Review of Nepal Health Sector Programme: A Background Document For The Mid-Term Review Mick Foster, John Quinley, Raghav Regmi and Binjwala Shrestha Final Report November 2007
Mick Foster Economics Ltd Development Consultancy Center (DECC) 9 Admirals Walk GPO Box # 5082 Chelmsford Nayamarga, Newplaza, Putalisadak, Essex Kathmandu, Nepal CM1 2XS Tel/Fax +977-1-4417361 England Email: [email protected] www.mickfoster.com Website: www.deccnepal.org +44 1245 355031
Review Of Progress Nepal Health Sector Programme
CONTENTS
ACKNOWLEDGEMENTS...... 4 ABBREVIATIONS AND ACRONYMS...... 5
1 1. EXECUTIVE SUMMARY...... 7 2. BACKGROUND...... 15 3, HEALTH OUTCOME TARGETS AND PERFORMANCE...... 16 4. PROGRESS AGAINST NHSP OUTPUTS...... 19
OUTPUT 1 ESSENTIAL HEALTH CARE SERVICES...... 20 Public Health Programmes...... 20 Curative Services...... 21 OUTPUT 2 DECENTRALISATION...... 21 OUTPUT 3 PRIVATE AND NGO SECTORS...... 23 OUTPUT 4 SECTOR MANAGEMENT...... 26 OUTPUT 5 HEALTH SECTOR FINANCING...... 27 Health Sector Budget...... 27 Aid Coordination and Harmonisation...... 30 Transparency of the Budget...... 31 OUTPUT 6 LOGISTICS MANAGEMENT...... 31 Physical Facilities...... 33 OUTPUT 7 HUMAN RESOURCE DEVELOPMENT...... 34 OUTPUT 8 HEALTH MANAGEMENT INFORMATION SYSTEM...... 35 OVERALL JUDGEMENT ON NHSP PROGRESS AT MID-TERM...... 36 5. PRIORITIES FOR THE FUTURE...... 37
5.1 OPPORTUNITIES FOR FURTHER PROGRESS IN REDUCING MORTALITY...... 37 Maintaining, Refining, Expanding Successful Programs...... 37 Maternal and newborn care...... 37 Malnutrition...... 38 Beyond EHCS...... 39 5.2 IMPROVING ACCESS BY THE POOR AND SOCIALLY EXCLUDED...... 40 Evidence on Inequality in Health Outcomes...... 40 Inequality In Access To Health Services...... 41 Existing MOHP Strategies To Tackle Inequality...... 44 Recommendations on Reducing Inequality...... 47 5.3 HEALTH SECTOR FINANCING AND FINANCIAL MANAGEMENT...... 48 The Role of User Charges...... 48 Community Drug Programme...... 49 Community Health Insurance...... 50 Budget Management...... 50 5.4 MANAGEMENT REFORM TO SUPPORT BETTER HEALTH OUTCOMES...... 51 Performance Management...... 51 Management Reform and the NHSP Log-Frame...... 52 5.5 HUMAN RESOURCES MANAGEMENT...... 52 5.6 MANAGING THE SWAP...... 53 Integrating the JAR within the MOHP Review...... 53 Longer Term, Predictable Finance...... 54 Reforming Pool Funding (and attracting more donors)...... 55 6. RECOMMENDATIONS...... 56
6.1 CHANGES TO THE NHSP LOG FRAME...... 56 6.2 FUTURE PRIORITIES FOR EHCS...... 56 6.3 INEQUALITY OF ACCESS...... 56 6. 4 MANAGEMENT AND RELATED REFORMS...... 57 6. 5 MANAGING THE SECTOR WIDE APPROACH...... 58 ANNEX 1 TERMS OF REFERENCE...... 59 ANNEX 2 LIST OF CONTACTS...... 62 ANNEX 3 SUGGESTED REVISIONS TO EHCS TARGETS AND INDICATORS...... 65 ANNEX 4 STATUS OF NHSP LOG-FRAME TARGETS...... 71
2 ANNEX 5 THE IMPACT OF FREE BASIC SERVICES...... 79
CURRENT POLICY ON CHARGES...... 79 COST OF FREE BASIC SERVICES...... 80 AFFORDABILITY OF FREE BASIC SERVICES...... 84 ANNEX 6 LIST OF REFERENCES...... 85
List of Tables Table 3.1 Reductions in Mortality Rates 1996-2006...... 16 Table 3.2 Explaining The Reduction In Under 5 Mortality...... 18 Table 3.3 Maternal mortality reduced...... 19 Table 4.2 Analysis of MOHP Budget and Spending 2003/4-2007/08 (NR m)...... 28 Table 5.1 Inequality in Under 5 Mortality...... 40 Table 5.2 Moderate to Severe malnutrition: % of Children More than 2 Standard Deviations Below Average...... 41 Table 5.3 Ethnic and religious Differences in Safe Motherhood Care...... 43 Table 5.4 Unequal Distribution of Health Personnel...... 45 Table 5.6 Estimated Cost of Free or Subsidised Services...... 81
3 Acknowledgements
We are grateful to the many staff in MOHP, MOF, NPC and external development partners who made time to meet us and who provided information. Particular thanks are due to Dr B.R. Marasini and to Susan Clapham of DFID. The study was financed by DFID, the World Bank, and SDC.
4 Abbreviations and Acronyms ADB Asian Development Bank AHW Auxiliary Health Worker AIDS Acquired Immune Deficiency Syndrome ANC Antenatal Care ANM Auxiliary Nurse Midwife AWPB Annual Work-Plan and Budget BCC Behavioural Change Communication BEOC Basic Emergency Obstetric Care BP Business Plan BPP Birth Preparedness Package CB-IMCI Community Based Integrated Management of Childhood Illness CB-MNC Community Based Maternal Neonatal Care CBO Community Based Organisation CDP Community Drug Programme CEOC – Comprehensive Emergency Obstetric Care CFAA Country Financial Accountability Assessment CHI Community health Insurance DDA Department of Drug Administration DDC District Development Committee DFID Department for International Development (UK) DoHS Department of Health Services DPHO District Public Health Office/Officer EDP External Development Partners EHCS Essential health Care Services EOC Emergency Obstetric Care EPI Expanded Program for Immunization FCGO Financial Comptroller General’s Office FCHV Female Community Health Volunteer FGD Focus Group Discussions FHD Family Health Division GO Governmental Organisation GoN Government of Nepal HA Health Assistant HDI Human Development Index HF Health Facility HFMC Health Facility Management Committee HIV Human Immunodeficiency Virus HMIS Health Management Information System HP Health Post HR Human Resource HRD Human Resources Development HRM Human Resource Management
5 HSRU Health Sector Reform Unit HuRDIS Human Development Information System IFMS Integrated Financial management System IMCI Integrated Management of Childhood Illness INGO International Non-Governmental Organisation JAR Joint Annual Review LMIS Logistic Management Information System MCHW Maternal & Child Health Worker MDG Millennium Development Goal MMR Maternal Mortality Ratio MOF Ministry of Finance MOHP Ministry of health and Population MTEF Medium Term Expenditure framework NDHS Nepal Demography Health Survey NGO Non Governmental Organization NHSP-IP Nepal Health Sector Programme- Implementation Plan NLSS Nepal Living Standard Survey NPC National Planning Commission OPD Patient Department PHCC Primary Health Care Centre SBA Skilled Birth Attendant SDC Swiss Agency for Development and Cooperation SHP Sub Health Post SSMP Support to Safer Motherhood Programme SWAP Sector Wide Approach TA. Technical Assistant TBA Traditional Birth Assistant TORs Terms of Reference VDC Village Development Committee VHW Village Health Worker WHO World Health Organization
6 1. Executive Summary Good Progress In Reducing Mortality Is Due To Effective Public Health Interventions The 2006 DHS survey1 shows that Nepal has achieved excellent progress in reducing mortality, nearly halving under five and maternal mortality, and reducing adult mortality by nearly one third. Nepal has overtaken India, achieving lower under five and infant mortality despite less favourable economic conditions and social indicators such as women’s education.
Analysis by the team shows that the majority of the mortality reduction can be explained by a small number of public health interventions. About three quarters of the reduction in under five mortality can be explained by the expansion of immunisation; Vitamin A capsules, community-based management of childhood illness, neonatal tetanus control, and improved home care for newborns. Although the private sector has made some contribution, the bulk of the credit goes to the public sector. The public sector has been entirely responsible for immunisation, Vitamin A distribution, de-worming; has led campaigns to change the care of newborns; and is responsible for about half of child visits to health service providers, including about half of treatment for pneumonia.
It is probable that the actual reduction in maternal mortality may be less than the central estimates in the survey suggest: maternal mortality is a low frequency event that is hard to measure precisely with sample surveys. A significant share of the reduction in maternal mortality can be explained by an increased share of deliveries taking place with skilled birth attendants, including an increased share delivered within health facilities (including more C-sections). About 25% of facility based deliveries are within the private sector. Adult mortality reduction is likely to have been mainly due to better TB control, lower fertility, and lower maternal deaths. Reduced maternal deaths reflect lower total fertility due to the success of family planning as well as a reduced maternal mortality rate.
The public health programmes were successful because:- i. They are delivered by locally resident volunteers and staff who are more accountable to the communities they live in (FCHV, VHW, MCHW). ii. They can be scheduled in advance, and do not require staff to be available at other times, as is the case with, for example, delivery care. iii. They are cheap and are offered free to the user, enabling them to be scaled up towards universal coverage. iv. They are delivered by Government, but have had long-term external support that has built sustainable capacity. Although technical assistance has been heavy, and remains so in some cases, the informed view of those consulted is that programmes might be weakened but would not be wrecked by the withdrawal of external TA.
1Department of Health Services, Ministry of Health and Population , New Era, USAID, Nepal Demographic Health Survey, 2006
7 Less Success In Curative Services Reflects Institutional Problems Curative services have been less successful. Outpatient contacts are low and stagnating at 0.38 per person per annum2. Maternal care has made some progress, but over 80% of deliveries still take place without the presence of a skilled birth attendant. On the demand side, low utilisation is caused by high out of pocket costs for perceived low quality services that are not available where and when needed. On the supply side, the quality and availability of services is compromised by:- i. Critical staff shortages (roughly half of Doctor posts are unfilled3, there is a shortage of skilled birth attendants), combined with frequent staff absence. ii. Lack of sufficient drugs and consumables iii. Location and standard of physical facilities in some areas
Budgets Have Been Increased And Reflect NHSP Targets The MOHP share of the national budget has increased steadily since the start of NHSP, reaching 7.2% in 2007/8, on track to reach the targeted 7.7% in 2009, though we would caution that it may be irresponsible to insist on a budget share target in the absence of any overall analysis of expenditure priorities across sectors. The structure of the budget reflects NHSP output targets, with the agreed share of 70% to EHCS, while 63% of the budget goes to preventive services4. About half (51%) of the budget is aid funded.
Actual health spending improved from 76% of 2005/6 budget to over 90% in 2006/7 (exact figures await reconciliation), but the finalisation of AWPB and issuing of expenditure authorisations was delayed in 2007/8, and the improved performance may not be sustained. Progress has been made in recording a larger share of aid in the budget. All of the aid identified in the MOF Sourcebook (the ‘White Book’) is included in the budget in 2007/85, including non-traditional donors such as India, and the AWPB6 contains a useful matrix relating EDP commitments to the expenditure programmes they are helping to finance.
Progress on Some Other NHSP Outputs NHSP is contributing to better sustainability of health programmes. A larger share of the cost of key programmes is being funded from regular budget resources, for example the scale-up of the IMCI programme to additional districts did not depend on project commitments but drew on GON and pooled fund resources, which now account for 60% of the costs of the programme.
2 DOHS Annual Report, new outpatient contacts. It is an under-estimate because only 62% of identified private sector providers reported in 2005/6, and the figure does not include informal consultations by pharmacies. 3 DOHS Annual Report 2005-6 4Ministry of Health and Population, Health Sector Reform Unit Government of Nepal, August, Budget Analysis 2007-08, Ministry of Health and Population, 2007 5 Government of Nepal, Ministry of Finance, Source Book of projects Financed with Foreeign Assistance, FY 2007-08
6 GoN, Ministry of Health & Population, Department of Health Service Annual Work Plan & Budget 2064/65(2007-2008)
8 Procurement and logistics generally have been long-standing problems, and 2006 witnessed some regrettable problems in relation to routine procurement of drugs and commodities. This happened despite sustained attention to building logistics capacity. Informed opinion is that it reflected nervousness related to a combination of the introduction of new procurement procedures, and some high-profile cases in which those not following procurement rules had been harshly dealt with by the then Government. The problems seem to have been overcome; there are no current problems in the pipeline of future procurement, though close monitoring is needed to avoid future supply interruptions.
