Is the use of fluoride toothpaste optimal? Knowledge, attitudes and behaviour concerning fluoride toothpaste and toothbrushing in different age groups in Sweden
OLGA JENSEN1,2, PIA GABRE2,3, ULLA MOBERG SKÖLD2, DOWEN BIRKHED2,
1Public Dental Health, Västra Götaland Region, Gothenburg, Sweden, 2Department of Cariology, Institute of Odontology, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden, 3Public Dental Health, Uppsala County Council, Uppsala, Sweden
Key words: attitudes, behaviour, dental caries, fluoride toothpaste, knowledge, oral health, toothbrushing
Corresponding author: Olga Jensen Folktandvården Strandvägen 17 444 31 Stenungsund Telephone: +46 303 726409 E-mail: [email protected]
1 Abstract
Objectives: The most effective method to prevent caries is regular use of fluoride toothpaste.
The aim of this study was to evaluate self-care routines in a population by identifying knowledge, attitudes and behaviour relating to fluoride toothpaste and toothbrushing habits.
Methods: A questionnaire was sent to 3,200 individuals in two municipalities in Sweden. Four age groups representing different life stages were chosen: 15-16, 31-35, 61-65 and 76-80 years of age. The participants were selected from the population register by random selection of birth dates.
Results: Totally 2,023 (63%) individuals answered the questionnaire. The majority (84-94%) in all age groups brushed their teeth twice a day or more often. Good toothpaste behaviour identified as brushing at least twice a day, using at least 1 centimetre toothpaste, brushing two minutes or longer and using a small amount of water when rinsing was reported by only 10% of the respondents. The factors that increased the odds for having good caries preventive behaviour were: 1) being female, 2) younger than 35 years, 3) having knowledge about fluoride, 4) finding use of fluoride toothpaste important, and 5) rating own oral health as good.
Conclusion: The population seems to have embraced regular toothbrushing with fluoride toothpaste to a large extent. However, regarding techniques for using fluoride toothpaste effectively there was great potential for improvement, especially among the older respondents.
2 Introduction
Dental caries has successively declined in recent decades, mainly thanks to the positive effect of fluoride in toothpaste (1, 2). Other preventive measures such as fluoride rinsing and gels have also played a role (3-5). However, there are now signs of a global increase in dental caries (6). One explanation may be that there has been a worldwide change in lifestyle towards increased sugar consumption (7).
The most effective method for preventing caries is use of fluoride toothpaste twice a day
(1,8). The main factors for positive effect of fluoride toothpaste are toothbrushing frequency, fluoride concentration in the toothpaste, the amount of toothpaste used, brushing time and subsequent water rinsing (9-12). Children who brush their teeth with fluoride toothpaste regularly are more likely to avoid tooth decay than children with irregular oral hygiene habits
(13). Despite this knowledge, two independent Nordic studies show that about 25% of 14- year-old adolescents do not brush their teeth regularly (14-15).
People’s oral health behaviour is influenced by several factors, such as socio-economic status, knowledge about and attitudes towards oral health (16-17). Previous results show that toothbrushing habits are strongly influenced by an individual's lifestyle and social behaviour
(18). Oral hygiene routines among Finnish 11- to12-year-olds were dependent on knowledge, attitudes and beliefs (19). Oral healthcare education can increase an individual's knowledge of and attitude towards oral health and improve their behaviour and brushing techniques, although changes in behaviour are difficult to maintain (20-21).
Few studies describe toothbrushing habits among adults. In a study by Hugoson et al., however, 90% of Swedish adults stated that they brushed once or twice a day (22). In Finland,
3 47% of the men and 79% of the women reported toothbrushing at least twice a day, while daily use of fluoride toothpaste was reported by 86% and 96%, respectively (23). In a recently published Swedish study among adults, 95% of the participants stated that they brushed twice per day, fluoride toothpaste was used by almost all and about 75% rinsed with water after brushing. On contrast, only 9% rinsed with toothpaste slurry after brushing (24). The brushing time was reported to be long in this observation study since almost half of the participants brushed two minutes or longer, a result contradicted in a study by Saxer et al. (25) where observed brushing time was just over one minute. That study concluded that brushing technique, post-brushing behaviour and use of fluoride toothpaste among the participants were not optimal and health education was needed to optimize the use of fluoride toothpaste
(24).
The hypothesis of this study was that increased knowledge of the benefits of fluoride toothpaste and the most effective technique to achieve caries reduction may affect the population's behaviour in using fluoride toothpaste. Thus, the aim of this investigation was to gain knowledge about a self-care design in a population by identifying knowledge, attitudes and behaviour concerning fluoride toothpaste and brushing habits among adolescents, adults and the elderly.
