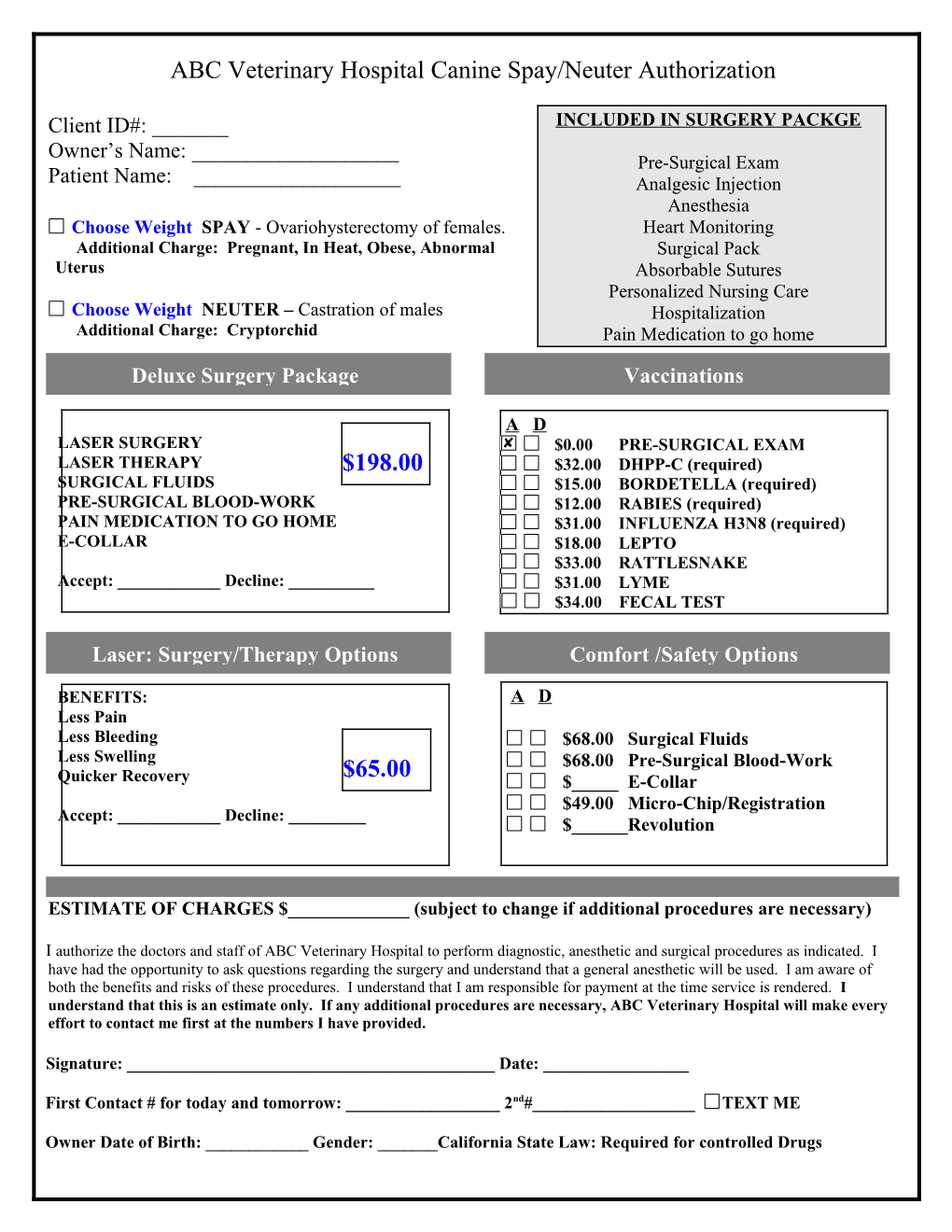
ABC Veterinary Hospital Canine Spay/Neuter Authorization
Client ID#: ______INCLUDED IN SURGERY PACKGE Owner’s Name: ______Pre-Surgical Exam Patient Name: ______Analgesic Injection Anesthesia Choose Weight SPAY - Ovariohysterectomy of females. Heart Monitoring Additional Charge: Pregnant, In Heat, Obese, Abnormal Surgical Pack Uterus Absorbable Sutures Personalized Nursing Care Choose Weight NEUTER – Castration of males Hospitalization Additional Charge: Cryptorchid Pain Medication to go home
Deluxe Surgery Package Vaccinations
A D LASER SURGERY $0.00 PRE-SURGICAL EXAM LASER THERAPY $198.00 $32.00 DHPP-C (required) SURGICAL FLUIDS $15.00 BORDETELLA (required) PRE-SURGICAL BLOOD-WORK $12.00 RABIES (required) PAIN MEDICATION TO GO HOME $31.00 INFLUENZA H3N8 (required) E-COLLAR $18.00 LEPTO $33.00 RATTLESNAKE Accept: ______Decline: ______$31.00 LYME $34.00 FECAL TEST
Laser: Surgery/Therapy Options Comfort /Safety Options
BENEFITS: A D Less Pain Less Bleeding $68.00 Surgical Fluids Less Swelling $68.00 Pre-Surgical Blood-Work $65.00 Quicker Recovery $_____ E-Collar $49.00 Micro-Chip/Registration Accept: ______Decline: ______$______Revolution
ESTIMATE OF CHARGES $______(subject to change if additional procedures are necessary)
I authorize the doctors and staff of ABC Veterinary Hospital to perform diagnostic, anesthetic and surgical procedures as indicated. I have had the opportunity to ask questions regarding the surgery and understand that a general anesthetic will be used. I am aware of both the benefits and risks of these procedures. I understand that I am responsible for payment at the time service is rendered. I understand that this is an estimate only. If any additional procedures are necessary, ABC Veterinary Hospital will make every effort to contact me first at the numbers I have provided.
Signature: ______Date: ______
First Contact # for today and tomorrow: ______2nd#______TEXT ME
Owner Date of Birth: ______Gender: ______California State Law: Required for controlled Drugs