The HMIS is a major achievement, generating a range of detailed operational information that few low income countries could match. Comparison with the NDHS suggests that the data is broadly accurate. The data that is collected is the major focus of the regional and national reviews that MOHP/DOHS conduct, encouraging the reviews to focus on performance, as we were able to observe through attendance at part of the Western Regional review. The data is published in the departmental report, which is a valuable source of detailed information on operational performance7. The main gaps in the available information are the lack of data on human resources, the difficulty of relating budget and expenditure data to the specific health programmes it is intended to finance, and the lack of data disaggregated by gender, ethnicity, caste, and religion. A pilot in three districts is collecting more disaggregated data including on staffing.
Human Resources The 2005/6 Annual Report showed 300 vacant posts for Doctors, about half of the total, and shortages for nurses and some other mainly hospital-based specialists, though 90% or more of positions for other types of health workers were filled. The Government has taken measures to reduce the shortfall, appointing 100 new doctors as permanent staff and recruiting more than 100 on contract. MOHP is also enforcing the requirement that medical students who receive public support must work for two years in Government before they can be registered to practice. Similar measures are being taken for other categories of medical staff in short supply, and the regional Directorates are being authorised to use their personnel budgets to recruit contract staff to fill vacant positions. Filling vacancies will help, but may not mean that staff are physically present and working at the times when facilities are supposed to be open. More effective performance management is limited by low per diems and late budget authorisation, making supervisors reluctant to make field visits.
The exercise of personal patronage in job allocations continues to cause high rates of transfers, causing significant disruption to the work of the department. Greater transparency, monitoring of numbers, and a greater willingness to draw public attention to cases, might have some impact on discouraging frivolous moves.
7 Department of Health Services, Ministry of Health and Population,, Annual Report 2005-2006
9 It is Government policy to phase out the VHW and MCHW cadres in favour of AHW and ANM staff as the lowest level permanent employees. Many of the existing staff lack the educational qualifications for upgrading, and will be phased out as they reach retirement age. The main concern with this approach is that the two cadres that are being phased out are the locally resident and therefore accountable staff that have, together with the unpaid FCHVs, been mostly responsible for successful implementation of public health programmes. The better qualified replacements are less likely to live locally and may be less willing to do the routine work such as mass immunisation. The impact on coverage of public health programmes needs to be monitored as the upgrading progresses, and the policy re-considered if there is evidence of a weakening of the public health interventions.
Some HMIS Outputs need Re-consideration Annex 3 and Annex 4 propose some revisions to the NHSP logframes and indicators.
Progress on the handing over of health facilities to management committees has made little difference in the absence of elected local bodies. The committees have been given no power over the staff and almost all financial resources still come from the centre and are earmarked for specific uses. The target should be dropped. Meaningful decentralisation to locally accountable elected bodies will need to await decisions on the future federal structure of the state. Delegation of more authority within the DOHS structure, however, can and should be taken further.
The log frame targets on mobilising local revenues and extending community health insurance are inconsistent with the new Government policy of extending free basic services to all, and should be dropped.
The NHSP correctly identifies the important role of the private and NGO sector, and rightly calls for cooperation and coordination. However, contracting out the management of hospitals and the responsibility for delivering specific health services to private or NGO service providers is a complex undertaking and may not be the best model for Nepal. The most appropriate institutional arrangements should be determined by the service delivery targets that NHSP wishes to reach, and outputs targeting specific institutional forms such as handing over a specified number of hospitals should be dropped.
Future Priorities for EHCS The first priority remains to maintain and scale up where necessary the public health interventions that generated the good DHS results.
In looking towards priorities for the next phase of NHSP, newborn mortality accounts for over half of under five deaths and should receive high priority. Achieving the major reductions in maternal and newborn mortality required to reach the MDGs will require coordinated improvements in access to skilled birth attendants, facilities for basic and comprehensive emergency obstetric care when needed, and improved incentives for mothers and staff. Initiatives to introduce most of these measures are in place, but there
10 are a number of challenges to coordinate facilities, staff, and incentives, while overcoming the teething problems that have accompanied the introduction of the MIS. Differences of terrain and population density mean that what is practical and affordable will differ between different parts of Nepal, and further refinement of the strategy is needed to get the mix of inputs right.
Although not an alternative to facility-based maternity care, low-cost pilot programmes of community based maternal and newborn care have achieved some promising reductions in maternal and newborn mortality. DOHS is developing a standard model that will be scaled up to 10 districts in the next year. If successful, this could be taken to national scale as a key programme for the next NHSP.
Reducing general malnutrition in children could have a large mortality impact. The problem is not mainly related to lack of food but to feeding practices. There are no good large scale models of how a programme to tackle malnutrition through the health services could work in Nepal, although UNICEF are about to start work with the MOHP on a pilot project in the terai8, drawing lessons from a number of African experiences of treating severe and acute malnutrition. The aim is to develop a cost-effective approach for subsequent scaling up.
Tackling Inequality Gender differences in health outcomes have been closed. There is no gender gap in under 5 mortality, while death rates for women aged 15-49 are now 16% lower than for men as a result of a 43% reduction in women’s death rates due to lower fertility and reduced maternal mortality.
The poor have the largest unmet demand for family planning, make the lowest use of maternal care, have the lowest vaccination coverage, and are least likely to seek care when ill. In geographical terms, the mid and far west regions have the deepest poverty and also the worst access to health services. Earlier surveys have shown that Dalits and ethnic and religious minorities have lower utilization of health services. The data that was collected on minority groups during the NDHS was still being analyzed at the time of writing, but could provide useful additional understanding of which groups are not benefiting from health care. It should be reported to the mid-term review meeting.
MOHP has taken practical steps to tackle inequality. Universal free coverage of public health measures such as Vitamin A ensures everyone benefits. Specific targeting for groups who tend to be low users of health services will become increasingly important as public health interventions approach universality and remaining pockets without access need to be reached. Micro planning, mapping pockets of non-coverage and planning how best to reach them, has been used with success to raise coverage in low-performing EPI districts, and is also being applied in family planning.. It may need to be supported by specific action to mobilize neglected communities to exercise their rights to basic health services, while raising the awareness of health workers with respect to particular causes
8 Community Based Therapeutic Care.
11 of non-coverage. Further progress on issues such as geographical resource allocation needs to be advanced as and when the political process permits.
The 2006 NDHS found that cost was an important reason for people not seeking care, but factors related to the quality of the service (absent staff and drugs) and to access (need for transport) were mentioned more frequently. User charges are not the only out of pocket cost, a factor recognised by the maternity incentive scheme, which also aims to help with transport costs.
The Government decision to make outpatient services free at sub-health post and health post level should reduce inequality, because the poor are the most intensive users of facilities at this level9, and are most likely to respond to reductions in cost10. The alternative policy of targeting the poor to receive free services while charging others has rarely been successful, and the cost savings are modest once the administration costs are included11. Available cost estimates12 suggest that the additional cost of extending free services to all up to district hospital level, including outpatient, emergency and in patient services, should be less than $1 per head. This should be affordable if phased in over two to three years, by adding PHCs and district hospitals, perhaps starting with the low human development index districts. However, a more detailed cost estimate should be prepared, as there are considerable uncertainties.
Disaggregated data is needed to monitor issues of inequality of access. The results of the pilot of a more disaggregated HMIS need to be reviewed quickly, necessary modifications agreed, and training and support provided to enable all districts to begin collecting disaggregated data.
If, as expected, the NDHS reveals that significant differences in health outcomes and health service access persist and can not be entirely explained by poverty, it is suggested that the Secretary consider issuing guidance that inclusion issues should be addressed in the 2008/9 AWPB and at the 2007/8 Annual Review, and should convene an AWPB working group to review drafts and ensure that the issue has been adequately addressed.
It is recommended that the next NHSP should make explicit reference to the objective of achieving more equal access to health services by all caste, ethnic, religious and other groupings in Nepali society. The NHSP2 design process should give explicit attention to how best to mainstream inclusion issues, including the implications for institutional arrangements.
Community Drug Programmes and CHI The CDPs will lose most of their revenue once all essential health services up to district hospital level are made free. They might have a residual role in the short-medium term
9 Nepal Living Standards Survey, 2004 10 Rob Yates, presentation to MOHP, September 2007 11 Yates, op cit 12 Devi Parasai, RTI International, Health Economics and Financing Unit, 2007
12 until MOHP demonstrates capacity to meet demand for consumables. They could also continue to procure drugs not included on the essential drugs list.
There is no role for community health insurance once the health costs it is intended to insure against become free.
Beyond EHCS The Government role in financing secondary and tertiary care is necessarily limited by a budget per head that is barely sufficient to finance public health interventions and basic curative care. The task for Government is to decide what limited services it needs and can afford to finance, and how best to procure them, which is likely to imply some partnership with the private sector institutions that are providing a large share of specialist care and are training the majority of doctors. One possibility as funds permit would be to meet the cost of referrals from district hospitals at agreed rates, allowing referrals to private sector hospitals when appropriate. This benefit should be means tested.
Doctors and nurses in district hospitals and PHCs need improved professional supervision. This could be supported by developing relationships with regional and zonal hospitals, or even with private hospitals, as the private hospitals association has suggested. There could be mutual advantage to short-term secondments of staff and development of telemedicine and other techniques to support isolated junior doctors.
Nepal has so far resisted pressures for higher spending on secondary and tertiary care. Moving national hospitals to fixed block grant funding while requiring them to raise other revenues themselves would limit future budgetary risks while providing incentives to make efficiency savings and find innovative ways to finance their own development.
Increasing middle class demand for Government spending on tertiary care can also be controlled by developing health insurance within the formal sector of the economy, possibly including the civil service. If the middle classes have a mechanism for spreading the financial risk of a catastrophic illness requiring expensive treatment, it should diminish the risk of political lobbying for increased spending on subsidised tertiary care.
Management Reform To Support Health Outcomes The management reform outputs envisaged in the NHSP are mostly unachieved. This partly reflects the effects of political turmoil, but there has also been a problem of lack of capacity. Recent changes should improve matters, with the appointment of a new head of the HSRU at Joint Secretary level, an additional staff member added, and the technical assistance from RTI now underway and co-located in the MOHP building. Though increased capacity will help, developing and implementing a coherent action plan for organisational change will require strong and determined leadership from the top of the Ministry.
Avoiding a negative impact on the quality of care following the abolition of charges for basic care will require MOHP to make available sufficient and timely extra resources to
13 compensate facilities for increased demand and lost revenue. The existing geographical allocation of staff and resources is already poorly matched to demand, and is likely to become moreso if free services result in a significant, but uneven, increase in demand. Increased resources will need to follow the demand, which will require unprecedented flexibility in the allocation of the budget.
The extra demand will only be sustained if staff behaviour changes in order to ensure that facilities are open, staffed, and stocked with drugs at the times and in the locations where people need them. Staff will have to work longer while increased MOHP provision of free medicines will reduce their private pharmacy income. It is proposed that the success of free services in galvanising higher output from the health system would be more assured if accompanied by the development, piloting, and phased introduction of performance based incentives, for facilities and staff. A 3-district pilot scheme was interrupted, but a detailed model has been developed and could be adapted13. There may also be lessons to be learned from other sectors and from the design of incentives under the local government development programme.
For equity, increased resources to help better performing districts meet growing demand will need to be complemented by monitoring the causes of lower utilisation elsewhere, and the implementation of interventions as necessary to remove the critical constraints.
Budget Management The importance of leadership can be illustrated by the long standing and Nepal wide problem of low utilisation of the approved budget. Delays occur at numerous levels, and partly reflect problems caused by an overly bureaucratic Government system of budget management, together with the reluctance of cautious civil servants to utilise the flexibility that exists. For example, up to one third of the previous year’s budget can be spent on P1 activities in advance of formal authorisation. Civil servants at all levels nevertheless tend to wait for the approval letter before starting activities. External development partners share significantly in the responsibility, as EDP funds consistently show the lowest percentage disbursement, partly reflecting late or incomplete approval of funds, and partly reflecting problems in complying with donor procedures, including submission of financial monitoring reports and obtaining timely ‘no objections’ to procurement proposals. Nevertheless, in 2006/7, the final figures are likely to confirm a significant improvement in the rate of disbursement of the budget, mainly due to regular meetings held by the Minister and Secretary in order to check progress and ensure that necessary steps were not being delayed. Unfortunately, the knock-on effects of late finalisation of the 2007/8 budget ceilings are likely to mean that the good 2006/7 performance will not be sustained. High level attention to budget monitoring needs to be continued, and might usefully be accompanied by a stronger role for the regional directorates in encouraging more pro-active management by the districts. The recently completed RTI study of bottlenecks will also be helpful14.