Materials and Methods
The Ethics Committee in Gothenburg, Sweden approved the study. Consent was obtained through a covering letter accompanying the questionnaire. When a completed questionnaire was returned it was considered as consent.
4 The questionnaire
A questionnaire was used to gain insight into knowledge, attitudes and behaviour about dental care habits among adolescents, adults and the elderly in two municipalities in Sweden:
Stenungsund and Enköping. The questionnaire consisted of 28 questions generated from initial interviews with people in current ages. Before the questionnaire was definitely established the questions were tested on a small group of individuals. The questionnaire consisted of multiple choice questions and a VAS scale was used in one question (26).
Study population
The questionnaire was sent to a total of 3,200 individuals, 1,600 in Stenungsund and 1,600 in
Enköping. The two municipalities were selected because they are similar in size and socio- economic structure and situated far from each other. An intervention aiming to influence knowledge and behaviour concerning toothbrushing is planned later for Stenungsund and in that phase of the study the population of Enköping will serve as a control group. In the present study, however, both municipalities are considered as one population with a cross-sectional design. Four age groups, representing different stages in life, were chosen: 15-16, 31-35, 61-
65 and 76-80.
The selection of the participants was based on randomly selected birth dates. The birth dates were chosen by lot and all individuals born on certain days of the months were included in the study. Since the municipalities and the age groups did not have exactly the same size of population, the number of randomly selected birth dates varied, but in each municipality and in each age group 400 participants were chosen. All four age groups completed the same questionnaire. A flow chart of the study is shown in Figure 1.
5 Data collection and data processing
The questionnaire was sent by post together with a postage-paid return mailer. A toothbrush was attached to the questionnaire in order to increase the response rate. If an envelope came back from the post office marked as “address unknown” or “deceased,” a new person was selected from the random list and a new questionnaire was sent. After 3 weeks, a reminder was sent to those who had not responded. The questionnaires were marked with an identification code, a number which indicated the person’s age group and municipality and their number on the list. This was done in order to be able, if necessary, to recall responses, as well as to do a longitudinal follow-up after the intervention study. The answers were entered unidentified in a database for analysis. A manual for data input was created by two of the authors (OJ and PG) when registered 20 questionnaires together. In cases where the respondents made more than two marks, despite the instruction to use only one, the first item in order was registered. If the respondents answered that they used both a fluoride mouthwash and another mouthwash not containing fluoride, the one with the fluoride was registered because of the importance for avoiding caries. Anonymous responses were included if the right age group could be identified. The data were transferred to the database by two secretaries and one of the authors (OJ). The answer “Do not know” was registered as a response in questions concerning knowledge. In other contexts the answer was considered as a missing answer. All transmitted data were subsequently verified by one of the authors (OJ).
Good toothpaste behaviour
A variable “Good toothpaste behaviour” was constructed by identifying those who showed the following behaviour: 1. Brushing twice a day or more often, 2. Using one centimetre toothpaste or more or putting toothpaste on the electric brush twice, 3. Brushing two minutes or longer, and 4. Using no more than a handful of water for the post-brushing rinse. The
6 association between “Good toothpaste behaviour” and a number of registered data in the study was analysed.
Statistical analysis
The size of the sample was determined by a statistician in this study with the purpose of having a sufficient number of participants to be able to investigate differences between the groups after the intervention. The number of participants was counted to be 150 respondents in each age group and from each municipality to provide the opportunity to detect improvements of 20% in knowledge and behaviour when comparing the results before and after the intervention. Given that 400 people would receive the questionnaire, the study design had good margins for drop-outs. Twenty randomly selected questionnaires were chosen and verification of the transmitted data was made on individual and group levels. The quality controls of the transfer process showed a margin of error of 0.004. Descriptive analyses of the answers to the questionnaires were shown in frequency tables. The frequency distributions were analysed with chi-square tests. A p-value of <0.05 was considered statistically significant.
Results
A total of 63% answered the questionnaire, with the highest frequency of answers among the age-group 61-65 years (75%), followed by 76-80 years (66%). More women than men participated in the study (Fig. 1). The 15- to 16-year-olds had all finished secondary school.
Among the 31-35-year-olds, 61% had post upper secondary school education. Among the 61-
65 and 76-80-year-olds, the corresponding figures were 40% and 30%, respectively.
