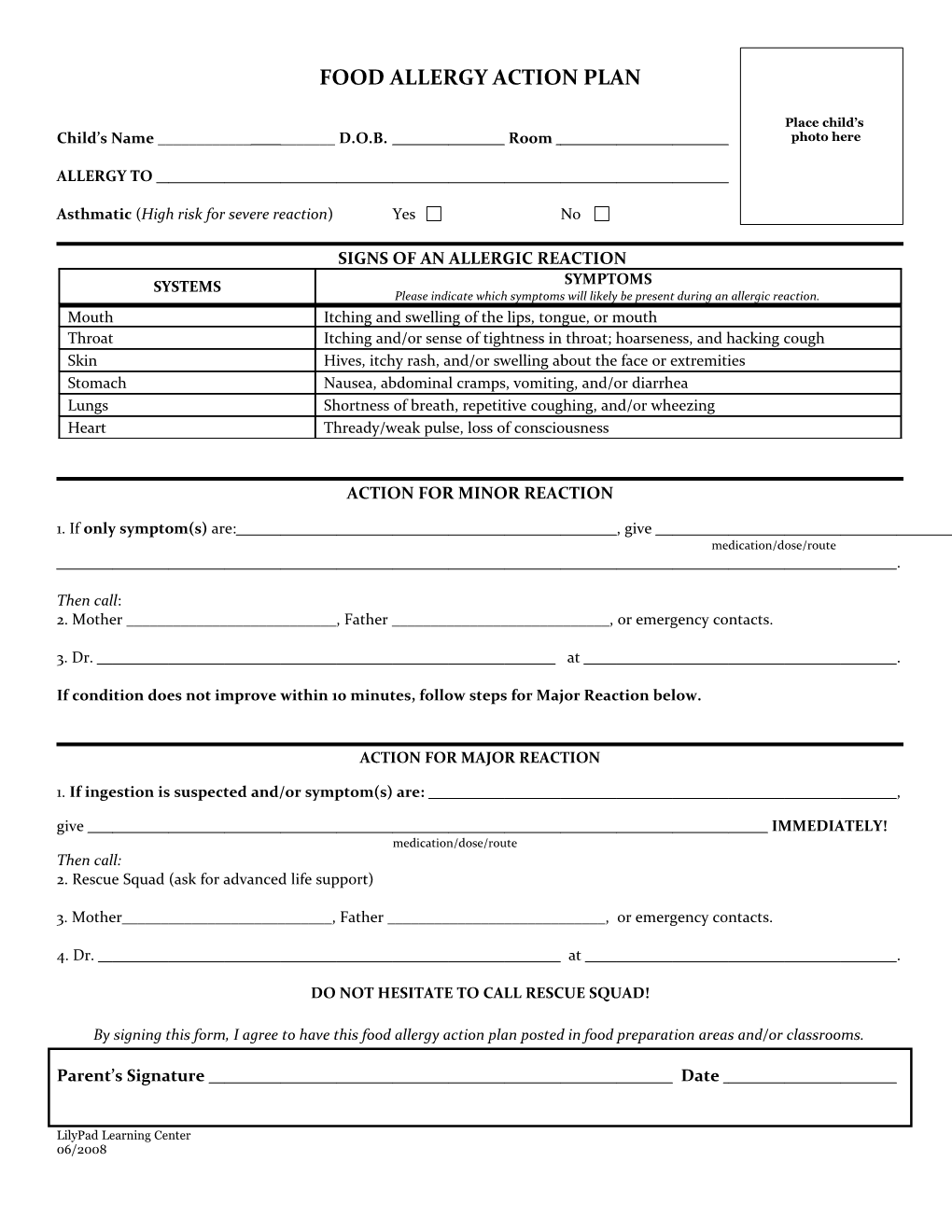
FOOD ALLERGY ACTION PLAN
Place child’s Child’s Name ______D.O.B. Room photo here
ALLERGY TO
Asthmatic (High risk for severe reaction) Yes No
SIGNS OF AN ALLERGIC REACTION SYSTEMS SYMPTOMS Please indicate which symptoms will likely be present during an allergic reaction. Mouth Itching and swelling of the lips, tongue, or mouth Throat Itching and/or sense of tightness in throat; hoarseness, and hacking cough Skin Hives, itchy rash, and/or swelling about the face or extremities Stomach Nausea, abdominal cramps, vomiting, and/or diarrhea Lungs Shortness of breath, repetitive coughing, and/or wheezing Heart Thready/weak pulse, loss of consciousness
ACTION FOR MINOR REACTION
1. If only symptom(s) are: , give medication/dose/route .
Then call: 2. Mother ______, Father ______, or emergency contacts.
3. Dr. at .
If condition does not improve within 10 minutes, follow steps for Major Reaction below.
ACTION FOR MAJOR REACTION
1. If ingestion is suspected and/or symptom(s) are: , give IMMEDIATELY! medication/dose/route Then call: 2. Rescue Squad (ask for advanced life support)
3. Mother______, Father ______, or emergency contacts.
4. Dr. at .
DO NOT HESITATE TO CALL RESCUE SQUAD!
By signing this form, I agree to have this food allergy action plan posted in food preparation areas and/or classrooms.
Parent’s Signature Date
LilyPad Learning Center 06/2008 Doctor’s Signature Date
LilyPad Learning Center 06/2008