13MOHP, Piloting of Performance-based Management System in Ministry of Health and Population, Highlights of Activities and Draft performance Improvement Plan for Sub-Health Posts, February 2006 14 RTI International, Supplemental Work plan, 17 September 2007- 30 June 2010
14 Managing the SWAP The SWAP is supposed to be a mechanism for supporting the Government health sector strategy, while moving towards increased harmonisation and alignment with Government systems. The November-December JAR should be combined with the MOHP Annual Review. It should continue to focus on performance in the previous year, but that review of performance should trigger EDP decisions on their future level of support.
The EDPs finance more than half of the health budget. External commitments often come too late in budget preparation, are too short term for planning purposes, and too unreliable in converting promises to actual disbursements. This has serious consequences for the ability of MOHP to sustain and develop the critical public health programmes that have saved so many lives. Wherever possible, EDP commitments or at least indications should be multi-year. Alterations to announced figures should be minimised. If EDPs have to adjust their spending, or feel compelled to do so because of concerns about performance, the sanctions should apply only from the next budget year, not the current one, and MOHP should be given clear guidance on whether previously announced figures can be restored, and what actions are needed to secure this. All formalities should whenever possible be completed before July, to ensure that late approval by EDPs does not become a cause of disruption in the NHSP programmes. These changes will be easier for some donors than for others, but it is important that all go as far as their procedures will permit. They are co-responsible for what happens in the sector, and need to behave predictably, taking account of the consequences for health service delivery.
In an effort to increase budget certainty, there is a strong case for moving the pooled fund towards a fixed cash commitment rather than a percentage of the actual spending. This will help budget planning by MOF and by DFID, possibly encouraging MOF to increase the budget by factoring in the full value of the pool fund. The change should not damage the incentive for MOHP to disburse, since actual donor disbursement benefits MOF but makes no difference to the budget that MOHP receives.
The AWPB process needs to start earlier in the year, and involve both the districts and the EDPs, who finance half of the budget. The aim should be to jointly prioritise resources from all sources to ensure that the most important programmes are fully funded. If there is greater involvement and transparency between partners during the planning and budgeting process, then the June/July JAR can become an opportunity to confirm and adjust resource assumptions and priorities that have already been extensively discussed. Ideally, greater involvement in the process will build mutual trust in an AWPB that all partners understand and own, even if differences of detail remain. 2. Background The NHSP 2004-2009 started in 2004 with the intention of developing a sector wide approach, with Government and external development partners working in partnership to implement the national health sector strategy. The mid-term review of the programme is scheduled for December 3-10th 2007, and is an opportunity to take stock of what has been achieved, consider adjustments and course corrections for the remaining two years, and
15 begin the process of preparing for what will come after NHSP. This independent assessment has been commissioned as a contribution to the mid-term review. Our terms of reference are reproduced at Annex 1.
The study was undertaken over a three week period in September-October 2007. It was preceded by a literature review. The main methodology was review of documents and interviewing of key informants in Government, development partners, and the private sector (list of contacts is at Annex 2). The team also undertook some analysis to estimate the probable impact of health interventions supported by the MOHP, in order to assess the extent to which health sector programmes can account for the improved health outcomes reported in successive demographic and health surveys. In addition to interviews in Kathmandu, team members visited the Western region where we observed some of the regional review and briefly met with district staff from the region. The team also visited the districts of Kaski and Syangja, and held discussions with staff from the district office, the district hospital, female community health volunteers, and a mothers group. 3, Health Outcome Targets And Performance The DHS surveys over the past 10 years have shown that Nepal has reduced under five and maternal mortality rates by about half between the early 1990s and the 2000-2006 period. Adult mortality has also declined substantially (Table 3.1). Our analysis suggests that the expansion of a small number of Essential Health Care Services over the past 10 to 15 years is sufficient to account for most of the observed decline in mortality.
Table 3.1 Reductions in Mortality Rates 1996-2006 Year of survey 1996 2001 2006 Under five mortality rate (per 1000 births) 118 91 61 Under five mortality net of neonatal mortality (per 1000 68 52 28 births) Maternal mortality rate (per 100,000 births) 539 - 281 Adult mortality 11.5 - 7.9 (% who die from age 15-49) Source: Demographic Health Surveys
The programs and activities that have shown the clearest improvements and have had the largest impacts are:- • Under five mortality – Immunizations, vitamin A, community-based management of childhood illness, neonatal tetanus control, improved home care for newborns • Maternal mortality – Emergency obstetric care, skilled birth attendants, antenatal care • Adult mortality – Tuberculosis control, maternal mortality control • Enabling programs – Family planning All of these are part of the EHCS package within the NHSP.
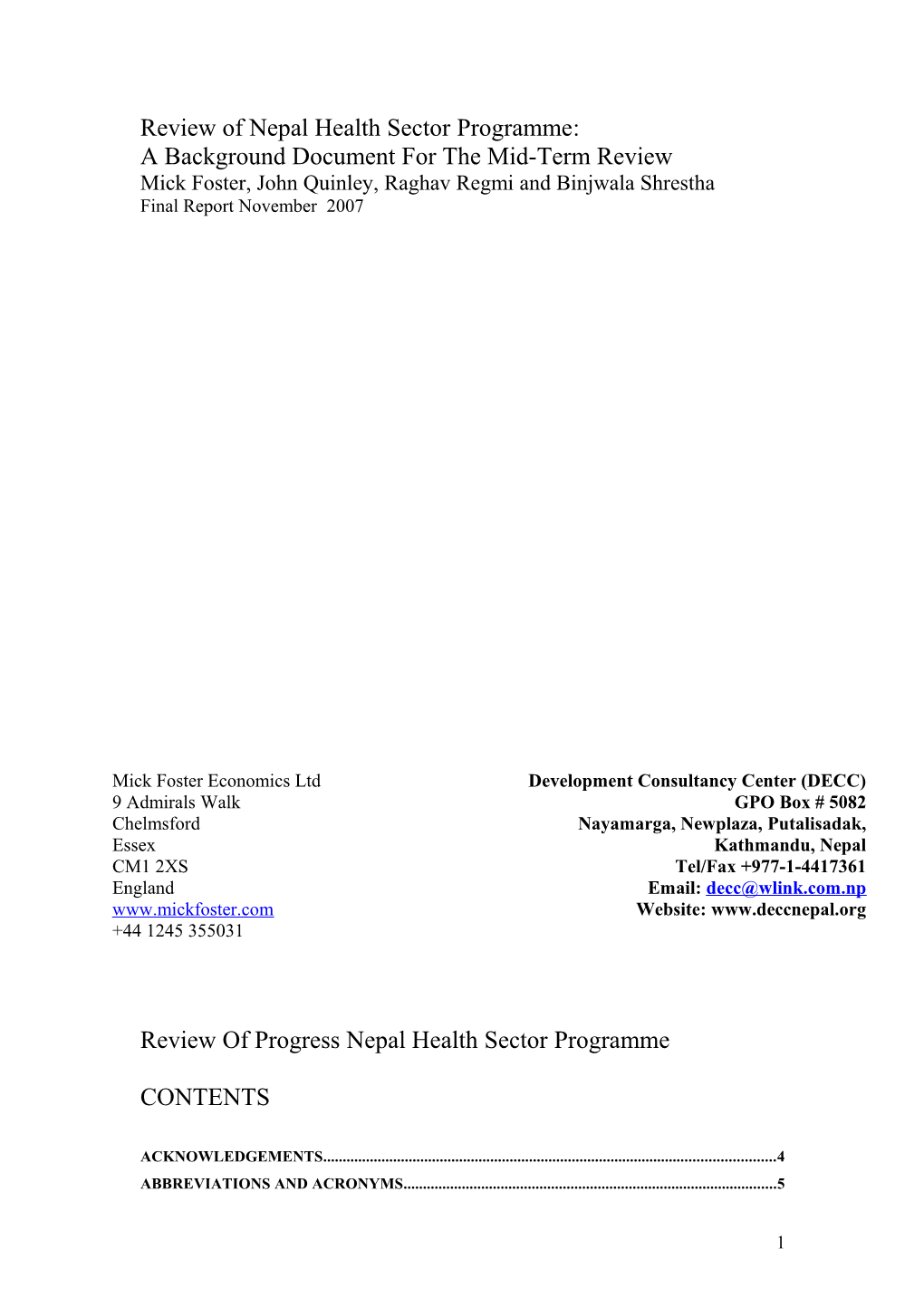
16 Another way of looking at the impact of key programs is to compare the experience of India with that of Nepal. India has the advantage of a stronger economy, better female education, and lower fertility than Nepal, all of which should keep mortality down. However, over the past 15 years Nepal has reduced under five mortality to a level lower than India (Figure 3.1).
The difference appears to be in key public health programs. Two of these that are easy to measure are vitamin A distribution and childhood immunisation. In 2006 Nepal reached over 90% of children with Vitamin A vs. only 21% for India and had 83% complete immunization compared to 44% for India. The rapid improvement of essential health care services is what has allowed Nepal to pull ahead. (Figure 3.1).
Figure 3.1 Under Five Mortality in India and Nepal 1991-2006
Nepal vs. India - Under Five Mortality Rate Deaths per 1000 live births
158 160
140
118 120 109
Nepal 100 91 India 95 74 80
60 61
40 91 92 93 94 95 96 97 98 99 01 02 03 04 05 06 Year (of survey)
For under five mortality after the newborn period, the reduction in mortality since 1996 has been about 40 per 1000 children (Table 3.1). If we look at three programs we can see that the improvement in these programs over the same time period accounts for most of this reduction (Table 3.2). Immunization coverage went from 43% in 1996 to 83% in 2006. Measles coverage, because of the second dose campaign, effectively went to near 100%. Together, the predicted mortality impact is 12 deaths per 1000 children. The vitamin A program started in 1993, reached 32% by 1996, but has been reaching 90% or more over the past five years. Its total impact is estimated at 13 per 1000 children. Finally, the increased rate of pneumonia treatment associated with the CB-IMCI program
17 has an estimated impact of 8 per 1000 children. In all three cases we are using the estimated mortality impact as calculated in the international literature (part of which comes from Nepal)15. Together, these three programs would predict 33 of the 40 observed reduced deaths. This may slightly over-estimate the combined impact, because a child saved from dying of one cause may yet die of something else before reaching the age of five. Nevertheless, the point remains that the majority of the very significant reduction in infant mortality since 1996 can be attributed to the impact of public health interventions managed by the MOHP.
Although the private sector has made some contribution, the bulk of the credit goes to the public sector. The public sector has been entirely responsible for success in immunisation, Vitamin A distribution, de-worming; it has led campaigns to change the care of newborns. The most significant private sector contribution has been curative, accounting for about half of child visits to health service providers, and a similar proportion of pneumonia treatment.
The remainder of the mortality reduction may be attributable to lower rates of childhood illness as a consequence of factors such as improved water/sanitation, slightly improved nutrition, better living standards, and the impact of improved education, especially of women.
Table 3.2 Explaining The Reduction In Under 5 Mortality 1996 2006 Estimated impact Immunizations (EPI & measles campaign) 43% 83%+ 12/1000 Vitamin A 32% 90% 13/1000 (coverage) CB-IMCI 0% 66% 8/1000 (% of Nepal covered) TOTAL 33/1000
Source: Mission estimates
For newborns the decline in mortality has been 16 per 1000 births. The biggest single factor may have been the neonatal tetanus elimination campaign, which provided most adult women in Nepal with three doses of vaccine. This appears to have reduced neonatal tetanus deaths to less than 1/1000. The rate in the early 1990s is not known but it could easily have been 5 to 10 per 1000. Additional factors are gradually improved home care for newborns. The example we have data for is the rate of breastfeeding on the first day, which has increased from 60% in the mid 1990s to 85% in 2006. A limited percentage of newborns have also benefited from increased health worker assisted deliveries, in which asphyxia can be better managed than with other attendants. These have increased from 10% in 1996 to about 23% in 2006.
