Cholera Surveillance in Bangladesh
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

12578ESIA Report Narayanganj Silo.Pdf
GOVERNMENT OF THE PEOPLES' REPUBLIC OF BANGLADESH MINISTRY OF FOOD DIRECTORATE GENERAL OF FOOD MODERN FOOD STORAGE FACILITIES PROJECT (MFSP) IDA Credit # 5265-BD ENVIRONMENTAL AND SOCIAL IMPACT ASSESSMENT (ESIA) REPORT FOR THE CONSTRUCTION OF GALVANIZED CORRUGATED FLAT BOTTOM STEEL SILO WITH RCC FOUNDATION AND IT'S ANCILLARY WORKS AT NARAYANGANJ SILO SITE PROJECT DIRECTOR MODERN FOOD STORAGE FACILITIES PROJECT PROBASHI KALLAYAN BHABAN, 71-72, ESKATON GARDEN RAMNA, DHAKA-1000, BANGLADESH. OCTOBER, 2019 Modern Food Storage Facilities Project (MFSP), Narayanganj Table of Contents LIST OF TABLES .................................................................................................................... vi ACRONYMS & ABBREVIATIONS...................................................................................... vii EXECUTIVE SUMMARY ...................................................................................................... ix 1. INTRODUCTION ............................................................................................................... 1 1.1. Background ................................................................................................................. 1 1.2. Objectives of the Project ............................................................................................. 2 1.2.1 Strategic Objectives ............................................................................................. 2 1.2.2 Specific Objectives ............................................................................................. -

46399E642.Pdf
PGDS in DOS Myanmar Atlas Map Population and Geographic Data Section As of January 2006 Division of Operational Support Email : [email protected] ((( Yüeh-hsi ((( ((( Zayü ((( ((( BANGLADESHBANGLADESH ((( Xichang ((( Zhongdian ((( Ho-pien-tsun Cox'sCox's BazarBazar ((( ((( ((( ((( Dibrugrh ((( ((( ((( (((Meiyu ((( Dechang THIMPHUTHIMPHU ((( ((( ((( Myanmar_Atlas_A3PC.WOR ((( Ningnan ((( ((( Qiaojia ((( Dayan ((( Yongsheng KutupalongKutupalong ((( Huili ((( ((( Golaghat ((( Jianchuan ((( Huize ((( ((( ((( Cooch Behar ((( North Gauhati Nowgong (((( ((( Goalpara (((( Gauhati MYANMARMYANMAR ((( MYANMARMYANMAR ((( MYANMARMYANMAR ((( MYANMARMYANMAR ((( MYANMARMYANMAR ((( MYANMARMYANMAR ((( Dinhata ((( ((( Gauripur ((( Dongch ((( ((( ((( Dengchuan ((( Longjie ((( Lalmanir Hat ((( Yanfeng ((( Rangpur ((( ((( ((( ((( Yuanmou ((( Yangbi((( INDIAINDIA ((( INDIAINDIA ((( INDIAINDIA ((( INDIAINDIA ((( INDIAINDIA ((( INDIAINDIA ((( ((( ((( ((( ((( ((( ((( Shillong ((((( Xundia ((( ((( Hai-tzu-hsin ((( Yongping ((( Xiangyun ((( ((( ((( Myitkyina ((( ((( ((( Heijing ((( Gaibanda NayaparaNayapara ((((( ((( (Sha-chiao(( ((( ((( ((( ((( Yipinglang ((( Baoshan TeknafTeknaf ButhidaungButhidaung (((TeknafTeknaf ((( ((( Nanjian ((( !! ((( Tengchong KanyinKanyin((( ChaungChaung !! Kunming ((( ((( ((( Anning ((( ((( ((( Changning MaungdawMaungdaw ((( MaungdawMaungdaw ((( ((( Imphal Mymensingh ((( ((( ((( ((( Jiuyingjiang ((( ((( Longling 000 202020 404040 BANGLADESHBANGLADESH((( 000 202020 404040 BANGLADESHBANGLADESH((( ((( ((( ((( ((( Yunxian ((( ((( ((( ((( -

Narayanganj Located in Central Bangladesh, Narayanganj Is Part of Dhaka, with an Area of 760 Square Kilometres