7 Knowledge
Knowledge concerning fluoride toothpaste, caries and toothbrushing is shown in Table 1. The majority of the individuals expressed the opinion that the main effect of fluoride was “to strengthen the teeth”. More teenagers than older participants did not know the effect of fluoride in toothpaste and more thought that fluoride “made the teeth whiter”. Few respondents stated that toothpaste was the most important tool to avoid caries, although more teenagers chose that answer than the older age groups. A vast majority stated that they had received no instructions about how to use toothpaste and this answer was more frequent the older the respondents were. When the respondents had received instructions, dental personnel were the dominant instructors. Twenty percent of the 15- to 16-year-olds answered that they had no knowledge if their toothpaste contained fluoride or not, while other age groups stated that they knew that their toothpaste was fluoridated (95-96%, P <0.0001).
Attitudes
Attitudes concerning fluoride toothpaste and toothbrushing are presented in Table 2. Almost all respondents in all the age groups thought that brushing was “very important” or “quite important” and they had the same opinion about brushing with toothpaste. When choosing toothpaste, taste was the most important factor among the three oldest age groups. Teenagers stated that they used whatever toothpaste was available at home. Most respondents of all ages stated that “healthy teeth” was most important, followed by “no cavities”. One third of the adolescents considered “white teeth” as important, an alternative seldom used by older respondents. The participants described how they experienced their oral health by marking a visual scale with the endpoints “Good” and “Bad”. Several individuals in the two oldest age groups did not answer the question (10 and 22% respectively). A large proportion estimated
8 their oral health as good, with the oldest age group choosing this assessment to a greater extent (Fig. 2; P <0.05).
Behaviour
Results concerning fluoride toothpaste and toothbrushing behaviour are presented in Table 3.
The majority in all age groups brushed twice a day with the highest frequency, 91%, for the
31- to 35-year-olds and the lowest frequency, 66%, for the 76- to 80-year-olds. The older the participants were, the greater the risk of just brushing once a day. The most common brushing pattern was “after breakfast” and “before going to bed”, but the older the respondent was the greater the risk was of brushing before breakfast and after dinner. Most, 74%, of those who stated that they brushed just once a day brushed “before going to bed”.
Of those who stated brushing twice per day, 65% of the 15- to 16-year-olds reported that it happened that they did not brush their teeth twice a day. The older the respondent, the less likely it was that they sometimes did not brush twice a day (40%, 20% and 16% respectively, p<0.0001). Several respondents (8-26%) stated that they sometimes brushed without toothpaste and respondents in the oldest age group were the most likely to do so (P <0.0001).
The majority did not eat, drink or take medicines after brushing their teeth, but 27% of the respondents stated that they had some intake. There were no statistically significant differences between the age groups. The oldest age group more often took medicines after evening toothbrushing (data not shown, P <0.001).