Maternal mortality is a comparatively rare event, resulting in relatively small sample sizes when attempting to estimate it from surveys such as the DHS. In statistical jargon,
15 Working papers with a fuller description of the methodology are available on request from the authors.
18 the estimated rates of maternal mortality in each survey have large ‘confidence intervals’, which means that the true level of maternal mortality in each survey could be higher or lower by as much as 150 per hundred thousand births. We can be confident that maternal mortality has been reduced, but the extent of that reduction could be significantly lower than the central estimates quoted in table 3.1. For maternal mortality there have been improvements in both the rate of emergency obstetric care (measured as C-sections) and in skilled birth attendance, although both gains are limited compared to total need. Improved antenatal care coverage shows rapid gains in terms of access to at least some care, but probably has little mortality impact in itself. The relatively small improvements in maternal care observed would be expected to produce a small, but significant improvement in maternal mortality. The survey estimates of maternal mortality are compatible with this more limited gain.
Family planning is mentioned because it indirectly improves both maternal and child health. In terms of maternal health the total chance of maternal death is the maternal mortality rate multiplied by the average number of births per woman. The reduction in total fertility means that a woman’s lifetime risk of maternal death has declined even more than the MMR.
Table 3.3 Maternal mortality reduced 1996 2001 2006 Emergency obstetric 1.0% 0.8% 2.7% care (% C-sections) Skilled birth 9% 11% 19% attendance Antenatal care 42% 50% 72% coverage Family planning 4.6 4.1 3.1 (total fertility rate)
Source: NDHS
The largest factor in explaining the 3.6 percent absolute reduction in the proportion of adults who die between their 15th and 49th year may be the national tuberculosis program, which is estimated to save thousands of lives each year compared to the poor quality care available in the early 1990s. The reduction in maternal deaths also makes a significant contribution to reduced adult mortality.
4. Progress Against NHSP Outputs Annex 4 summarises progress against the 8 output areas identified in the NHSP log- frames. Annex 3 recommends some changes to the EHCS indicators and targets, to ensure that they are both useful and possible to measure.
19 The log-frames produced in 2004 had a logical structure that aimed at supporting improved health outcomes via actions that tackled critical constraints to improved access to cost-effective and equitable health services. However, subsequent developments in the political and institutional environment, and improved information on what interventions are effective, argue for the log-frames to be revised. The mid-term review in December provides an opportunity to do this.
Output 1 Essential Health Care Services
Public Health Programmes The analysis summarized in Chapter 3 suggests that the dramatic improvements in mortality rates in Nepal, as estimated from the 2006 NDHS, can be largely explained by the successful expansion of a small number of key EHCS services over the past 10-15 years.
Relatively successful EHCS services include family planning, EPI, CB-IMCI, Vitamin A, Tuberculosis, immunization campaigns, and antenatal care. They have either already reached very high coverage or are rapidly expanding. Pertinent characteristics of these interventions are that:- 1. They are low-cost per person covered. 2. Most of them can be delivered by the lowest levels of staff or even by community volunteers. 3. Most of these services can be scheduled, particularly those needing higher level staff, so they can be delivered by staff that are often missing from post or working short hours. 4. Most of them have long received substantial project support from a variety of EDPs and projects although all are implemented through the government’s health services, and receive increasing levels of government financial support. 5. Most are delivered free or nearly free to the user. 6. Most have benefited from attention paid to improved logistics management so that they usually have needed stocks. 7. They have had large scale effective in-service training programs for staff and BCC programs for education of the population.
The most effective ones are coordinated national programmes, managed by divisions of DOHS, delivered using Government staff, and increasingly using Government systems for planning, budgeting, procurement, service delivery, and monitoring and supervision. Some of them have in the past by-passed dependence on the GON budget for critical inputs, but this is changing. Where programs are relying on EDPs, the respective roles and contributions are identified in the AWPB. Fewer commodities are now directly procured by EDPs, although they have sometimes stepped in to help overcome crises. The share of expenditures financed from domestic budgetary resources is increasing. Although technical support is heavy in some districts, e.g. the 17 USAID supported districts under the NFHP, the geographical coverage achieved is much broader, and e.g. IMCI has been expanded to other districts using the GON budget. The judgement of
20 those we interviewed in Government and in EDPs is that the programmes are stronger because of EDP support, but they would not collapse without it.
Curative Services Curative health services have been of uneven quality and have achieved lower coverage. They require relatively high level health workers available every day (or, in the case of delivery services, even 24/7). They impose high costs on patients, either due to user charges, or due to inadequate supplies of essential drugs, obliging patients to purchase from the private sector, or due to high transport costs. As a consequence, reported outpatient contacts have stagnated at a low 0.38 contacts per person per annum. This is an under-estimate because surveys suggest about half of such visits are to non-Government providers, but only 62% of identified private and NGO service providers reported their data. Even allowing for this under-reporting, the level of outpatient consultation with modern health service providers is far short of international norms. This results in low utilisation of facilities, and staff. Similar factors result in a low proportion of institutional deliveries and relatively low rates of C-sections. There are a variety of constraints that need to be tackled via the supporting policy and institutional reforms under NHSP:- affordability and access to the poor, staff non-availability and poor motivation, problems of physical access in some areas, logistical problems, and in some cases lack of adequate budget provision for meeting the demand.
The other 7 output areas are designed to tackle some of the constraints, but the precise formulation of the measures needs to be re-visited.
Output 2 Decentralisation Decentralisation was intended to bring more bottom-up accountability to communities to give them more opportunity to tackle local problems, respond to local priorities, and hold service providers accountable to those they serve. It is seen as one important instrument for tackling the problem of absent or poorly motivated staff.
Over 1400 health facilities have been handed over to be managed by Health Facility Management Committees compared to the target for 1800 by 2006. The budget for handed over facilities is supposed to come from:-
i. The regular budget for medicines and equipment, each SHP is supposed to receive NRs30, 000 to buy medicines from the district level. The DPHO buys and sends on behalf of the SHP. ii. 5% of the VDC budget is supposed to go to the SHP, and would be worth NRs 25,000. iii. The DDC is supposed to devote 10% of the total budget to the health sector. iv. The handover was partly motivated by Government expectation that communities would be able to mobilise more funds for local health services. They currently levy registration fees for those seeking services, and those with community drug funds may raise additional resources for medicines from this source. However, the evaluation of
21 the handover reports that 60% of SHPs see no possibility of raising additional funds16.
In practice, the HFMCs have limited authority, while accountability to the community is weak in the absence of elected local bodies pending a political settlement. The evaluation found that existing clients do not believe that the HFMC represents them, not surprisingly when the chair is the Village Secretary, an employee of the Ministry of Local Government who is usually not from the village, while the Secretary is the Health Facility In-Charge. The budget flows from DDC via the DPHO and VDC before reaching the facility, and the real power remains with the health professionals. The handed over facilities report themselves to have serious financial difficulties, and nominal powers to recruit additional staff have not in practice been used. Perhaps surprisingly, the evaluation nevertheless reports that handover has produced some positive impacts on staff attitude. The impact on service utilisation is variable.
Although efforts have been made to introduce district planning, in practice the plans had little influence, and the district is mostly in the role of an implementing agent for policies and plans decided at the centre. District managers do have some authority over staff placement (they can move and second staff within the district) and have limited funds to carry out activities. District programs often receive EDP project support, occasionally in the form of district specific project staff, to help them achieve good results for EHCS programs.
The district share of the health budget has been increased sharply from 13 percent in 2006-07 to 21 percent in 2007-08. These funds may be spent at local level, but they are earmarked to policies and programmes decided at the centre. Although the funds are shown under ‘integrated district health program’ in the budget, this is something of a misnomer, since it is largely composed of the district level costs of national public health and disease control programmes. The AWPB for each of the national programmes is prepared centrally, and specifies activities and budget ceilings for the districts for programmes such as IMCI and malaria and kala-azar control. The earmarking reflects a legitimate concern that local decision-makers may focus on curative care to the detriment of the preventive and promotive EHCS programs that have reduced mortality rates17. When decentralisation to locally elected bodies is able to go ahead, earmarking may need to be maintained for some time, but should be accompanied by action to raise district and community level awareness of the importance of public health interventions, by publicizing the evidence that they are largely responsible for the dramatic declines in child and maternal deaths.
The increase in the district share also includes the budget provision for extending free basic health care, providing financial incentives provided under the maternity incentive scheme, creation of small pooled funds for community health volunteers, and provision for improvements to health facilities. It is reported that districts are uncertain regarding
16 Evaluation of decentralization Process, NHSP Chapters, 2007 17 This was the experience of a number of African countries. For a Uganda example, see Foster and Mijumbi, 2002
22 the exact procedures for using these funds, reflecting the lack of opportunity for prior planning and sensitization of staff. Similar problems have been experienced with respect to the Maternity Incentive Scheme, where the recent process evaluation identified significant procedural problems that have prevented timely payment of the incentives to those who have claimed them18.
Hospitals have been given some increased powers, mainly the power to raise revenue by charging for their services. However, Government funding continues to be tightly controlled. Although described by Government as a ‘block grant’, the budgets sent to the regional hospitals are in practice entirely earmarked, and subject to the same strict rules as other components of the Government budget. Further deconcentration to increase the delegated authority of individual cost-centers within DOHS would be very desirable, to help them to manage more efficiently the resources available to them.
More complete decentralization in the sense of devolving power to local Government is probably not possible at present pending a political settlement on the future, probably federal, structure of the state. .
Table 4: MOHP Budget by levels NR Bns 2006-07 2007-08
Amount Share Amount Share Level Growth Centre 8.02 86.89 9.57 79.13 19.37 District 1.21 13.11 2.52 20.87 108.67 Total 9.23 100.00 12.10 100.00 31.08 Source: Ministry of Finance, Estimates, 2007/08
Output 3 Private and NGO Sectors
The NHSP calls for recognition of the important role of private and NGO sectors in service delivery, defining appropriate roles for each, and proposing to work in partnership where there are benefits from doing so.
Private providers account for a substantial portion of EHCS service provision. This includes: i. Roughly half of all outpatient visits for acute illness among both children and adults are to private providers (NDHS 2006 and NLSS 2004). This includes private pharmacies, which provide diagnostic services as well as drugs: - nearly two thirds reporting taking a sick child to a pharmacy report that the child was examined (NDHS, 2006). Private sector use increases with wealth. Government services are used at similar rates by most wealth groups, but less by the wealthiest.
18 Powell Jackson et al, 2007
23 ii. Most patients see private providers in urban areas and the Terai. In the rural hills and especially mountains public providers (and FCHVs) are more popular. iii. About one-quarter of facility based deliveries are in NGO or private hospitals (NDHS 2006) iv. Since abortion was legalised in 2002, more than 80% of women receiving comprehensive abortion care have used private or NGO facilities (Box 4.1) v. NGOs or private entities provide a substantial minority of family planning services (nearly 10% of sterilizations, 18% of injectables, 50% of oral contraceptives and 70% of condoms) (NDHS 2006) vi. Since 2004, four district hospitals of total 60 bed capacity have been added to the public system but in the same time more than 600 additional beds have been added in the urban area based private hospitals. vii. The majority of Doctors graduating in Nepal do so in private medical schools. As part of their agreement with Government, a percentage of places are reserved for Nepali students, including 20% of places made available free to students nominated by Government of Nepal.
Box 4.1 Comprehensive Abortion Care Abortion was legalised in March 2002 if undertaken by Doctors who have completed NHTC training. Abortion is available at a cost of Rs1000 from listed public or private service providers. Listed service providers include district hospitals and above, while private service providers include clinics run by Marie Stopes International and the FPA as well as private for profit providers. Over 80% of legal abortions take place in private or NGO sector facilities. According to DHS, 3% of women reported having had an abortion in the previous 5 years, but rates are higher in urban areas (5.7%), and among women in the highest wealth quintile (6.6%) and with SLC and above education (6.6%). Only one third of women knew that abortion was legal, and reporting is likely to be underestimated. The policy is seen as having been successful in reducing deaths from unsafe and illegal abortion, but there are issues of physical and financial access for poor and rural women.
