal sex on fertile days. Fertility awareness methods do not work if you do not have regular periods. Infections and some medications can cause changes in vaginal mucus, making some fertility awareness methods harder to use. Unprotected anal, oral, and vaginal sex may raise your chances of getting HIV or other STIs. Withdrawal and avoiding vaginal sex can be used as backup methods during your fertile days. Important Terms Period – the days of your menstrual cycle when you have vaginal bleeding. Menstrual Cycle – the length of time between the start of one period and the next. You ovulate (release an egg) in the middle of your menstrual cycle. You are most fertile on the days around ovulation.