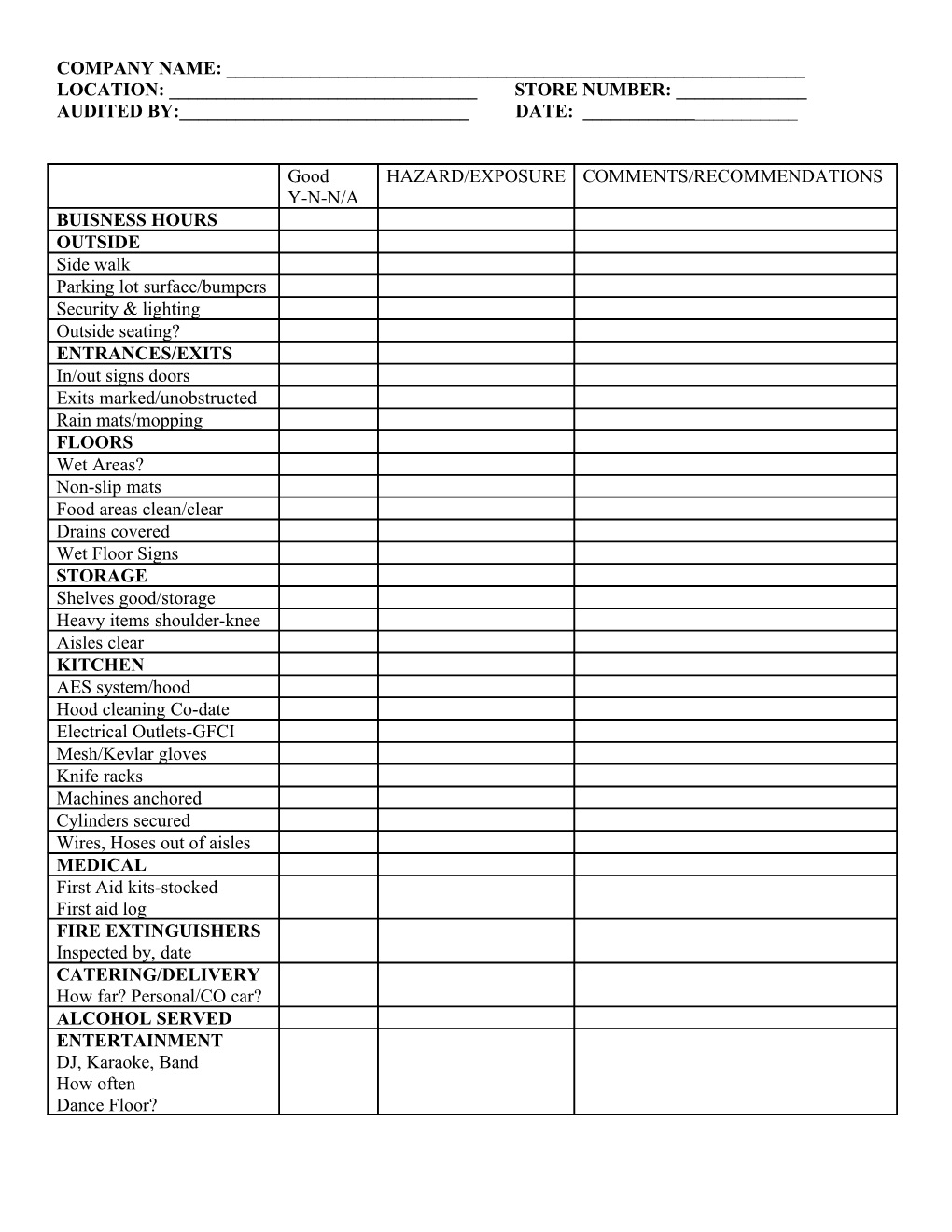
COMPANY NAME: ______LOCATION: ______STORE NUMBER: ______AUDITED BY:______DATE: ______
Good HAZARD/EXPOSURE COMMENTS/RECOMMENDATIONS Y-N-N/A BUISNESS HOURS OUTSIDE Side walk Parking lot surface/bumpers Security & lighting Outside seating? ENTRANCES/EXITS In/out signs doors Exits marked/unobstructed Rain mats/mopping FLOORS Wet Areas? Non-slip mats Food areas clean/clear Drains covered Wet Floor Signs STORAGE Shelves good/storage Heavy items shoulder-knee Aisles clear KITCHEN AES system/hood Hood cleaning Co-date Electrical Outlets-GFCI Mesh/Kevlar gloves Knife racks Machines anchored Cylinders secured Wires, Hoses out of aisles MEDICAL First Aid kits-stocked First aid log FIRE EXTINGUISHERS Inspected by, date CATERING/DELIVERY How far? Personal/CO car? ALCOHOL SERVED ENTERTAINMENT DJ, Karaoke, Band How often Dance Floor?