A number of contractual and informal partnerships exist with private and NGO partners. For example, the logistics management division contracts to private companies for transportation of drugs from central to regional and district stores. The child health division contracts with private organizations for CB-IMCI training. Manipal private teaching hospital gains access to sufficient beds to support their teaching by an arrangement with the Western Regional Hospital, paying for access to WRH patients and providing eight full-time staff. This mutually beneficial arrangement enables WRH patients and staff to gain access to additional highly qualified staff and specialist facilities, while the teaching hospital avoids the need for investing in additional beds in a city that already has relatively low bed occupancy. Even in this case, where the mutual benefits are self evident, negotiation of a new contract is proving difficult, with WRH
24 pressing for higher payments, while Manipal is concerned that Government has not complied with some aspects of the original agreement.
Much of the work of EDP funded projects also involves contracting with organizations to carry out work on behalf of the government program. Surveys, research studies, BCC campaigns and many training activities are contracted out to local companies. Even the DHS survey is implemented by a local private company. Community mobilization activities for health are usually contracted to local NGOs in the districts involved. Many projects, through their own staff, provide technical assistance at the national level and managerial support at both national and district levels. For some specific EHCS activities, such as for HIV control, a large number of local NGOs provide a range of services from counseling of high risk groups, to testing, to care and support for persons living with HIV/AIDS. Many of these services are either not available from government health services or are not located and targeted to deal with specific risk groups.
The private hospitals association has suggested a scheme for short internships, with junior staff seconded to regional or district hospitals in rotation for a period of two months or so, under the supervision of a more experienced staff member. The idea would be to provide access to some more specialist care at local level, and help upgrade the skills of the Government staff, while the private hospitals would gain from giving their staff useful experience. The private hospitals would provide the services of their staff free of cost, although there would be implications for accommodation and equipment and medical supplies. The suggestion is certainly worth exploring. A similar support role could also be envisaged for the regional and zonal hospitals with respect to district hospitals in their area.
The existing examples of Government contracting out in Nepal generally relate to quite specific functions where it is straightforward to define outputs and performance standards; a longer term contractual relationship to provide health services or manage a hospital presents a more complex challenge in defining what is to be delivered by the contractor, what support will be provided by the Government, and what processes will be established for adjudicating disputes. The log frame targets do not capture the wide range of existing and proposed partnership arrangements. They instead focus quite narrowly on the specific, and quite complex, model of service delivery agreements between GON and private or NGO partners, with the GON budget being used to procure services from non- Government service providers where they have capacity to provide those services more cost effectively. The targets envisage contracting out the management of complex clinical services, such as hospitals. It is not clear how this model serves the objective of expanding access to quality EHCS. GON lacks capacity to frame, monitor and supervise the necessarily complex contracts for service provision. It runs the risk that badly framed contracts may not deliver what is wanted at a price that reflects a fair balance between risk and reward. Any private partner taking on a service contract at present would need to factor in risks related to GON management of the contract: - disputed assessments of their performance and of the amounts to be paid, failure to pay in full and on time, inability of GON to fulfil their own obligations under any contract, and risks associated with current political uncertainty. GON faces risks of protracted and complex tendering
25 and negotiation processes, and of poor performance by contractors, possibly leading to costly legal action to resolve disputes. After potential contractors factor these risks into their tenders, the offer price may be unattractive from the point of view of GON.
We suggest dropping targets for handover of a specific number of facilities in favour of a more pragmatic approach in which institutional arrangements are derived from consideration of the best way to achieve health outcomes, given the public and private resources that are likely to be available, and the political and institutional constraints on policy choices.
Where contracting out is the best technical solution, a pragmatic alternative in the short term is to let the EDP or its project carry on doing the contracting, but with MOHP/DOHS taking a strong coordinating role for the program area to ensure that the contracting supports the government program. There are several EHCS program areas in which the close working relationship between the government and external partners shows how this can work. It is particularly relevant in cases where the form of contract envisaged would be a new development for MOHP, and where international experience may add value in developing a workable approach before GON takes on full responsibility. The main concern in the medium to long term would be the issue of sustainability. This need only be a concern in the case of long-term service agreements, where GON will need to take on the responsibility as and when the EDP phases out.
Output 4 Sector management The sector management outputs envisage moving towards unified sector-wide planning, programming, budgeting, financing, and performance management to support service delivery, supported by the EDPs and involving NGOs and the private sector. They also envisage restructuring of MOHP to support this more unified approach, with the expectation of efficiency savings being realised.
The specific verifiable indicators focus on activities that imperfectly capture what the output area is intended to achieve, and may actually undermine progress. Completion of a large number of organisational reviews, for example, need not indicate any progress in actual re-organisation to make an MOHP that is fit for purpose, but will absorb limited capacity. In May, MOHP called for bids for five reform agenda related studies. According to the TORs, these would require MOHP senior officials to provide their time for 35-40 workshops of varying durations. It is unhelpful that studies of organisational reform have been divided into separate Vertical, Horizontal and Functional studies, while HRM related studies have been divided into Needs assessment, Training Plan, and HR plan. The contracts have gone to different consultants, resulting in a lack of coherent vision for the reform of MOHP, and leaving MOHP with a very difficult task of making sense of it all and deciding what to do with conflicting recommendations.
The real progress that has been achieved is not reflected in the indicators. At programme level, there are some excellent best practice examples of joint planning and programming of resources, with programmes being scaled up using a common approach supported by GON and EDP resources, following a successful period of piloting. At sector level, the
26 DOHS has a good annual process for reviewing performance against the targets set in annual workplans, starting with regional reviews that are then reflected in the annual review and departmental report, identifying constraints that need to be overcome. The main weakness of the MOHP/DOHS review process is that the findings from the annual review held in October-November are not then systematically carried forward into preparation of annual work plans and budgets for the following year, although they clearly will influence the planning process.
The NHSP process sits rather uncomfortably outside the long established national GON processes for planning, budgeting, and progress review. The most significant donor interactions on the content of the annual work plans, and how they can be financed, take place at division and programme level, largely independent of NHSP.
The successive JARs have complained at the lack of progress on the management outputs listed in the logical frameworks or agreed in previous aide memoires. The sector management reforms on which the JARs have focussed attention are clearly beyond the capacity of a two person reform unit to implement, or ensure that others implement. Some significant action has been taken by MOHP to enhance the capacity of HSRU over the last year. A Joint Secretary has been assigned to lead the unit as 'Chief Coordinator', and another MOHP staff member has been assigned to the unit. TA support provided by DFID is working closely with HRSU, and is now physically located within MOHP. These changes and new arrangements are expected to provide additional drive to the reform agenda.
MOHP has been effective in implementing public health programmes, but has not implemented the necessary reforms to build effective institutions for delivering basic curative and safe motherhood services. These pose a more difficult set of challenges to overcome entrenched opposition and change the organisational culture as well as the structures. In a turbulent political situation, NHSP-IP may not have consistently enjoyed the level of political commitment and bureaucratic ownership that would have been required to drive the reform process forward.
Output 5 Health Sector Financing
Health Sector Budget GON has approved a 2007/8 budget in which health (or rather MOHP) has a 7.2% share, continuing the upward trend since NHSP started in 2004/5. MOHP is on track to reach the targeted 7.7% share in 2009, although the appropriate health share ought to be a national decision taken by politicians: - there is no technical justification for the EDPs pressing on the Government a particular view as to what is the appropriate share. The only basis for such an agreement might be a donor desire to ensure that funds committed to health result in additional health expenditure. This would require a rather different approach to framing the indicator, and could still be objected to on the grounds that the health spending that GON might have undertaken without the aid can not be known.
27 Table 4.1: Health budget as a percent of national budget Total National Budget ( Billion Health Health Budget NRs) Budget Share % 2004/5 111.690 6553 5.86 2005/6 126.885 7555 5.95 2006/07 143.912 9.230 6.40 2007/08 169.000 12.099 7.16 Source: MOHP, Budget Analysis 2007-08
The donor share of HMGN budgeted health spending was just 13% in 2003/4, before NHSP started and when a large share of health expenditure was not captured in the budget. It increased to 42% in 2004/5, with the inception of NHSP and the start of pooled funding, and has been 51% in the budgets of both 2006/7 and 2007/8.
MOHP and the NPC are trying to capture all external assistance to the health sector within the budget, and the budget for 2007/8 reflects the full value of external donor commitments included in the MOF source-book (the ‘White Book.’) This is in contrast with earlier years. In 2005/6, the FCGO report on actual expenditure recorded 5.19bn of aid to MOHP, compared to just 3.22bn budgeted19. It is clearly easier to plan if donor support is fully taken into account, and the AWPB contains a useful analysis showing not only what aid is expected, but also where it is expected to be disbursed. Communication between MOHP and EDPs seems to be a problem:-the pool fund donors have committed just NRs1.4bn, but the approved 2007/8 budget assumes NRs2.7bn in pooled funding. (Table 4.2).
Table 4.2 MOHP Budget and Spending 2003/4-2007/08 (NR m) Source of 03/04 04/05 05/06 06/07 07/08 Finance Budget Spent Budget Spent %Spent Budget Spent %Spent Budget Budget 5,920 GON 5,354 3,451 3,812 3,117 82% 4,340 3,847 89% 4,516 $92.5m 2,691 Pooled Fund 953 690 72% 1,630 943 58% 1,649 $42m GON plus Pooled 8,611 Fund 3,451 4,765 3,807 80% 5,970 4,790 80% 6,166 $135m 3,488 Non-Pool 517 1,789 5.65 44% 1,585 1,045 66% 3,064 $54.5m 12,099 Total 5,354 3968 6,554 4372 70% 7,555 5,835 77% 9,230 $189.2m % increase in spending, GON+pool 10.30 25.85 39.7 Pool% of GON+pool spending 18.13 19.70 31.30 MOHP as % of Government 4.93 4.44 5.87 4.57 5.95 5.20 6.40 7.16 Source: DFID/WB calculation from GON sources
19 Government of Nepal, Consolidated Financial Statement, 2005/6, Financial and Comptroller General’s office,2007
28 It is difficult to provide an accurate analysis of what share of the budget uses harmonised systems. The pooled fund on Government assumptions will be 22% of total expenditure in 2007/8, and a number of other major donors use a reimbursement methodology that relies on the Government to account for expenditure, while most external support is at least jointly planned. None of the donor support is fully aligned with GON systems, including the pooled fund. The pooled fund relies on Government expenditure data collected by the FCGO, and reimburses a share of the total Government spending, but the Financial Monitoring Reports and procurement reports that are required by the pool donors in order to claim reimbursement have features that are additional to the reporting that Ministry of Finance requires for its own purposes.
Using an agreed definition, MOHP has allocated 70% of the budget to the EHCS in both the 2006/7 and 2007/8 budgets, in line with the NHSP target. The strong public health orientation of the NHSP is reflected in the high share of preventive programmes in the total budget; nearly 64% is directly allocated to preventive programmes, before considering the extent to which they also benefit from central expenditures on procurement, monitoring, and other management services. Although the curative share in the budget increases in 2007-8, this mainly reflects spending at district level. Recurrent spending increases include provision for the extension of free basic services, as well as payment of maternity incentive scheme payments. Capital spending includes creation of new BEOC and CEOC centres, and up-grading of sub-health posts.
Table 4.3: Budget analysis by types of services and types of inputs
2006-07 2007-08 Types of services Recurrent Capital Total Share Recurrent Capital Total Share Budget for curative 1.25 0.79 2.04 22.1 2.553 1.343 3.896 32.20 Budget for preventive 5.32 0.56 5.89 63.8 6.227 1.460 7.687 63.53 Others (health system, monitoring evaluation) 1.24 0.06 1.30 14.1 0.392 0.124 0.516 4.26 Total 7.82 1.41 9.23 100 9.172 2.927 12.099 100.00
Source: MOHP, Budget Analysis 2007-08
Actual spending by MOHP in most years falls significantly short of the budget, with the outturn typically less than 80% of the sums allocated. Most of this appears to reflect problems in spending donor money, although GON financed expenditure has also been less than 80% of the budget. The implementation rate has improved consistently since 2004/5, and is expected to have exceeded 90% in 2006/7 (final figures are still being reconciled). The improved budget outturn that seems likely to have been achieved in 2006/7 is said to partly reflect high level attention by Minister and senior officials to budget monitoring, as well as an early start to AWPB finalisation and fund releases. It seems unlikely to be repeated in 2007/8:- advocacy for a larger MOHP budget delayed reaching agreement on ceilings, and districts received their spending authorisations late.
