Oadby and Wigston
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Network Rail MHLSI Works.Pub
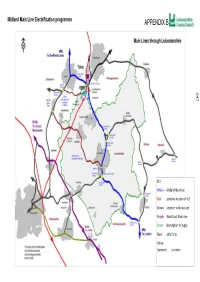
Midland Main Line Electrification programme 247 KEY MMLe — Midland Main Line Red potenal locaon of Hs2 Brown Leicester to Burton Line Purple West Coast Main Line Green Birmingham to ugby Black other lines Yellow diamonds %uncons POST HENDY REVIEW—UPDATE The Hendy Enhancements delivery plan update (Jan 2016) Electrification of the Midland Main Line has resumed under plans announced as part of Sir Peter Hendy’s work to reset Network Rail’s upgrade programme. Work on electrifying the Midland Main Line, the vital long-distance corridor that serves the UK’s industrial heartland, will continue alongside the line-speed and capacity improvement works that were already in hand. Electrification of the line north of Bedford to Kettering and Corby is scheduled to be completed by 2019, and the line north of Kettering to Leicester, Derby/Nottingham and Sheffield by 2023. Outputs The Midland Main line Electrification Programme known as the MMLe is split into two key output dates, the first running from 2014-2019 (known as CP5) and the second, 2019-2023 (CP6). There are a number of sub projects running under the main MMLe programme which are delivering various improvements in the Leicestershire area. Each sub project has dependencies with each other to enable the full ES001- Midland Main Line electrification programme to be achieved A number of interfaces and assumptions link to these programmes and their sub projects will affect Leicestershire. ES001A- Leicester Capacity The proposed 4 tracking between Syston and Wigston is located under sub project ES001A - Leicester Capacity which can be found on page 27 of Network Rails enhancements delivery plan . -

Leicester and Leicestershire City Deal
Leicester and Leicestershire City Deal Page | 1 Executive Summary Leicester and Leicestershire is a diverse and dynamic local economy and its success is integral to driving economic growth in the United Kingdom. The area is home to just under 1 million residents and over 32,000 businesses, many in the manufacturing and logistics sectors. Leicester and Leicestershire also benefits from its location at the heart of the UK road network and close proximity to both the second largest freight handling airport in the UK and London. The area provides employment for 435,000 people and generates an estimated gross value added of £19.4 billion. Despite these strengths Leicester and Leicestershire faces a series of challenges: more than 25,000 jobs were lost between 2008 and 2011 (nearly twice the national average); youth unemployment is relatively high within the city of Leicester and parts of the county; and whilst 70% of small and medium enterprises have plans for growth many find accessing the right type of business support is complex. Some local businesses also note difficulties in filling vacancies. As part of the area’s wider Growth Strategy the City Deal seeks to tackle these key barriers. Over its lifetime the Leicester and Leicestershire Enterprise Partnership expects that the City Deal will deliver: A new employment scheme targeted at 16-24 year olds that will reduce youth unemployment by 50% by 2018, deliver 3,000 new apprenticeships and 1,000 traineeships and work placements. An innovative new employment and training scheme for young offenders. Improved co-ordination of business support services and a range of innovative business support programmes. -