More than 50% of the individuals in the different age groups brushed their teeth for less than two minutes. Most participants stated that they used one centimetre of toothpaste on a regular toothbrush and the youngest age-group more often used a larger amount of toothpaste. When
9 an electric toothbrush was used, the vast majority, irrespective of age, put toothpaste on the brush just once (81-87%, data not shown). The majority in all age groups dipped the brush in water during brushing. However, older respondents dipped more frequently and used more water when rinsing after brushing than younger respondents.
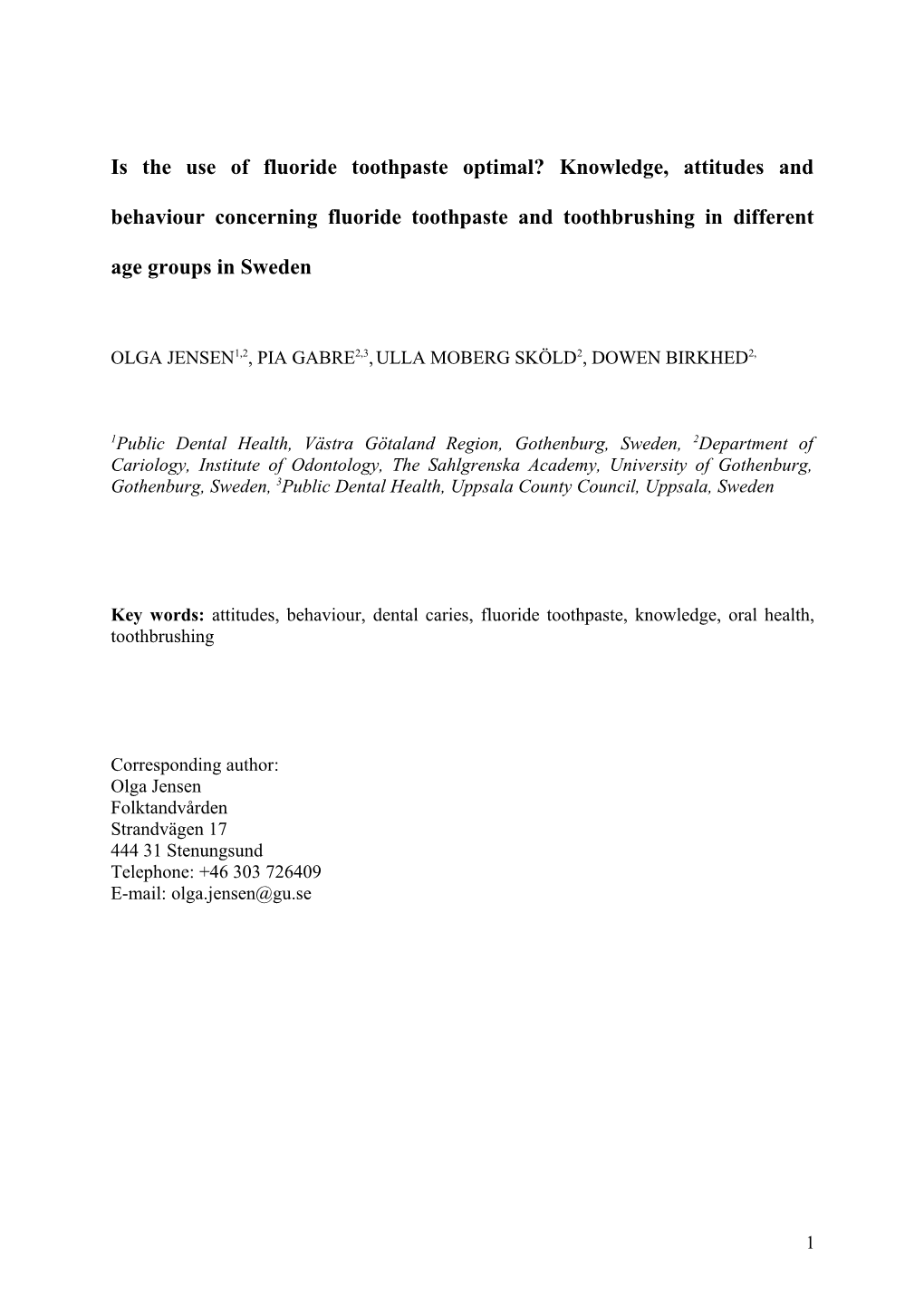
Factors that increased the chance of having “Good toothpaste behaviour” were being female, age less than 35, with the knowledge that fluoride strengthens the teeth, believing that brushing with fluoride toothpaste is important and rating one’s own oral health as good (Fig.
3).
Oral hygiene habits concerning toothbrushing, interdental aids and use of mouthwash are presented in Table 4. The majority in all age groups used a regular toothbrush, but use of an electric toothbrush, alone or in combination with a regular one, was also common, especially in the age group 61-65. Interdental aids were used more frequently among the age group 31-
35 and less frequently among the youngest respondents. The majority reported that they did not use mouthwash, and among those who used mouthwash the use of a fluoride rinse was most common.
Discussion
This study shows that good toothpaste technique and good toothbrushing behaviour, identified as brushing twice a day or more often, using sufficient amount of toothpaste, brushing two minutes or longer and using no more than a handful of water when rinsing was reported by only 10% of the respondents. Respondents under 35 showed the best behaviour and the oldest age group the worst. Knowledge about fluoride, considering use of fluoride toothpaste important and rating one’s own oral health as good increased the odds of having good caries
10 preventive behaviour. In addition, women, more often than men showed this positive behaviour.
The response rate was high, especially in the older groups. Women responded more often than men. The response patterns agree with previous frequently reported experience; lower response rates from young people and men. Since women had more favourable oral hygiene habits the response rate could have given a more positive picture of people’s habits than was actually true. However, respondents in the older age groups showed worse oral hygiene than the younger ones. The over-representation of the elderly could therefore give a picture of worse toothbrushing habits in the population than reflected in reality.
The level of knowledge on the effect of fluoride in toothpaste was high amongst the respondents although the oldest age group had less knowledge than the younger ones. Despite the knowledge about fluorides most of the individuals believed fluoride toothpaste and toothbrushing were equally important for preventing caries. Knowledge related to oral health has been investigated previously in Sweden. Hugoson et al. (22) reported that 73% of the 15- year-olds knew that fluoride strengthen the teeth, as compared to 75% in the present study.