NGO spending and spending undertaken via private partners (for example, the social marketing programme) are not currently captured. This is reasonable if the SWAP is
29 conceived of as a programme to support public expenditure plans for health that are framed within a clear set of policies and regulatory structures that allow an appropriate role for other partners, but do not require everything to be planned or centrally coordinated by a centralised Government department. MOHP does need to be aware of NGO proposals, and to ensure that they do not distort the allocation of spending between districts, or undercut Government policies: - for example, the AWPB mentions an MSF project providing free drugs in a district and thereby undermining efforts to develop the CDP20. There are diminishing returns from trying to centralise or even monitor everything, but MOHP does need to regulate in general terms the policy environment within which other service providers must operate, and has a role in steering NGOs towards underserved districts and towards issues where further support would be welcome.
Action is still pending on a needs-based resource allocation system, understandable in the current delicate stage of negotiations regarding the future federal structure of the state.
Aid Coordination and Harmonisation Although MOHP are now including all donor support to MOHP within the budget, some of it is provided using parallel arrangements for planning, disbursing, and reporting on the aid, and Government may have incomplete information on how aid is being used. The main problems that could result from this are:-
i. Donors financing activities that do not form part of the GON plan, and that GON would not have chosen to finance, or would have provided for at lower cost. This is probably the case with much of the technical assistance being provided by the EDPs, both at central and at programme level. ii. Donors financing projects that impose high management costs but achieve low coverage, and are neither sustainable nor replicable. They impose high transaction costs through duplication of training and workshops that take staff away from their jobs, multiple reporting systems, reviews, etc that absorb scarce management attention. iii. Donors financing activities using project funds that are not sustainable beyond the project life, and that Government becomes dependent on. The danger is that key functions may collapse when EDP support is withdrawn, because Government has not developed the capacity to undertake the task and has not made budget provision for performing it. Usually, the problem is that the donor has stepped in because GON systems can not handle the particular issue, solving the problem in the short term, but possibly delaying pressure for a more durable solution. iv. Donors supporting inconsistent approaches, causing confusion and poor sustainability. v. Donors undermining public sector management by paying incentives to staff, who may then be unwilling to work without them. vi. Donors undermining capacity building and ownership by doing too much on their own responsibility, leaving no space for local staff to develop.
20 AWPB, page 148
30 Although all of these problems are present to some extent, the good coverage achieved by public health interventions was based on good coordination on programmes that were scaled up to reach national scale with coordinated support from GON and EDPs, using mostly GON staff. Donor involvement has been long standing. Although programme level TA has been heavy in some programmes, for example the US supported NFHP, districts that have had lower support have also shown reasonable results, and the consensus is that the national programmes would be weakened but would not be destroyed if assistance were scaled down. GON logistics and procurement functions have been strengthened, and are capable of sustaining the programmes. Although there are examples of additional reporting called for by specific programmes, EDP supported national programmes have tried to work with the NHMIS that they helped to develop. There are certainly problems of duplication in some areas, especially training. However, if some EDPs must provide their assistance via parallel routes, the major public health interventions in Nepal provide a good model for how to do so while minimising the negative impacts on sustainability. The results achieved, built up over a long period of piloting and scaling up, speak for themselves.
Transparency of the Budget The structure of the MOHP budget would benefit from an effort to improve the transparency with respect to how important expenditure programs are reflected. The costs and budget provision for major new policy initiatives is invisible both in the detailed line item budget and in the separate annual work plan and budget. The most important example, discussed below, is that the budget provision for free basic services can not be identified in either document, other than a tiny provision under management division for supervision and monitoring of the policy21. As far as we could detect, the free basic services policy receives no other mention in the AWPB.
Output 6 Logistics Management The new procurement law that was passed in January 2007 reflects international standards of fair competition and transparency. The challenge is to ensure that it is effectively implemented.
There were significant procurement problems in 2006/7, including failure to complete some routine vaccine procurements. Indeed, the 2007/8 AWPB reports that only 23 from 56 drug tenders could be awarded, attributing the problems partly to problems with the introduction of the WHO GMP provision, adding to the time taken to procure. The AWPB also mentions problems of late start to the procurement process, with technical specifications and cost estimates not reaching logistics management division until the third quarter, due to the usual problems of late receipt of budget authorisation. This increases the risk of procurement not being completed and the budget having to be returned at year end, especially if ‘no objection’ certificates are also required from the financing donor. The logistics function thus remains prone to serious risks that vital inputs may not be procured in a timely fashion.
21 AWPB page 33.
31 The consensus of those we spoke to is nevertheless that the problems experienced in 2006 reflected unfamiliarity regarding new procedures, and a general reluctance to take responsibility for decisions at a time when anti-corruption agencies were taking a harsh line with perceived wrongdoers. Logistics management and procurement functions have been strengthened with donor support, and further support is envisaged.. The work plan for technical assistance from RTI includes provision for orientation training on the new act, and the development of a manual for implementing it fully within MOHP. In recent months, things have run relatively smoothly, and there are no current supply problems or looming difficulties in the pipeline of future supplies. The regional review meetings that were underway at the time of the mission are reporting a significant improvement in the drug 'stock out' situation, something that is also evident in LMIS reporting data.
Logistics for most EHCS programs is adequate, although constant attention is needed to ensure minimal disruptions of supplies. “Program commodities” include:
a. Family planning commodities (condoms, pills, injectables, IUDs, Norplant) b. Vaccines (BCG, DPT or DTP/HepB, Polio, Measles, TT) c. Vitamin A capsules and deworming tablets d. Maternal care (iron/folate) e. Sick child care (ORS, pediatric cotrim) f. Tuberculosis, leprosy and kala-azar drugs. g. Insecticide for household spraying for malaria. h. HIV (this area is just starting to develop but includes ARVs and test kits).
With the development of EHCS programs, more items may eventually join the “program commodity” list and receive more attention to constant supplies. Examples include: i. Safe motherhood supplies (e.g. oxytocin, Mg Sulfate) j. CB-MNC supplies (e.g. misoprostol, injectable gentamycin)
Beyond the list of “program commodities” for most EHCS services, there is the list of “essential drugs” with separate lists for SHP, HP and PHC level of 50 to over 100 items. Program commodities are generally available in sufficient quantity, but the funds available to purchase essential drugs are limited, so that stock outs are common in health facilities22. Stock outs are exacerbated by the traditional method of distributing essential drugs, in which facilities receive an annual allowance based on the type of facility and geographic region, which often contains too much of a few items and too little of most others. Many facilities have had to simply refer patients to pharmacies to buy their own drugs.
There are several reforms in the logistics systems to improve provision of essential drugs. The first is a “pull” system at the district level in which essential drugs are allocated to health facilities according to demand rather than by formula. This allocates supplies better between facilities, but does not solve the problem of overall low quantities
22 Source, drug availability survey, confirmed in discussions.
32 purchased. In the district we visited, the ‘pull’ system is only being applied to the relatively small quantities of locally purchased drugs. The centrally purchased drugs come in boxes, and the district store was reluctant to break them down and allocate specific drugs according to demand: - each facility was still receiving the standard box of essential drugs on a fixed schedule.
Community drug programs allow health facilities to establish a revolving fund to buy drugs for sale to patients, and thereby maintain a stock of all essential drugs. In well operating schemes the facility is able to negotiate favorable prices for buying drugs, and can sell them at substantially less than private sector prices. Users have attributed low prices and improved quality of drugs as benefits of the CDP.
The Ministry of Health has mentioned a plan by which the Logistics Management Division would do central tendering for essential drugs, but would allow districts to buy the quantity of drugs they wanted from the winning bidders at a fixed price. It is hoped that this would result in a combination of a good price obtained from large scale tendering, with freedom of districts to spend their essential drug funds as they wish and to adjust the drug supply to fit to the local needs. Again, while this may improve essential drug supplies, it does not solve the problem of inadequate total funds for essential drugs. This system may also make the districts more accountable for their drug supply with more autonomy; however the quality control of the locally supplied drugs needs to be given some serious thoughts.
Introduction of free services will only result in significant improvements to access if Government provides significantly increased funds for purchase of essential drugs in the district budget. If this is not done, ‘free’ services will be frustrated by drug shortages, resulting in patients still needing to incur the cost of buying prescribed drugs that are unavailable from the facility.
Physical Facilities The equipment and physical facilities of the majority of the health facilities at district and below level are substandard, very old and insufficient. The challenge is to put significant one time capital investment to upgrade these facilities to an acceptable level. The maintenance plan that was recently completed may help in prioritizing the need for re- habilitation and upgrading of facilities. An inventory and a physical upgrading plan will be important aspects of the required preparation process for the next NHSP.
There are plans for improvements to health facilities, mostly to allow them to become birthing centers or EOC centers. This needs to be well coordinated with staffing plans and financial reforms to be successful. The effectiveness of these services depends upon the health institutions providing quality care with skilled staff available 24/7, and with the facility making available the promised free services and timely and transparent financial support under the MIS. These supply side measures need to be accompanied by awareness-raising, to ensure that households have accurate and complete information about the services that are available, and the benefits of using them. FCHVs and mothers groups are key instruments for spreading the word.
33 Supplies of furniture which are locally available (in particular wooden furniture) are also being centrally supplied. They can stay in store for long periods before being sent to the district23. In route damage is very common in such supplies and because of the transportation cost they might be more expensive compared to the local market price of the same goods.
Output 7 Human Resource Development Within the MOHP, the HR functions are divided between three different divisions. (Personnel Administration, Training, and HRMIS). The HRMIS is still not fully functional (as filing of personnel data by about 8000 of the roughly 30,000 individual staff is lagging behind) and no linkage has been established between the other two functions. Simple information on the current total number of approved and filled positions is not readily available from the HRMIS system.
The main staff shortages are for Doctors, roughly 50% vacancies reported in the 2005/6 annual report, and nurses, who work mainly in hospitals and PHCCs, where 50% of established posts are vacant. In contrast, over 90% of the positions for Auxiliary Health Workers, Auxiliary Nurse Midwives, village based health workers, and mother and child health workers are filled. These are the core of the primary health care system, staffing the health posts and sub-health posts, and mainly responsible for implementing the public health interventions, together with the 50,000 unpaid female community health volunteers.
Some useful practical steps have been taken to overcome staff shortages. Recently 100 doctors have been appointed as permanent staff and about 105 doctors have been also appointed on contract. This will go a long way towards filling the 300 vacant positions for doctors reported in the 2005/6 annual report. PSC is about to start recruitment for about 600 paramedic staff (Nurses, AHWs and others). At regional level, initiatives have been taken to appoint medical personnel as temporary staff in the approved vacant positions. Where the CSC has been unable to recruit, the Regional Directors are authorized to appoint temporary or contract staff using the salary provision in their budget. The RD needs episodic authority to do this from DOHS, which may have been an impediment to using this power as widely as would be justified.
Graduates from the eight medical schools who received Government scholarships (roughly one hundred per year) are now posted to work for two years in Government health facilities in the districts before they are granted their licence to practice. At the time of writing, 75 medical officers were posted to work in PHCCs and hospitals under this scheme. This is helping to reduce the lack of physician staff in those areas, but does not provide some high level skills such as surgery, and the inexperienced MOs will require supervision.
Ensuring positions are filled may not mean that staff are physically present and working at the times when facilities are supposed to be open. More effective performance
23 Foster and Regmi, 2006, quoting NAO audit report
34 management is limited by low per diems and late budget authorisation, making supervisors reluctant to make field visits. Introduction of an effective performance incentive scheme would help. This will need to be developed through a broad consultative process that draws on models that have been verifiably successful in other countries, and it would need to be piloted before national introduction. A carefully designed three district pilot was abandoned due to MOF not releasing the required budget in 2006/724. The pilot should be re-started, adapted as necessary for the changed context of free essential services, and should be fully funded.
Current policy is to provide larger numbers of skilled birth attendants in rural areas and staff for BEOC and CEOC facilities. This needs to be carefully coordinated with the other requirements for improving delivery care, since provision of staff by itself may have little impact. Other aspects include facilities and equipment for deliveries, reduction of financial barriers, incentives to staff to want to have a busy delivery service, and available referral systems to the facility and to higher levels when needed.
MOHP staff and the EDPs have expressed concern about the high level of transfers of staff at all levels, many of them done outside the basic rules and norms of transfer as per the health act, which specifies a 2 year minimum posting. They are especially damaging for managerial and administrative positions at district, region, department and ministry level, creating discontinuity and hampering the programs and activities.
Output 8 Health Management Information System The HMIS provides reasonably accurate data for most EHCS programs. It is supplemented by a number of surveys, in particular the NDHS every five years.