Welcome to the BMC Travel Guide 2020/21
Welcome to the BMC Travel Guide 2020/21 This guide is for all students, staff and visitors! This guide has been created to provide the very best information for all visitors to Brooksby Melton College, whether this is via public transport, car, bicycle or on foot. As part of a vision which holds sustainability and the environment in mind, here at BMC we are always keen to increase travel choice to our staff, students and visitors. This guide provides information on the transport services available across Melton Mowbray and the Leicestershire area to help students and staff to plan their travel routes to college. BMC is situated on two campuses and is well served by a range of buses and trains which makes for simple and easy access. BMC aims to ensure learning opportunities are available and accessible to all of our students wherever you live. This guide will also help staff members to choose their mode of transport; we hope you find this guide useful, informative and helpful when planning your journey to BMC. Brooksby Hall - Brooksby campus Leicestershire’s Choose How You Move campaign helps people to get fit, save money, have fun and help the environment. For further information visit www.leics.gov.uk/ choosehowyoumove Walking to BMC Walking is a great way to stay healthy, help the environment and save money! Walking to BMC can help you keep fit and healthy. Both campuses benefit from good pedestrian links within the surrounding areas, which allows people to find their way to campus easily and safely. Walking 1 mile in 20 minutes uses as much energy as: Running a mile in 10 minutes Cycling for 16 minutes Aerobics for 16 minutes Weight training for 17 minutes Further information is available from: www.leics.gov.uk/index/highways/passenger_ transport/choosehowyoumove/walking.htm Cycling to BMC Cycling is fun and good for you, so get on your bike! Cycle facilities are provided at both campus; including cycle parking, lockers and changing facilities. -

Covid-19-Weekly-Hotspot-Report-For
Weekly COVID-19 Surveillance Report in Leicestershire Cumulative data from 01/03/2020 - 29/09/2021 This report summarises the information from the surveillance system which is used to monitor the cases of the Coronavirus Disease 2019 (COVID-19) pandemic in Leicestershire. The report is based on daily data up to 29th September 2021. The maps presented in the report examine counts and rates of COVID-19 at Middle Super Output Area. Middle Layer Super Output Areas (MSOAs) are a census based geography used in the reporting of small area statistics in England and Wales. The minimum population is 5,000 and the average is 7,200. Disclosure control rules have been applied to all figures not currently in the public domain. Counts between 1 to 5 have been suppressed at MSOA level. An additional dashboard examining weekly counts of COVID-19 cases by Middle Super Output Area in Leicestershire, Leicester and Rutland can be accessed via the following link: https://public.tableau.com/profile/r.i.team.leicestershire.county.council#!/vizhome/COVID-19PHEWeeklyCases/WeeklyCOVID- 19byMSOA Data has been sourced from Public Health England. The report has been complied by Business Intelligence Service in Leicestershire County Council. Weekly COVID-19 Surveillance Report in Leicestershire Cumulative data from 01/03/2020 - 29/09/2021 Breakdown of testing by Pillars of the UK Government’s COVID-19 testing programme: Pillar 1 + 2 Pillar 1 Pillar 2 combined data from both Pillar 1 and Pillar 2 data from swab testing in PHE labs and NHS data from swab testing for the -

Dementia Pilot
Assistive Technology Dementia Pilot January 2020 Information for participants What are we doing? We are running a small pilot project for 50 people to test some new technology designed to help people with dementia living at home. This is something new for the council and we would like to see how it works and understand what the people taking part think about it. We have selected the technology that we are going to use and at the end of the project we will ask you how helpful and easy it was to use. Where are we doing it? The pilot project is a partnership between Leicestershire County Council and five district and borough councils and is for people living in the following areas: • Charnwood • North West Leicestershire • Hinckley and Bosworth • Oadby and Wigston • Blaby What does the technology do? We will be using a product called MySense. This monitors an individual’s activity and daily routine in the home and then communicates the information it collects using the internet. It gathers information using: • Sensors – which can identify movement and activity, e.g. when the bathroom door was opened, or the fridge was used • Smartplug – which connects to the kettle and can indicate when this has been used • Sleep Sensor – which can identify the time at which someone has gone to bed and the time they spent in bed This information is then communicated in the following ways: • App – for family members/friends, which shows a timeline of activity. • Notifications – that a family member/friend will receive by text about the important things you need to know about Do I have to pay for this? No, the council will provide the system to you free of charge during the pilot. -