Narayanganj Located in central Bangladesh, Narayanganj is part of Dhaka, with an area of 760 square kilometres. About 34 kilometres away from the nation’s capital, Narayanganj is located on the banks of the Shitalakshya river. It is one of the major hubs of business and industry in Bangladesh, especially for jute trade, processing plants and the textiles sector. Photo credit: BRAC BRAC operates a majority of its programmes in Narayanganj Happy students of BRAC primary school including microfinance, education (BEP), health, nutrition and population (HNPP), water, sanitation and hygiene (WASH), human rights and legal aid services WASH (HRLS), community empowerment At a glance Sanitation coverage 91% (CEP), and gender justice and Deep tubewells installed 171 As of December, 2014 diversity (GJD). Among them Sanitary latrines microfinance largest programme in installed in school 30 the area, covering approximately Microfinance Loans for sanitary latrines 1,896 100,000 clients. Additionally, WASH Village organisation (VOs) 1,670 has achieved 91 per cent sanitation Member 123,463 HRLS coverage in Narayanganj. Borrowers 75,852 Human rights and legal education Progoti (HRLE) shebikas 138 Small enterprise clients 15,050 HRLE graduates 33,671 General information Legal aid clinics 5 BEP Population 2,095,000 Primary schools 460 CEP Pre-primary schools 130 Unions 41 Groups/members 60/3,600 Adolescent development Villages 1,374 Community educators 3,260 programme (ADP) centres 37 Children (0-15) 67,000 Schools/students 40/12,000 Community libraries 31 Primary schools 1,425 Student watch groups/members 40/1,000 Literacy rate 52% HNPP Community watch Hospitals 6 group/members 40/600 NGOs 35 Health workers 117 Health volunteers 1,034 Banks 40 Social enterprises Bazaars 199 Aarong Outlets 1 Although every effort has been made to include and verify the accuracy of relevant information in this fact sheet, users are urged to check independently on matters of specific interest. -

2016Eng. Practice 8 Habiganj Booklet (Spora)
Learning From Hobiganj Health awareness and services UPPR Urban Partnerships for Poverty Reduction 2008-2015 8 About these booklets This series of booklets are case studies of good practice from the Urban Partnerships for Poverty Reduction (UPPR) Project in Bangladesh and form as part of the documentation of the UPPR Learning and Good Practices study conducted by Spora Synergies. The booklets follow a simple, clear structure reflecting on the practices that are seen as examplar and selected through a series of community based participatory workshops, focus group discussions and key interviews. Each case explains [1] The extent to which the practices or the processes developed through UPPR are innovative; [2] The extent to which they were and are sustainable [environmentally, socially and financially]; [3] The extent to which they are transferable and/or have been transferred locally or nationally and; [4] The key reasons explaining their sustainability and their transferability. 1 Savings and credits, Rajshahi 2 Women empowerment, Rajshahi 3 Community Housing Development Fund (CHDF), Gopalgonj 4 Water and sanitation access, Comilla 5 Water and sanitation, Khulna 6 Creation of a new fund for disaster management, Sirajganj 7 Health and apprenticeship, Tangail 8 Health awareness and services, Hobiganj 9 Improve child security and enabling employment of mothers, Mymensingh 10 School attendance improvement, Gazipur 11 Apprenticeship and skill building, Naogaon Acknowledgements Thanks to the Community Development Committee members of Hobiganj for their input and contributions, and to the UNDP PPDU team for their assistance. Urban Partnerships for Poverty Reduction About the Urban Partnerships for Poverty Reduction (UPPR) Project, Bangladesh By developing the capacity of three million urban poor to plan and manage their own development, the Urban Partnerships for Poverty Reduction (UPPR) project enabled the poorest within the nation’s urban slums to break out of the cycle of poverty. -