Hedman et al. (17) also reported sufficient knowledge about fluoride and girls had better knowledge than boys. In our study, few respondents reported that they had been taught how to use toothpaste, and if they had received such information dental personnel were the main source. A previous study also concluded that people are not aware of how to use toothpaste in a rational way (24).
The majority of the respondents, 84-94%, answered that they brushed their teeth twice a day, which is in accordance with other Swedish studies (22, 24) and better than the results from a recently published study in Finland (23). The oldest age group showed the highest proportion of individuals who brushed just once a day or less. Low brushing frequency not only increases
11 the risk of developing caries (1, 8) but also increases the risk of not having regular dental care
(27). A third daily toothbrushing also increases the fluoride concentration in saliva and plaque and seems therefore to have potential to further prevent caries (28). For those who brushed once a day, especially if it was irregular brushing in the evening, this was associated with high caries prevalence (29). In this study 74% of the subjects who stated that they brushed once a day did their brushing in the evening. Just under half of the respondents brushed their teeth for 2 minutes or longer, and among the 76- to 80-years-olds, only 34% stated this duration of brushing. The result is in line with the study by Saxer et al. (25) but differs from the duration reported in a Swedish study (24). Brushing duration from 30 seconds to 3 minutes was evaluated by Zero et al. (12). Longer brushing time reduced retention of toothpaste in the brush, leading to both higher and prolonged fluoride levels in the mouth. The amount of toothpaste on the brush has been described as both insignificant and important (12, 30). The latter study found that increasing the amount from 0.5g to 1.5g more than doubled the fluoride content in saliva after brushing. In our study, about one quarter of the respondents stated that they used a large amount, 2 centimetres of toothpaste, which corresponds to 1-1.5g. In contrary, those who used an electric toothbrush risk of using too small an amount of toothpaste, since 81-87% of them stated that they only put toothpaste on the brush once.
The majority of the participants stated that they dipped the brush in water during brushing.
Dipping the brush was more common among the oldest age groups. To dip the brush in water means that fluoride toothpaste is rinsed off and less fluoride in the toothpaste reaches the teeth. Rinsing with water after brushing was common and especially among the oldest group a large amount of water was used since half of the elderly people stated that they used a half glass of water or more. The subsequent rinsing with water after brushing is of importance for caries prevention (10-11). The most common pattern for brushing was after breakfast and
12 before going to bed. On contrast, 23% of the 76- to 80-year-olds stated that they brushed before breakfast.
No correlations between level of education and toothbrushing habits could be seen in this study. Such relationships have been reported in other studies. In adolescents, toothbrushing habits have been found to be strongly associated with lifestyle factors and education (15) and in a study of adults in Finland, an association between number of years of education and toothbrushing habits was found (31). However, the latter study reports that the association between sense of coherence and more favourable oral health habits was even stronger. Self- perceived oral health and attitudes to oral health were associated with good toothbrushing behaviour. This is in line with studies of both adolescents and older individuals (27, 32).
However, the latter study reports that 75-year-olds estimated their oral health as worse than the ten-year younger individuals. In our study, the opposite was found. Overall the respondents rated their oral health as high, and they stated that oral health was important. In our study, the taste of the toothpaste was important in the three oldest age groups, while adolescents mainly used whatever toothpaste was available at home. Saxer et al (25) noted that when people liked the taste of toothpaste they brushed their teeth longer.
Toothbrushing with fluoride toothpaste is significant for the prevention of caries, and the population in Sweden appears to have embraced this practice to a large extent. However, there are several areas where improvements can be made, such as brushing time, amount of toothpaste and post-brushing procedures. Especially the oldest age groups showed unfavourable toothbrushing habits, which is unfortunate since these are most at risk of caries in any case (33). Few respondents reported that they had been taught about toothpaste technique. Since toothbrushing with fluoride toothpaste is the most important tool for people in self-care, oral health promotion must include the transfer of knowledge of the most
13 effective toothpaste technique. These efforts must include both measures that target the entire population and individual measures taken during dental visits in conjunction with effective health education methods.
Acknowledgements
We thank Mr Tommy Johnsson for performing the statistical analysis and Linda Scheck for revising the manuscript. The study was financially supported by the Public Dental Service in
Västra Götaland Region, Sweden.
14 References
1. Marinho VC, Higgins JP, Sheiham A, Logans S. Fluoride toothpastes for preventing
dental caries in children and adolescents. Cochrane Database Syst Rev
2003:CD002278.
2. Bratthall D, Hänsel-Petersson G, Sundberg H. Reasons for the caries decline: what do
the experts believe? Eur J Oral Sci 1996;104:416-22.
3. Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoride mouthrinses for preventing
dental caries in children and adolescents. Cochrane Database Syst Rev
2003:CD002284.
4. Marinho VC, Higgins JP, Logan S, Sheiham A. Fluoride varnishes for preventing
dental caries in children and adolescents. Cochrane Database Syst Rev
2002:CD002279.
5. Marthaler TM. Changes in dental caries 1953-2003. Caries Res 2004;38:173-81.
6. Bagramian RA, Garcia-Godoy F, Volpe AR. The global increase in dental caries. A
pending public health crisis. Am J Dent 2009;22:3-8.
7. Popkin BM, Nielsen SJ. The sweetening of the world´s diet. Obes Res 2003;11:1325-
32.
15 8. Twetman S, Axelsson S, Dahlgren H, Holm AK, Källestål C, Lagerlöf F et al. Caries
preventive effect of fluoride toothpaste: a systematic review. Acta Odontol Scand
2003;61:347-55.
9. Richards A, Fejerskov O, Larsen MJ. Fluoride concentrations in dentifrices in relation
to efficacy, side-effects and salivary clearance. In: Embery G, Rölla G, editors:
Clinical and Biological Aspects of Dentifrices. Oxford: Oxford University Press,
1992; 73-90.
10. Sjögren K, Birkhed D. Effect of various post-brushing activities on salivary fluoride
concentration after toothbrushing with sodium fluoride dentifrice. Caries Res
1994;28:127-31.
11. Davies RM, Ellwood RP, Davies GM. The rational use of fluoride toothpaste. Int J
Dent Hyg 2003;1:3-8.
12. Zero DT, Creeth JE, Bosma ML, Butler A, Guibert RG, Karwal R et al. The effect of
brushing time and dentifrice quantity on fluoride delivery in vivo and enamel surface
micro hardness in situ. Caries Res 2010;44:90-100.
13. Twetman S. Caries prevention with fluoride toothpaste in children; an update. Eur
Arch Paediatr Dent 2009;10:162-67.
16 14. Klock B, Emilson CG, Lind SO, Gustavsdotter M, Olhede-Westerlund AM.
Predicition of caries activity in children with today´s low caries incidence. Community
Dent Oral Epidemiol 1989;17:285-88.
15. Koivusilta L, Honkala S, Honkala E, Rimpelä A. Toothbrushing as part of the
adolescent lifestyle predicts education level. J Dent Res 2003;82:361-66.
16. Wendt LK, Hallonsten Al, Koch G, Birkhed D. Oral hygiene in relation to caries
development and immigrant status in infants and toddlers. Scand J Dent Res
1994;102:269-73.
17. Hedman E, Ringberg C, Gabre P. Knowledge of and attitude to oral health and oral
diseases among young adolescents in Sweden. Swed Dent J 2006;30:147-154.
18. Macgregor ID, Balding J, Regis D. Toothbrushing schedule, motivation and ”lifestyle”
behaviours in 7,770 young adolescents. Community Dent Health 1996;13:232-37.
19. Poutanen R, Lahti S, Hausen H. Oral health-related knowledge, attitudes, and beliefs
among 11 to 12-year-old Finnish schoolchildren with different oral health behaviors.
Acta Odontol Scand 2005;63:10-6.
20. Kay E, Locker D. A systematic review of the effectiveness of health promotion aimed
at improving oral health. Community Dent Health 1998;15:132-44.
17 21. Hugoson A, Lundgren D, Asklöw B, Borgklint G. The effect of different health
programms on young adult individuals. A longitudinal evaluation of knowledge and
behaviour including cost aspects. Swed Dent J 2003;27:113-30.
22. Hugoson A, Koch G, Gothberg C, Lundin SA, Norderyd O, Sjodin B et al. Oral health
of individuals aged 3-80 years in Jönköping, Sweden during 30 years (1973-2003). I.
Review of findings on dental care habits and knowledge of oral health. Swed Dent J
2005;29:125-38.
23. Tseveejav B, Suominen AL, Hausen H, Vehkalahti MM. The role of sugar, xylitol,
toothbrushing frequency, and use of fluoride toothpaste in maintenance of adults`
dental health: findings from the Finnish National Health 2000 Survey. Eur J Oral Sci
2011;119:40-7.
24. Wikén Albertsson K, van Dijken J. Awareness of toothbrushing and dentifrice habits
in regularly dental care receiving adults. Swed Dent J 2010;34:71-8.
25. Saxer UP, Barbakow J, Yankell SL. New studies on estimated and actual
toothbrushing times and dentifrice use. J Clin Dent 1998;9:49-51.