Oadby and Wigston Borough Information Sheet
Oadby and Wigston Borough Information Sheet Local Council Information and Support Oadby & Wigston Borough Council 40 Bell Street, Wigston, Leicestershire LE18 1ED 0116 2888961 [email protected] Hours: Friday 8:45am–4:15pm Saturday Closed Sunday Closed Monday 8:45am–4:45pm Tuesday 8:45am–4:45pm Wednesday 9:30am–4:45pm Thursday 8:45am–4:45pm Supermarkets and Food Deliveries ASDA – Leicester Road, Oadby Frith, Leicester, LE2 4AH Phone: 0116 2718341 Opening Hours: Mon to Sat 8am - 10pm. Sun 10am – 4pm Sainsbury’s – Leicester Road, Wigston, Leicester, LE18 1JX Phone: 0116 2885571 Opening Hours: Mon to Sun 7am – 9pm Londis – 182 Oadby Road, Wigston, LE18 3PW Phone: 0116 2571391 Foodbanks Food banks are designed to provide short-term, emergency support with food during a crisis. Their aim is to relieve the immediate pressure of the crisis by providing food, while also providing additional support to help people resolve the crises that they face The Kings Centre, http://leicestersouth.foodbank.org. uk/ Mon 56 Bull Head Street, 18:00 - 19:00 Wigston, Tue Leicester, Closed LE18 1PA Wed 07912 194783 http://leicestersouth.foodbank.org.uk/ Mon 18:00 - 19:00 Tue Closed Wed Closed Thu 13:00 - 14:00 Fri Closed Sat Closed Sun Closed When you contact a foodbank direct, inform them you are a PA Housing resident. We have agreements with many foodbanks and it may assist them in deciding whether they can help you. The Trussell Trust covers approximately 75% of the Foodbanks across the UK. If the local numbers can’t provide the help and support you need, try the Trust at https://www.trusselltrust.org/coronavirus-food-banks/ or on 01722 580180. -

Private Residents
AND RU'fLAND. ] PRIVATE RESIDENTS. SNO 657 Sanford Renry Reming, Fair lawn, Sheeter Edward, Fosse villa, Wanlip Slater William Marshall, The Grange, High street, Castle Donington, Derby road, Syston, Leicester Tamworth road, Ashby-de-Ia-Zoucb Sargant W.L. M.A., J.P. School ho. Oakhm Shelbourn Edward, 16 Park road, Mel- Sleath Mrs. High street, Oakham Sarson Mrs. Quorn, Lougbborough ton Mowbray Slee Frederick WaIter,l Nithsdale aven. Saunders Ernest William Cotes M.A. SheIton William Robert,Alexandra villa, Market Harborough High street, Uppingbam Leicester road, Narborough, Leicester Slee H. W. 2 Nithsdale av. Mkt. Rarboro' Saunders Hugb Stanley, Western house, Shenton J. S. Husbands Boswortb,Rgby Sloane Mrs. Townsend road, Enderby, George street, Lutterworth Shepbard John, The Limes, Ravenstone, Leicester Sawyer Rev. Herbert Edward, The Vicar- Ashby-de-Ia-Zouch Smeeton In. J.P. Theddingworth, Rugby age, Asbby-de-Ia-Zouch Shepberd A.J.140 Rerrick rd.Lougbboro' Smeeton Miss, Beech house, Thedding- Saxon S. E. West villa,Kegworth,Derby Sheppard John, Greenfield, Bottesford, worth, Rugby Scarborough Miss, The Laurels, Keg- Nottingham Smeeton Mrs. 44 Coventry road, worth, Derby Sheppard Miss, Manor house, Humber- Market Harborough Schulhof Rev. John Maurice M.A. 58 stone, Leicester Smith Capt. Corbet J.P. Walcote house, Burton road, Melton Mowbray Sheppard Wm. Philpott, Ravenstone Lutterworth Schwabe Alfred J. The Hutch, North- house, Ashby-de-Ia-Zouch Smith Rev. Harry Percival M.A. Rectory, ampton road, Market Harborough Shepperson Mrs. 28 Burton st. Lghboro' Ridlington, Uppingbam Schwind Arthur F. Anker bill, Sbeepy SherilIe Bertie, Wyndham lodge, Ankle Smith Rev. William Fraucis B.A. -