Disaster Relief Emergency Fund
Bangladesh: DREF operation n° MDRBD004 GLIDE n° TC-2009-000105-BGD 2 June 2009 Cyclone AILA The International Federation’s Disaster Relief Emergency Fund (DREF) is a source of un-earmarked money created by the Federation in 1985 to ensure that immediate financial support is available for Red Cross and Red Crescent response to emergencies. The DREF is a vital part of the International Federation’s disaster response system and increases the ability of national societies to respond to disasters. Cyclone AILA caused extensive damage in south-western Bangladesh, destroying houses, crops and livestock. BDRCS. CHF 253,397 (USD 237,528 or EUR 167,208) has been allocated from the International Federation’s Disaster Relief Emergency Fund (DREF) to support the national society in delivering immediate assistance to some 10,000 families (approximately 50,000 people). Unearmarked funds to repay DREF are encouraged. Summary: Cyclone AILA made landfall in the south western coast of Bangladesh on 25 May 2009. As of 29 May, government figures indicate that 3,709,334 people have been affected in 15 coastal districts, with 147 dead and 1,131 missing. Up to 230,208 houses were reportedly destroyed while those partially damaged stand at 315,018. The amount of damaged crops is estimated to be 340,660 acres. The government, United Nations agencies, international and local non-governmental organizations have been providing relief materials and conducting assessments in the aftermath of the disaster. With time more details of damage are coming to light and the major concern has been that the water sources have been salinated and is not receding. -

Patuakhali Located in the South of Bangladesh, Patuakhali Lies Under Barisal Division and Has an Area of 3,220 Square Kilometres
Patuakhali Located in the south of Bangladesh, Patuakhali lies under Barisal division and has an area of 3,220 square kilometres. Kuakata – the famous beach located at Patuakhali, is also called the “Sagorkonnya” (the daughter of sea). It is the only beach in Bangladesh where both the sunset and sunrise can be seen. The Photo credit: BRAC/Shehzad Noorani Photo credit: two major rivers here are Sitting on a colourful jute matres she participated to paint, a girl child writes in her the Laukathi and Lohalia, textbook in a BRAC primary school in a rural village. which are directly connected with the Bay of Bengal. As disaster management and this city is adjacent to the climate change (DMCC) At a glance programme is also operating in Bay of Bengal, agriculture the area since it is affected by (as of December, 2018) and fishing are the most natural disasters like cyclones, floods and tornadoes each year. Microfinance common professions for the Branches 24 Village organisations 1,457 people of Patuakhali. Members 103,003 Borrowers 36,306 BRAC operates the majority of Progoti Small enterprise clients 5,031 its components at Patuakhali, General information such as microfinance, health, Education nutrition and population (HNPP), Population 1,557,137 Pre-primary schools 28 education (BEP), community Sub-districts 8 ADP centres 25 empowerment (CEP), human Unions 72 Community libraries 40 rights and legal aid services (HRLS), water, sanitation and Villages 882 Children (0-15) 416,689 Human rights and hygiene (WASH), ultra poor legal aid services graduation (UPG) programmes. Primary schools 1,101 Among them, microfinance is the Literacy rate 65% Human rights legal largest programmes, offers three Hospitals 8 education (HRLE) shebikas 339 Legal aid clinics 6 types of loans - dabi (microloan), NGOs 126 HRLE graduates 38,554 progoti (enterprise loan) and Banks 75 Cases filed 361 tenant farmers’ development Bazaars 202 Complaints resolved 2,901 loan (agriculture loan). -