Although the focus of the HMIS and Annual Report is on HMIS collected data and on process targets for program areas, it would be useful if the program chapters took a more comprehensive view of their programs, bringing in data from surveys or other sources and describing the mix of activities under their program, including EDP project activities.
The pilot improvement in the HMIS in three districts includes disaggregation by ethnicity and other minority groups, and six monthly reporting of facility staffing levels, which will provide a useful and timely source of information on human resources. There is a strong case for extending this to all districts, given that this information is crucial for management purposes, and is not likely to be available from HURDIS any time soon. There is also a strong case for reporting more gender-disaggregated data, the current system does not for example identify whether OPD patients are male or female, which would be useful for assessing the extent of gender bias in access.
The other major weakness is that little attention is paid anywhere in the management and review system to relating operational statistics to financial data on expenditures. This is difficult to do with the existing structure of the budget. A strengthened capacity in health
24 MOHP, Piloting of Performance-based Management System in Ministry of Health and Population, Highlights of Activities and Draft performance Improvement Plan for Sub-Health Posts, February 2006
35 economics is now available via the RTI, which may be able to analyze the available data in order to try to draw some clear conclusions on issues of cost-effectiveness and the efficiency of resource allocation. However, sustainability is an issue given the lack of local counterparts with a health economics background.
Overall Judgement on NHSP Progress at Mid-Term The NHSP can not take credit for the excellent progress in reducing mortality levels, but it has contributed to sustaining and expanding the public health programmes that have delivered the good results. There has been progress in raising the health share of the Government budget, and progress in continuing to concentrate spending on EHCS. Pooled funding delivered via the budget has enabled Government to expand the IMCI to more districts, using budgetary resources and Government systems. This has improved sustainability, with 60% of the costs of IMCI now born by Government. Budget implementation remains a concern, but has improved each year since NHSP started.
Some aspects of the reform agenda have made good progress. The HMIS produces detailed data down to district level, and is linked to an annual review process in which district managers are encouraged to identify constraints to programme performance and propose solutions. There are significant gaps in coverage and a lack of disaggregation of patients by gender and other characteristics, but the required improvements are being piloted. Although the progress may be fragile, the consensus view is that logistics management has improved as a result of sustained support to systems improvement and capacity building, and there are no current problems in the drugs and commodities pipelines.
Other output areas have made little progress in achieving their targets, some of which have been rendered irrelevant by the evolving political situation and changes in both Government and donor policy. Decentralisation as conceived can make little progress at present. The types of public private partnerships that can best contribute to improved health outcomes are not well captured by the current output targets and indicators, while the movement away from user charges represents a reversal of the targets for local resource mobilisation that were set out in NHSP-IP. The human resources management and overall sector management outputs have not been achieved. Some of the key constraints require action that lies beyond the remit of the MOHP. After three years of little progress on recommendations that have been repeated at each JAR, it is important to re-think the priorities and focus on a limited agenda of reforms that are feasible to achieve and will contribute to sustained delivery of improved health sector outcomes. Discussion of what those priorities might be is the focus of the remainder of this report. 5. Priorities For The Future
5.1 Opportunities For Further Progress In Reducing Mortality
Maintaining, Refining, Expanding Successful Programs First priority is to maintain and build on the success that has been achieved:
36 - CB-IMCI. This program is already scheduled for expansion to national coverage within two years. Program modifications in terms of zinc for diarrhea and revised guidelines for treatment are also being introduced and scaled up. - - EPI (new vaccines). The EPI program is steadily adding new and improved vaccines to the current successful structure for delivering immunization services. This expands the program in terms of content and impact rather than coverage.
- Vitamin A and Deworming. The current system reaches about 90% of the target group with good equity.
- Periodic immunization campaigns (measles and polio). The second dose measles campaign needs to be repeated about every five years to keep measles circulation in Nepal at a minimum. The polio campaigns are needed to minimize importation of polio from India.
- Tuberculosis and Leprosy programs. Both appear to be very good at successfully managing patients and reasonably good at case finding.
- HIV. There are an array of programs for prevention, diagnosis and care for HIV at various stages of expansion. Some programs for prevention in high risk groups have held infections down in these groups for 10 years, while other programs (e.g. ARV treatment) are still developing. ARV treatment is very expensive, and would not form part of a care package aimed at saving as many life years as possible with available funding. Subsidised ARV treatment should only be embarked on with clear commitment by donors to maintain funding for anyone started on treatment until the end of their life.
- Family planning. The programme has been successful in rapidly expanding coverage, but now needs to focus on the poor, reducing the substantial gap between their desired family size and actual fertility.
There are a number of health programs beyond this list which are important, but which do not have the large mortality impacts of the programs listed above (e.g. Malaria, vector borne diseases, salt iodization, etc.).
Maternal and newborn care Over half of Nepal’s under five mortality is now in the newborn period, and among EHCS programs, progress in terms of high level maternal care has been the slowest. The area of Maternal-newborn care is the most in need of new models which have the promise of addressing limitations in this area and greatly reducing mortality.
High-level maternal and newborn care covers the array of activities to improve the use of skilled birth attendance, facility based deliveries and emergency obstetric care for those who need it. Although usually called “safe motherhood” programs, they also benefit newborns. There are several initiatives addressing this topic, including:
37 - Programs to upgrade existing workers to SBA levels and recruit new SBAs. - Upgrading of facilities as birthing centers, BEOC and CEOC sites. - The MIS “Maternal Incentive Scheme” to reduce financial barriers for SBA and facility based deliveries. - Measures to reduce patient charges for all maternal care in selected areas. - Expansion of quality comprehensive abortion care - A variety of promotional programs for the public.
It appears that some progress is being made through these initiatives. The exact combination of measures that will be successful and sustainable in different parts of Nepal is only gradually becoming clear. The government needs to support continued testing, expansion and revision of these program elements to produce a successful maternal care system.
The Department of Health Services (CHD and FHD) have also been supporting a variety of community based programs to improve essential newborn care, prevent post-partum hemorrhage and improve the identification and management of newborn infections. Although these programs also encourage high level care, they provide benefits to mothers and newborns even if high level care is not accessed and so can help fill the gap while Safe Motherhood services are expanded.
Several of the district level trials have been successful with evidence of substantially reduced maternal and newborn mortality, although each trial offers a somewhat different mix of services. The DOHS is working to create a standard which will be spread to more than ten districts over the next year, while being further refined and adjusted. While most of the additional expense for this first phase of CB-MNC expansion will be supported by EDP projects, support for additional expansion throughout Nepal will require increased government funding.
Malnutrition A program to greatly reduce general malnutrition in children could have a large mortality impact. The problem is not mainly related to lack of food but to feeding practices. There are no good large scale models of how a programme to tackle malnutrition through the health services could work in Nepal, although UNICEF are about to start work with the MOHP on a pilot project in the terai25, drawing lessons from a number of African experiences of treating severe and acute malnutrition. The aim is to develop a cost- effective approach for subsequent scaling up.
Beyond EHCS The Government role in financing secondary and tertiary care is necessarily limited with a budget per head that is barely sufficient to finance public health interventions and basic curative care. The task for Government is to decide what limited services it needs and can afford to finance, and how best to procure them, which is likely to imply some partnership with the private sector institutions that are providing a large share of specialist care and are training the majority of doctors. There appears to be no case for
25 Community Based Therapeutic Care.
38 new Government investment in referral hospitals: - national occupancy is below 50%, with spare capacity in all regions (although some individual hospitals are heavily utilised). The private sector has added 600 new hospital beds since 2004.
According to the WHO, the referral system in practice provides very limited access to secondary or tertiary care, especially for those from remote areas26. One possibility as funds permit would be to meet the cost of referrals from district hospitals at agreed rates, allowing referrals to private sector hospitals when appropriate. This benefit should be means tested.
A significant share of doctors in the public sector work in the regional and zonal hospitals. With many of these hospitals relatively under-utilised, it might be questioned whether MOHP is making the best use of this precious resource. The private hospitals have proposed a scheme whereby their doctors and specialists might be seconded to district hospitals for short periods of up to two months, benefiting the staff and patients at the district hospital while also giving supervised experience to their junior staff. This idea is well worth exploring, though the costs would need to be carefully assessed. If feasible, a similar approach would be equally or more relevant for regional and zonal hospitals, who presently have no real relationship with the district hospitals in their catchment area.
Nepal has been largely successful in resisting pressures for higher spending on secondary and tertiary care, spending 70% of the budget on essential services and nearly two thirds on preventive care. However, there have been some recent increases in spending on tertiary hospitals, confirming that it is not immune to such pressures. The national hospitals have a degree of autonomy under hospital boards, but this could be further developed, providing them with a fixed block grant while leaving them free to mobilise their own resources in competition with the private sector. The aim would be to avoid the risk of ‘raids’ on public funds to finance expensive ambitions of the tertiary hospitals, while giving them the freedom and the incentive to make efficiency savings and find innovative ways to finance their own development.
Another tactic for reducing the political pressure for spending on tertiary care is to develop health insurance within the formal sector of the economy, possibly including the civil service. This will provide a mechanism for the better off to spread the financial risk of a catastrophic illness requiring expensive treatment.
5.2 Improving Access by the Poor and Socially Excluded
Evidence on Inequality in Health Outcomes Under five mortality is lower in urban than rural areas, in the hills and terai than in the mountains, in the East and Centre than in the mid to far West, and among the rich than the poor (Table 5.1). Education of the mother, age of mother, birth spacing, and avoiding too many births have a significant impact in reducing under 5 mortality. Education for girls and meeting the unmet demand for family planning can therefore be expected to have a significant impact on child mortality.
26 WHO 2007, working paper for IHP proposal.
39 Poor and rural people have higher fertility and lower CPR.
Table 5.1 Inequality in Under 5 Mortality Under 5 mortality rate Urban 47 98 Rural Hills 62 128 Mountains Mid West and far West 100+ 60 East Poorest wealth quintile 98 47 Wealthiest quintile Mother with no education 93 13 Mother with SLC Boys 80 78 Girls 7th+ birth 136 64 2nd-3rd Mother over 40 130 67 Mother 20-29 Less than 2 yrs since previous birth 130 37 Over 4 years Total Fertility rate Mountain 4.1 3.0-3.1 Hill and Terai Use of modern FP Far West Hills 26% 65% Far West terai Source: DHS
Women are no longer disadvantaged in health outcomes. Under 5 mortality is now lower for girls than for boys, differences in boy-girl malnutrition have reduced since 2001, and 15-49 mortality for women is now 16% lower than for men as a result of a 43% reduction for women compared to just 18% for men.. In this age group, mortality among men is now 2.42 per 1000 compared to 2.09 for women. Maternal mortality accounts for 18% of adult female deaths, and accounts for female death rates being higher than those for men in the 25-39 age group. A large part of the explanation for the steep decline in death rates among women is reduced fertility (reducing the lifetime risk of death in childbirth), and lower maternal mortality. Reductions in maternal mortality have benefits also to newborn and neonatal death rates and to household health and welfare, but the same may also be true for adult males, who are likely to be the main source of income for the household. The causes of the excess in male deaths are not discussed in the DHS. Some may relate to the effects of conflict, but it would seem on equity grounds to be worth giving more attention to understanding the reasons.
Table 5.2 Moderate to Severe malnutrition: % of Children More than 2 Standard Deviations Below Average Height For Age Weight For Height Weight For Age 2006 NDHS Boys 49.0 12.9 37.5 Girls 49.6 12.3 39.7 2001 NDHS Boys 49.5 10.7 46.6 Girls 51.0 8.8 51.0
40 Source, NDHS, Table 12.11 and World Bank op cit Table 8.11
The DHS collected data by religion and ethnicity, but it has not yet been analyzed. Earlier surveys found significantly higher rates of malnutrition among Dalits and other minority groups, and among the terai middle castes. According to CLSS 1, infant mortality among Brahmans, Chhetris and Newars was significantly lower (52.5 and 56 per thousand) than the then national average of 84. Under 5 mortality among Dalits was 171, compared to the national average of 10527. The differences are greater than can be explained simply by differences in poverty between groups. It will be important to analyze the 2006 DHS data, in order to determine whether there has been any narrowing of the differences in health outcomes between ethnic and religious minorities and the general population.
Inequality In Access To Health Services The accepted conventional wisdom has been that health services in Nepal are highly inequitable. This is true if one looks at total health sector expenditure, which is dominated by private out of pocket spending and which, inevitably, reflects the greater spending power of the better off. However, several influential reports have argued that public expenditure on the health sector is also highly unequal. That view needs to be significantly revised, to take account of the significant advances of the last decade.