Breakdown of COVID-19 Cases in Leicestershire
Weekly COVID-19 Surveillance Report in Leicestershire Cumulative data from 01/03/2020 - 11/08/2021 This report summarises the information from the surveillance system which is used to monitor the cases of the Coronavirus Disease 2019 (COVID-19) pandemic in Leicestershire. The report is based on daily data up to 11th August 2021. The maps presented in the report examine counts and rates of COVID-19 at Middle Super Output Area. Middle Layer Super Output Areas (MSOAs) are a census based geography used in the reporting of small area statistics in England and Wales. The minimum population is 5,000 and the average is 7,200. Disclosure control rules have been applied to all figures not currently in the public domain. Counts between 1 to 5 have been suppressed at MSOA level. An additional dashboard examining weekly counts of COVID-19 cases by Middle Super Output Area in Leicestershire, Leicester and Rutland can be accessed via the following link: https://public.tableau.com/profile/r.i.team.leicestershire.county.council#!/vizhome/COVID-19PHEWeeklyCases/WeeklyCOVID- 19byMSOA Data has been sourced from Public Health England. The report has been complied by Strategic Business Intelligence in Leicestershire County Council. Weekly COVID-19 Surveillance Report in Leicestershire Cumulative data from 01/03/2020 - 11/08/2021 Breakdown of testing by Pillars of the UK Government’s COVID-19 testing programme: Pillar 1 + 2 Pillar 1 Pillar 2 combined data from both Pillar 1 and Pillar 2 data from swab testing in PHE labs and NHS data from swab testing for the -

COVID 19 Cases in Leicestershire
Weekly COVID-19 Surveillance Report in Leicestershire Cumulative data from 01/03/2020 - 30/12/2020 This report summarises the information from the surveillance system which is used to monitor the cases of the Coronavirus Disease 2019 (COVID-19) pandemic in Leicestershire. The report is based on daily data up to 30th December 2020. The maps presented in the report examine counts and rates of COVID-19 at Middle Super Output Area. Middle Layer Super Output Areas (MSOAs) are a census based geography used in the reporting of small area statistics in England and Wales. The minimum population is 5,000 and the average is 7,200. Disclosure control rules have been applied to all figures not currently in the public domain. Counts between 1 to 7 have been suppressed at MSOA level. An additional dashboard examining weekly counts of COVID-19 cases by Middle Super Output Area in Leicestershire, Leicester and Rutland can be accessed via the following link: https://public.tableau.com/profile/r.i.team.leicestershire.county.council#!/vizhome/COVID-19PHEWeeklyCases/WeeklyCOVID- 19byMSOA Data has been sourced from Public Health England. The report has been complied by Strategic Business Intelligence in Leicestershire County Council. Weekly COVID-19 Surveillance Report in Leicestershire Cumulative data from 01/03/2020 - 30/12/2020 Breakdown of testing by Pillars of the UK Government’s COVID-19 testing programme: Pillar 1 + 2 Pillar 1 Pillar 2 combined data from both Pillar 1 and Pillar 2 data from swab testing in PHE labs and NHS data from swab testing for the -