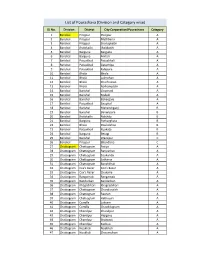
List of Pourashava (Division and Category Wise)
List of Pourashava (Division and Category wise) SL No. Division District City Corporation/Pourashava Category 1 Barishal Pirojpur Pirojpur A 2 Barishal Pirojpur Mathbaria A 3 Barishal Pirojpur Shorupkathi A 4 Barishal Jhalokathi Jhalakathi A 5 Barishal Barguna Barguna A 6 Barishal Barguna Amtali A 7 Barishal Patuakhali Patuakhali A 8 Barishal Patuakhali Galachipa A 9 Barishal Patuakhali Kalapara A 10 Barishal Bhola Bhola A 11 Barishal Bhola Lalmohan A 12 Barishal Bhola Charfession A 13 Barishal Bhola Borhanuddin A 14 Barishal Barishal Gournadi A 15 Barishal Barishal Muladi A 16 Barishal Barishal Bakerganj A 17 Barishal Patuakhali Bauphal A 18 Barishal Barishal Mehendiganj B 19 Barishal Barishal Banaripara B 20 Barishal Jhalokathi Nalchity B 21 Barishal Barguna Patharghata B 22 Barishal Bhola Doulatkhan B 23 Barishal Patuakhali Kuakata B 24 Barishal Barguna Betagi B 25 Barishal Barishal Wazirpur C 26 Barishal Pirojpur Bhandaria C 27 Chattogram Chattogram Patiya A 28 Chattogram Chattogram Bariyarhat A 29 Chattogram Chattogram Sitakunda A 30 Chattogram Chattogram Satkania A 31 Chattogram Chattogram Banshkhali A 32 Chattogram Cox's Bazar Cox’s Bazar A 33 Chattogram Cox's Bazar Chakaria A 34 Chattogram Rangamati Rangamati A 35 Chattogram Bandarban Bandarban A 36 Chattogram Khagrchhari Khagrachhari A 37 Chattogram Chattogram Chandanaish A 38 Chattogram Chattogram Raozan A 39 Chattogram Chattogram Hathazari A 40 Chattogram Cumilla Laksam A 41 Chattogram Cumilla Chauddagram A 42 Chattogram Chandpur Chandpur A 43 Chattogram Chandpur Hajiganj A -

Community Perspectives on Water and Sanitation Towards 'Disaster
Report on “Community Perspectives on Water and SanitationWatSan towards ‘Disaster Risk Reduction (DRR)” Report on Community Perspectives on Water and Sanitation towards ‘Disaster Risk Reduction’ (DRR) For August 2008 Study Conducted by 7/3, Block -A Lalmatia, Dhaka 1207, Bangladesh Phone: +88-02- 9146063, Fax: +88-02-9119459 E-mail:[email protected], [email protected] Web site: www.eminence-bd.org Eminence Page 1 of 56 Report on “Community Perspectives on Water and SanitationWatSan towards ‘Disaster Risk Reduction (DRR)” Study Team Principal Investigator Dr. Md. Shamim H. Talukder Public Health Specialist Chief Executive Eminence Technical Advisors ARMM Kamal Water and Sanitation Specialist Consultant Eminence Haroon Ur Rashid Water, Sanitation and Environmental Specialist Consultant Eminence Dr. Kuntal K Saha Health and Nutrition Specialist Consultant Eminence Research Coordinator S.M Shajedul Haque Palash Shusmita H Khan Team Members Khan Hasibul Hasan Golam Rabbani Jewel Sabia Kamal Dina Farhana Shaima Akter Serajul Islam Eminence Page 2 of 56 Report on “Community Perspectives on Water and SanitationWatSan towards ‘Disaster Risk Reduction (DRR)” Preface In Bangladesh, one-third of the total 140 million populations live below the national poverty line. Furthermore, the intensity of poverty gets worse by high levels of vulnerability due to increasing frequency and magnitude of natural disasters in the coastal areas adjacent to the Bay of Bengal. The common disasters in Bangladesh include floods, cyclones, tornadoes, river erosion, landslides, droughts and earthquakes as well as the affects of these disasters. The situation is further exaggerated by a continuous rise of population and lack of functional community- based disaster management strategies. -

127 Branches