26. Aitken RCB. Measurements of feelings using visual analogue scale. Proc R Soc Med
1969;62:989-93.
18 27. Östberg AL, Ericsson J, Wennström J, Abrahamsson K. Socio-economic and life-style
factors in relation to priority of dental care in a Swedish adolescent population. Swed
Dent J 2010;34:87-94.
28. Nordström A, Birkhed D. Effect of a third application of toothpastes (1,450 and 5,000
ppm F), including a “massage” method on fluoride retention and pH drop in plaque.
Acta Odontol Scand; in revision
29. Julihn A, Barr Agholme M, Grindefjord M, Modéer T. Risk factors and indicators
associated with high caries experience in Swedish 19-year-olds. Acta Odontol Scand
2006;64:267-73.
30. Ashley PF, Attrill DC, Ellwood RP, Worthington HV, Davies RM. Toothbrushing
habits and caries experience. Caries Res 1999;33:401-02.
31. Bernabé E, Watt RG, Sheiham A, Suominen-Taipale Aluutela A, Vehkalahti MM,
Knuuttila M et al. Sense of coherence and oral health in dentate adults: findings from
the Finnish Health 2000 survey. J Clin Periodontol 2010;37:981.
32. Ståhlnacke K, Unell L, Söderfeldt B, Ekbäck G, Ordell S. Self-perceived oral health
among 65 and 75 year olds in two Swedish counties. Swed Dent J 2010;34:107-19.
33. Petersson G, Fure S, Twetman S, Bratthall D. Comparing caries risk factors and risk
profiles between children and elderly. Swed Dent J 2004;28:119-28.
19 Table 1
Table 1. Distribution of responses regarding knowledge about fluoride toothpaste and toothbrushing. P-values show differences between age groups.
15-16years 31-35 years 61-65 years 76-80 years Questions Percent Percent Percent Percent P-value
What is the effect of fluoride in toothpaste? n=445 n=448 n=592 n=517 Makes teeth whiter 11 4 2 3 <0.0001 Strengthens the teeth 75 90 83 63 <0.0001 Clean teeth 20 21 12 22 <0.0001 Makes your mouth fresh 24 21 22 28 NS Do not know 17 4 6 12 <0.0001
What is most important in avoid caries? n=444 n=447 n=592 n=519 <0.0001 Toothbrushing 16 22 33 21 Fluoride in toothpaste 16 8 7 12 Toothbrushing and tooth- 68 70 60 67 paste are equally important
Have you had any toothpaste instruction? n=440 n=445 n=587 n=506 No instruction 61 72 74 78 <0.0001 From parents/family 16 2 2 1 <0.0001 From dental personnel 21 23 22 19 <0.0001 From advertisement, brochure 0 0 0 1 NS From school personnel 1 2 1 1 NS Other 1 1 1 0 NS
Table 2
20 Table 2. Distribution of responses regarding attitudes towards fluoride toothpaste and toothbrushing. P-values show differences between age groups.
15-16years 31-35 years 61-65 years 76-80 years Questions Percent Percent Percent Percent P-value
Is toothbrushing important? n=442 n=449 n=595 n=523 <0.0001 Yes, very important 59 88 89 85 Yes, quite important 40 12 11 15 Not important 1 0 0 0
Is tooth brushing with toothpaste important? n=439 n=449 n=590 n=513 <0.0001 Yes, very important 87 95 77 68 Yes, quite important 13 5 22 30 Not important 0 0 1 2
What is important when choosing toothpaste? n=443 n=445 n=569 n=502 Price 7 31 17 17 <0.0001 Taste 22 57 49 49 <0.0001 Advertisements 9 16 15 13 <0.05 Uses what’s at home 74 21 33 34 <0.0001 Do not know 7 11 6 6 <0.05
What is important to you? n=442 n=449 n=592 n=518 Healthy teeth (p<.0001) 66 84 85 75 <0.0001 White teeth (p<.0001) 35 9 5 4 <0.0001 No cavities (p<.001) 43 33 39 47 <0.001 Other (p<.05) 4 3 5 7 <0.05
Table 3
21 Table 3. Distribution of responses regarding toothbrushing behaviour and use of toothpaste. P-values show differences between age groups.