Vebraalto.Com
76 Leicester Road, Wigston, Leicester, LE18 1DR Telephone: 01162 811 300 • Email: [email protected] www.nestestateagents.co.uk FLOOR PLAN DIMENSIONS Entrance Hall 13'02 xx 5'08 (4.01m xx 1.73m) Lounge 12'11 x 12' (3.94m x 3.66m) Dining Room 9'06 x 8'10 (2.90m x 2.69m) Kitchen 10'10 x 8'10 (3.30m x 2.69m) Downstairs Cloakroom 5'05 x 2'07 (1.65m x 0.79m) Landing Bedroom One 12'10 x 10'02 (3.91m x 3.10m) Bedroom Two 9'06 x 12' (2.90m x 3.66m) Bedroom Three 8'11 x 7'08 (2.72m x 2.34m) Family Bathroom 5'06 x 5'09 (1.68m x 1.75m) FIXTURES AND FITTINGS All items in the nature of the vendors fixtures and fittings unless otherwise indicated in these sales details excluded from the sale. VIEWING Via our office at 76 Leicester Road, Wigston, Leicester, LE18 1DR Telephone: 01162 811 300 • Email: [email protected] who will be pleased to arrange an appointment to view. Or visit our website at www.nestestateagents.co.uk FREE PROPERTY VALUATIONS Looking to sell? Need a valuation? Excellent area coverage local offices all working together to sell your property. Giving one of the most comprehensive displays in Leicester and County – total coverage for your home. Call us on 0116 277 2277 for free advice. OFFER PROCEDURE If you are obtaining a mortgage on this property, one of our qualified mortgage consultants will contact you to qualify the offer on behalf of our vendors. -

Public Transport Map Acocks Green R
WARWICKSHIRE CD INDEX TO PLACES SERVED WARWICKSHIRE BUS SERVICES IN WARWICKSHIRE A L Edingdale Public Transport Map Acocks Green R ............................... B3 Langley............................................. B4 Warwickshire Adderley Park R ............................... A3 Langley Green R .............................. A3 Public Transport Map SERVICE ROUTE DESCRIPTION OPERATOR DAYS OF NORMAL SERVICE ROUTE DESCRIPTION OPERATOR DAYS OF NORMAL 82 R NUMBER CODE OPERATION FREQUENCY NUMBER CODE OPERATION FREQUENCY 7 Alcester ............................................. A5 Lapworth ...................................... B4 June 2016 Clifton Campville Alderminster ...................................... C6 Lawford Heath ...................................D4 Measham Alexandra Hospital ............................. A4 Lea Hall R....................................... B3 March 2017 1/2 Nuneaton – Red Deeps – Attleborough SMR Mon-Sat 15 Minutes 115 Tamworth – Kingsbury – Hurley AMN Mon-Sat Hourly Elford Harlaston Allen End........................................... B2 Lea Marston ...................................... B2 PUBLIC TRANSPORT MAP 82 Allesley ............................................. C3 Leamington Hastings..........................D4 Newton Alvechurch R ................................... A4 Leamington Spa R............................ C4 1/2 P&R – Stratford – Lower Quinton – Chipping Campden – JH Mon-Sat Hourly 116 Tamworth – Kingsbury – Curdworth – Birmingham AMN Mon-Sat Hourly 7 Burgoland 224 Alvecote ........................................... -
1. Introduction
Oadby Town Centre Area Action Plan 1 Baseline Report 1. Introduction 1.1. Taylor Young, in conjunction with BE Group and Faber Maunsell and in association with White Young Green, have been commissioned by Oadby and Wigston Borough Council to undertake an Area Action Plan (AAP) for the town centre of Oadby. This will be prepared fully in accordance with The Town and Country Planning (Local Development) (England) Regulations 2004, and as such will form part of the Council’s Local Development Framework (LDF) in accordance with their Local Development Scheme (LDS). Running in parallel to this work is the preparation of an AAP for Wigston town centre. 1.2. This Baseline Report therefore presents the first of a series of stages that will lead to the production of the Area Action Plan. It also develops a thorough understanding of Oadby and presents an in depth evidence base upon which to move forward and if necessary support the Area Action Plan through examination. 1.3. This has been achieved through a detailed document review of national, regional and local planning policy in relation to town centres, as well as both generic and locally focused reports on retailing and regeneration. This is complemented by a thorough understanding of place – surveys undertaken by Planners, Regeneration Specialists, Urban Designers, Landscape Architects, Transport Specialists, Sustainability Experts and Property Specialists. 1.4. To supplement this and to further the understanding of wider town centre issues, an analysis of census based information has been undertaken to understand the socio- economic position of the catchment for Oadby, and analysis of retail and housing capacity undertaken to support the eventual proposals.