মেটলাইফ পলললির প্রিপ্রিয়াি ও অꇍযাꇍয মপমেন্ট বযা廬ক এপ্রিয়ার িকল শাখায় ꇍগদে প্রদান কমর তাৎক্ষপ্রিকভাদব বমু ে লনন ররপ্রভপ্রꇍউ স্ট্যাম্প ও সীলসহ রিটলাইদের প্ররপ্রসট এই িলু বধা পাওয়ার জনয গ্রাহকমক মকান অলিলরক্ত লফ অথবা স্ট্যাম্প চাজ জ প্রদান করমি হমব না Sl. No. Division District Name of Branches Address of Branch 1 Barisal Barisal Barishal Branch Fakir Complex 112 Birshrashtra Captain Mohiuddin Jahangir Sarak 2 Barisal Bhola Bhola Branch Nabaroon Center(1st Floor), Sadar Road, Bhola 3 Chittagong Chittagong Agrabad Branch 69, Agrabad C/ A, Chittagong 4 Chittagong Chittagong Anderkilla Branch 184, J.M Sen Avenue Anderkilla 5 Chittagong Chittagong Bahadderhat Branch Mamtaz Tower 4540, Bahadderhat 6 Chittagong Chittagong Bank Asia Bhaban Branch 39 Agrabad C/A Manoda Mansion (2nd Floor), Holding No.319, Ward No.3, College 7 Chittagong Comilla Barura Branch Road, Barura Bazar, Upazilla: Barura, District: Comilla. 8 Chittagong Chittagong Bhatiary Branch Bhatiary, Shitakunda 9 Chittagong Brahmanbaria Brahmanbaria Branch "Muktijoddha Complex Bhaban" 1061, Sadar Hospital Road 10 Chittagong Chittagong C.D.A. Avenue Branch 665 CDA Avenue, East Nasirabad 1676/G/1 River City Market (1st Floor), Shah Amant Bridge 11 Chittagong Chaktai Chaktai Branch connecting road 12 Chittagong Chandpur Chandpur Branch Appollo Pal Bazar Shopping, Mizanur Rahman Road 13 Chittagong Lakshmipur Chandragonj Branch 39 Sharif Plaza, Maddho Bazar, Chandragonj, Lakshimpur 14 Chittagong Noakhali Chatkhil Branch Holding No. 3147 Khilpara Road Chatkhil Bazar Chatkhil 15 Chittagong Comilla Comilla Branch Chowdhury Plaza 2, House- 465/401, Race Course 16 Chittagong Comilla Companigonj Branch Hazi Shamsul Hoque Market, Companygonj, Muradnagar J.N. -

Bangladesh GAP ANALYSIS
GAP ANALYSIS Cyclone Amphan/Waterlogging Response 2020, Bangladesh NeedsAssessment Working Group (NAWG), Bangladesh Date-November 21, 2020 About the Working Group: The Needs Assessment Working Group (NAWG) is a platform for government and non-government humanitarian agency under Humanitarian Coordination Task Team (HCTT). The secretariat of the Working Group is hosted by CARE Bangladesh, “Supporting Bangladesh Rapid Needs Assessment (SUBARNA) Project.” For Regular Updates: https://www.humanitarianresponse.info/en/operations/bangladesh/needs- assessment-working-group Fund Managed By Funded By Implemented By Disclaimer: This material has been funded by UK aid from the UK government, however the views expressed do not necessarily reflect the UK government’s official policies. GAP Analysis_ Cyclone Amphan/Waterlogging response 2020 NAWG, BANGLADESH Background: On May 2020, devastating cyclone Amphan made landfall in Jammu island near west Bengal at afternoon with a wind speed about 140 km per hour, took life of 26 people while 7 people injured and this cyclone affected about 10 million people from 19 districts of Bangladesh (Response Plan for Cyclone Amphan).As reported by the Ministry of Disaster Management &Relief about 55 thousand houses totally damaged where about 3 lakhs houses damaged partially and about 100,000 people were displaced (Response Plan for Cyclone Amphan). As per report of National authority, Cyclone Amphan caused infrastructural damage of US$ 130 million which includes damage of electricity network, school building, bridges and road network, damages of water source, embankments etc. Among all districts 9 districts affected severally; which are Khulna, Satkhira, Barguna, Bhola, Patuakhali, Pirojpur, Noakhali, Bagerhat and Jessore. Humanitarian coordination task team (HCTT) formulateda Response Plan for Cyclone Amphan focusing the sectoral need on priority basis by mentioning the geographical coverage of 7 districts in terms of severity with funding request of US$ 25M for response to cyclone Amphan. -