15-16years 31-35 years 61-65 years 76-80 years Questions Percent Percent Percent Percent P-value
Toothbrushing frequency n=446 n=449 n=596 n=527 <0.0001 Less than once per day 2 0 1 1 Once per day 9 6 11 15 Twice per day 87 91 77 66 Three times or more 2 3 11 18 Time for toothbrushing n=445 n=449 n=595 n=523 Before breakfast 7 18 28 23 <0.0001 After breakfast 88 83 70 69 <0.0001 Before dinner 1 1 2 1 NS After dinner 6 5 6 17 <0.0001 Before going to bed 91 94 93 89 <0.001 Toothbrushing duration n=440 n=449 n=595 n=516 <0.0001 Half a minute or less 10 7 7 15 One minute 24 23 25 31 Less than two minutes 23 26 24 20 Two minutes 30 30 31 28 More than two minutes 13 14 13 6 Amount of toothpaste on a regular brush n=419 n=405 n=487 n=467 <0.001 Size of a pea 4 5 7 5 0.5 cm 14 20 21 22 1 cm 51 55 48 50 2 cm 31 20 24 23 Times toothbrush dipped in water n=440 n=448 n=584 n=496 <0.0001 Never dip 28 45 30 24 1-2 times 57 45 43 35 3 times or more 15 10 27 41 Subsequent rinsing with water n=443 n=448 n=595 n=520 <0.0001 Never 21 22 12 10 Occasionally 21 19 11 12 Often 17 18 14 14 Always 38 40 61 62 Never considered 3 1 2 2 Amount of water when rinsing n=345 n=348 n=517 n=455 <0.0001 A handful 54 77 57 32 Two handfuls 22 14 15 17 Half a glass of water 18 7 24 43 A full glass of water 6 2 4 8 Table 4
22 Table 4. Distribution of responses regarding oral hygiene habits. P-values show differences between age groups.
15-16years 31-35 years 61-65 years 76-80 years Questions Percent Percent Percent Percent P-value
Type of toothbrush n=444 n=447 n=595 n=524 <0.0001 Regular 80 66 49 68 Electric 7 13 22 14 Both regular and electric 13 21 29 18
Perform interdental hygiene n=440 n=446 n=595 n=521 <0.0001 Yes 33 54 51 51 No 67 46 49 49
Use of mouthwash n=441 n=448 n=591 n=512 <0.0001 No use of mouthwash 66 52 64 65 Mouth rinse 0.2 % fluoride 24 36 17 21 Essential oil mouth rinse 6 9 12 8 Mouth rinse containing 1 2 5 3 chlorhexidine and zink (SB12) Other/unknown 2 1 2 3
Figure 1
23 All individuals ages 15-16, 31-35, 61-65 and 76-80 respectively in the two municipalities Enköping and Stenungsund
Individuals selected from randomly 5 individuals living in chosen birthdates - 400 individuals nursing homes were from each age group and each excluded. municipality = 3,200 participants Men: 48.4%. Women: 51.6%
29 questionnaires returned 3,200 questionnaire sent by post – with “address unknown” or 1,600 to Enköping and 1,600 to “deceased”. Stenungsund
29 additional questionnaire were sent to randomly selected 1177 individuals did not individuals respond: 15-16 y.: 354 (44%) 31-35 y.: 351 (44%) 61-65 y.: 201 (25%) Reminder was sent after 3 weeks. 76-80 y.: 271 (34%)
Men: 53.7% Women: 46.3% A total of 2,023 individuals (63 %) responded:
15-16 y. 446 (56%) 31-35 y. 449 (56%) 61-65 y. 599 (75%) 76-80 y. 529 (66%)
Men: 46.3% Women: 53.7%
Figure 2
24 60
50 ) % ( s l a 40 u d i v i d n i
30 f o n o i t r 20 o p o r P 10
0 15-16y 31-35y 61-65y 76-80y
Figure 3
25 A. Men 15 E. Poorer oral health A. Women
10 E. Good oral health B. 15-16y.
5
D. Not important 0 B. 31-35y.
D. Important B. 61-65y.
C. Lack of knowledge B. 76-80y.
C. Knowledge
.
Legends
26 Figure 1. Flow chart showing the study design, number of respondents/non-respondents and some characteristics of the respondents/non-respondents in the study.
Figure 2. The respondents descriptions of how they experience their oral health. Good Rather good Neither good or bad Rather bad Bad
Figure 3. Factors significantly related to “Good toothpaste behaviour” (percent of individuals) A. Sex: Significant differences P <0.01 (Chi2-test) B. Age: Significant differences P <0.0001 (Chi2-test) C. Knowledge, agree that fluoride strengthens the teeth: Significant differences P <0.01 (Chi2- test) D. Important, believe that brushing with fluoride toothpaste is important: Significant differences P <0.0001 (Chi2-test) E. Good oral health, rate their own oral health as good: Significant differences P <0.05 (Chi2- test)
27