The Situation Information Bulletin Bangladesh: Floods and Landslides
Information Bulletin Bangladesh: Floods and Landslides Information Bulletin n° 1 GLIDE n° FL-2012-000106-BGD 29 June 2012 Text box for brief photo caption. Example: In February 2007, the This bulletin is being issued for information Colombian Red Cross Society distributed urgently needed materials after the floods and slides in Cochabamba. IFRC (Arial only, and reflects the current situation and 8/black colour) details available at this time. The Bangladesh Red Crescent Society (BDRCS), with the support of the International Federation of Red Cross and Red Crescent Societies (IFRC), has determined funding from its internal sources to mobilize emergency response to the affected areas. No external assistance has been requested at this time. Bangladesh Red Crescent Society (BDRCS) volunteers in search and rescue operation in Chittagong mud slide on 27 June 2012. Photo: BDRCS. The situation Monsoon rains starting 25 June in southeast and northeast Bangladesh resulted in flash floods and landslides causing at least 100 deaths. Damage has been most severe in the southeast districts of Chittagong, Cox’s Bazar, and Bandarban and in the northeast district of Sylhet. Landslides, collapsed houses, drowning and lightning following torrential rains on 27 June caused further damages and loss of lives in Cox's Bazar, Chittagong, Bandarban and Sylhet. Thousands of people remain stranded in low-lying areas and many communities in the Chittagong Hill Tracts are still unreachable due to the landslides. Many areas are cut off from the rest of the country as roads and railway tracks are unusable due to the floods and landslides. Displaced people in the affected districts of Cox’s Bazar, Chittagong, Bandarban, Feni, Sylhet, Habiganj and Sunomganj are residing on road sides, schools and colleges, and need shelter, food, clean water and medical care. -
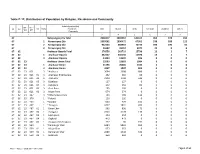
Table C-13: Distribution of Population by Religion, Residence and Community
Table C-13: Distribution of Population by Religion, Residence and Community Administrative Unit UN / MZ / ZL UZ Vill RMO Residence Total Muslim Hindu Christian Buddhist Others WA MH Community 1 2 3 4 5 6 7 8 67 Narayanganj Zila Total 2948217 2802567 144105 963 378 204 67 1 Narayanganj Zila 1959261 1890472 67951 538 188 112 67 2 Narayanganj Zila 942354 868943 72733 396 190 92 67 3 Narayanganj Zila 46602 43152 3421 29 0 0 67 02 Araihazar Upazila Total 376550 363733 12796 13 1 7 67 02 1 Araihazar Upazila 362127 350136 11970 13 1 7 67 02 3 Araihazar Upazila 14423 13597 826 0 0 0 67 02 23 Araihazar Union Total 25593 23603 1984 6 0 0 67 02 23 1 Araihazar Union 21196 20006 1184 6 0 0 67 02 23 3 Araihazar Union 4397 3597 800 0 0 0 67 02 23 021 3 *Araihazar 3694 3008 686 0 0 0 67 02 23 021 01 3 Araihazar Krishnapura 262 202 60 0 0 0 67 02 23 021 02 3 Araihazar 2294 1748 546 0 0 0 67 02 23 021 03 3 Dighirpar 127 127 0 0 0 0 67 02 23 021 04 3 Debipura 242 162 80 0 0 0 67 02 23 021 05 3 Goal Para 195 195 0 0 0 0 67 02 23 021 06 3 Nagar Para 574 574 0 0 0 0 67 02 23 247 3 *Chhota Barai Para 703 589 114 0 0 0 67 02 23 376 1 *Faitadi 126 126 0 0 0 0 67 02 23 403 1 *Gazipur 693 494 199 0 0 0 67 02 23 467 1 *Jhaugara 4237 3831 400 6 0 0 67 02 23 467 01 1 Binar Char 963 890 73 0 0 0 67 02 23 467 02 1 Jhaugara 2320 2178 136 6 0 0 67 02 23 467 03 1 Lakhupura 254 254 0 0 0 0 67 02 23 467 04 1 Dighaldi 473 473 0 0 0 0 67 02 23 467 05 1 Jhaugara Krishnapura 227 36 191 0 0 0 67 02 23 559 1 *Kamrangir Char 6384 5833 551 0 0 0 67 02 23 559 01 1 Majar Char 553