An Equitap study published in May 2005 placed Nepal as having the ‘strongest pro-rich bias in health expenditure in the region’, based on a study of 15 countries in Asia28. This paper was quoted in the World Bank poverty assessment29, and the thinking behind it seems to have been influential in the attitudes of NHSP development partners. However, the conclusion is based on data for Nepal from the mid 1990s, before the major expansion in public health programmes, and is largely based on analysis of curative care, which has admittedly been inequitable due to low utilisation by the poor and high charges. However, as a depiction of the equity with which limited public expenditure on health services is allocated, it is grossly unfair. Nepal has spent two thirds or more of the health budget on successfully reducing mortality from easily preventable causes. The poorest were previously most prone to die from such causes, and it therefore seems highly likely that the impact has been pro-poor.
The report ‘Unequal Citizens’ has also been influential on external development partner thinking. It argues that ‘cultural religious and social values beliefs and behaviors are shaped by interlocking gender, ethnic and caste based hierarchies’, resulting in low access to health care and poor quality of health care for some excluded groups. For example, the low status, poor education, and high poverty levels of Dalit and Janajati groups are argued to result in low access, compounded in those areas where it is associated with remote locations. Women in all groups are further disadvantaged by low status in relation to men. In addition to other causes of low access, disrespectful attitudes
27 Unequal Citizens, p73 28 Equitapproject, Working Paper #3, Who benefits from public spending on health care in Asia? 29 World Bank, 2006, Nepal, Resilience Amidst Conflict, An Assessment of Poverty in Nepal, 1995-96 and 2003-04, Report 34834-NP, June 2006
41 of service providers towards Dalit and janajati groups are said to be a major barrier to seeking health care.
Some aspects of this picture may need to be qualified, and all of them should be re- considered in the light of the NDHS data on ethnicity and other minority groups when it is analysed. The 2004 living standards survey showed no statistically significant difference between male and female in the distribution of health consultations by practitioner type:- for both sexes, 26% consulted a Doctor, while 36.9% of men consulted a paramedic compared to 35.5% of women. The 2006 drug availability survey reported that facilities in all ecological regions see more female than male patients. The 2006 NDHS analysis of women’s health seeking behavior revealed that the top problems in accessing healthcare, reported by over half of the women interviewed, were concerns that no health care provider and no drugs would be available; not wanting to go alone, and concern that there would be no female care provider. For the poorest women, these reasons are also among the most important constraints, but are reported by more women (over 60% in each case), with more than 60% of women also reporting distance and the need to take transport as serious problems in accessing health care. Getting permission to go for treatment is not an important constraint for any group (consistently less than 10% for nearly all groups), even though NDHS also reports that decisions on their own health care were mainly taken by husband or someone else (presumably, other family members for non-married women) in more than half of cases. Problems in getting money for treatment are reported by 39% of all women, but 50% of poor women. This presumably mainly reflects poverty. It is possible that women have less control over household financial resources, though the NDHS reports most major household financial decisions being taken jointly, with only a small difference between men and women in the proportion of major purchase decisions taken mainly by the husband (20%) or mainly by the wife (15%). Women are reported to be more than twice as likely to take decisions on purchases of daily household needs. There are still gender biases in health-care seeking behavior for children, with NDHS 2006 reporting boys more likely than girls to be taken to a health care provider when suffering fever, and more likely to receive anti-biotics for ARI, though these differences are not reflected in mortality outcomes.
The most significant policy finding on health-seeking behavior from the NDHS survey is probably that abolishing user charges alone may not have a significant impact unless accompanied by other measures to ensure that service providers and drugs are available.
The NDHS2006 and NLSS2004 surveys show clear gaps by wealth quintile for a number of EHCS services. These include: - Family planning. The poor use family planning, but have a large gap between ideal family size and current fertility, while the better off have no such gap. - Safe motherhood. Both antenatal and delivery care show large disparities by wealth quintile. Antenatal care from any provider was 50% for the lowest quintile, 77% for the middle and 92% for the highest. Use of a health worker birth attendant was 8% for the poorest, 16% for the middle and 62% for the highest quintile. Disparities are worse for services by skilled birth attendants.
42 - EPI. The coverage of “all basic vaccines” is only 68% for the lowest quintile, vs. 87% for the middle and 93% for the highest. - Outpatient care. The NLSS 2004 survey (table 6.2A, 6.3), shows that for acute illnesses in the month prior to survey 43% of the poorest consumption quintile did not see any provider, vs 34% of the middle quintile and 27% of the richest quintile. This was in spite of the fact that 15% of the richest quintile reported an acute illness vs. only 10% of the poorest (i.e. presumably the richest reported more minor illnesses).
Other dimensions of inequality of access are related to educational level and location, with greater use of health services by the better educated, by the urban population, and by those living in the hills and in the Eastern and Central region as opposed to the relatively deprived mid and far West. Differences by ethnicity and religion have yet to be analyzed. A recent USAID survey on religious and ethnic differences with respect to maternal care services suggests that they remain significant (Table 5.3).
Table 5.3 Ethnic and religious Differences in Safe Motherhood Care Coverage, who uses Who does not benefit, and why? Inclusion policy and strategy Further action the service? needed? Ethnicity and ANC Muslims are less likely to receive Universal accessibility of service Inclusive policy in pregnancy check ups while Brahmins are Local language IEC and BCC training and more likely to get the services. Dalits and program recruitment of health Muslims are significantly less likely to use Dalit and Muslim focused worker and iron folic and vitamin A capsules. Empowerment program community volunteers Place of Delivery Overall, 84% had delivered their last child Need increase coverage for all Improvements to services at home, 15% had delivered their child at communities. Maternity incentive management of MIS. the health facility scheme to overcome cost barriers. IEC/BCC program. (11.0%), private clinic/nursing home (1.7%) Implementation Action Plan for the Quality of care and rural based health facilities like vulnerable communities HP/SHP or PHCC (1.5%). Brahmin or development plan. Chhetri castes are significantly more likely to deliver their child at a health facility. Dalits or Muslims are significantly less likely to deliver their babies at a health facility. Source: Mid Term Survey of Nepal Family Health program supported by USAID, 2005 (Based on a sample survey, 17 districts, all regions: Total respondents: 2144)
Existing MOHP Strategies To Tackle Inequality In terms of how public sector health expenditure has been allocated, the major approach to addressing inequality has been to move towards universal free access to a limited range of highly cost-effective public health interventions. As public health programs reach very high rates of coverage, inequities decline. The Vitamin A program has very high coverage and is equal across wealth quintiles. If Antenatal care or EPI reach nearly everyone, they will also become more equitable. As coverage increases, DOHS has begun to introduce micro planning, mapping pockets of non-coverage and planning how best to reach them. This has been used in low-performing EPI districts, and appears to
43 significantly raise coverage. A similar approach is being taken by family health division to address low contraceptive prevalence. Health Facility Management Committees may be a good place to discuss within VDC targeting since their interests are broad coverage, while the health staff would like to reduce their travel time if possible. In addition to geographical targeting, some minority groups may require external support to mobilize them to exercise their rights to basic health services, ensuring that Dalits and marginalised groups are represented on facility management committees as the law requires, encouraging them to have the confidence to raise their concerns, and raising the awareness of health workers with respect to particular causes of non-coverage. Community based approaches using FCHVs can be better at reaching the marginalized if well designed (e.g. the CB-MNC programs in Banke and Morang show good coverage of all social groups). FCHVs may need support and guidance, however, to ensure that the marginalised are reached effectively. FCHVs are generally drawn from higher status households, and NDHS 2006 survey seems to show that they are more often consulted by middle wealth quintile households.
Difficult judgements need to be made regarding the phasing in of targeting as coverage expands. A trial that specifically targeted dalit and Muslim groups produced large increases in family planning new acceptors, but raised questions about cost-effectiveness and sequencing (Health Communication Program/Flexible Fund under NFHP). In family planning, there is existing unmet demand from the poorest wealth quintiles, and the director of the family health division argued to us that the most immediate task is to ensure that those demands are met. As coverage expands from the current 44%, it will become increasingly important to focus on generating increased demand by those groups where acceptance of family planning is at present quite low. Too early a focus on targeting may result in expensively raising utilisation among hard to reach groups, while failing to meet needs that already exist and could have been met relatively inexpensively. DOHS are well aware of the dilemma, and have made reasoned judgements regarding the point at which general measures to expand coverage need to move towards targeted interventions to reach the groups that have been missed.
Geographical targeting has been a somewhat neglected approach. Although work has been undertaken on a need-based formula for allocating resources30., this has not been adopted, and would have political implications given the likely federal structure of the future state. The allocation of budget is at present based on norms related to the location of facilities, and on an incremental rather than needs-based approach to the annual budget. The regional medical stores for example allocate the same volume of drugs to every health facility of a given type, irrespective of the level of demand31.
Although the allocation may not be efficient, it does appear to favour the poorest areas. In Nepal, the poorest wealth quintiles are disproportionately found in remote hill districts, with the Mid-West and Far West hills and mountains having over 50% of their population
30 MOHP, Health Sector Reform Unit, Draft: Equity Analysis in Resource Allocation to Districts, (A review of the existing resource allocation pattern and development of formula for resource allocation to districts) , 2007
31 MOHP, drug availability survey, 2006
44 in the lowest wealth quintile. These areas receive priority in the per capita allocation of public expenditure on health. The poorest regions of the West (Nrs166) and Far West (NRs145) have the highest per capita public spending on health; while the wealthy Central region that includes Kathmandu and has most of the tertiary facilities nevertheless has the lowest per capita public health spend (NRs120)32. There are some inequalities within regions, especially between mountain districts, with some low HDI districts also having low health expenditure. Expenditure is higher in the mountains (261NRs per head) and hills (NRs156) than in the Terai (NRs100). The disproportionately high per capita spending in the mountains reflects the fact that populations of some mountain districts are not only poor, but are also remote and hard to reach, and health services established to meet their needs suffer relatively low utilisation due to low population density. Solutions that can be applied in densely populated districts and that may reach large populations of poor people relatively cost-effectively will not work in mountain and some hill districts.
Unfortunately, the relatively pro-poor allocation of budget is not reflected in the availability of staff. The concentration of 70% of Doctors in the Central region mainly reflects the dominance of the Kathmandu valley as the location for private sector services and national hospitals, but Table 5.4 suggests that Government allocation of resources has not been successful in offsetting this bias, with the two Western regions having disproportionately fewer staff relative to population in all categories.
Table 5.4 Unequal Distribution of Health Personnel Region Percentage Shares of:- Population Doctors Nurses and ANMs Retail Pharmacies Eastern 23 14 23 17 Central 35 70 40 64 Western 20 11 26 13 Mid Western 12 3 8 4 Far Western 10 2 3 3 All 100 100 100 100 Source: Ministry of Health (2005) (www.moh.gov.np
As we have seen, addressing unequal access is especially difficult with respect to curative services, but curative care will become increasingly important as preventive approaches reach universality and just require maintenance. Extending basic curative care and maternity services are key priorities for future expansion, but their success requires the multiple constraints on the supply and utilisation of these services to be tackled. This involves addressing the multiple problems involved in providing physical and financial access to facilities that are suitably equipped and stocked with drugs, with sufficiently trained and motivated staff able and willing to provide services when needed.
32 MOHP, Health Sector Reform Unit, Draft: Equity Analysis in Resource Allocation to Districts, (A review of the existing resource allocation pattern and development of formula for resource allocation to districts) , 2007
45 Outpatient service utilization is currently very low (0.38 visits per capita) and stagnating, and there is unused capacity in the system to cope with higher demand in most if not all areas of the country. The poor are more likely to go to SHP/HP (46% of visits) than middle (31%) or the wealthiest (14%) so improvements to those facilities help the poor more (NLSS2004 Tbl 6.5). User charges can be a barrier for the poor for some EHCS services (e.g. outpatient care and deliveries) so removal or reduction of user fees, whether universal or targeted for the poor, may increase their utilization. Reducing charges may be a necessary, but not sufficient, measure for increasing utilisation, since it will need to be accompanied by effective action on the other constraints regarding staffing and access to drugs.
The Maternity Incentive Scheme offers incentives to women delivering in public health facilities in all 75 districts (NPR. 500 for Terai, 1,000 for Hills and 1500 for Mountain), with free delivery care in 25 low human development index districts. Although it was initially planned as a payment for transport cost, in practice it provides incentive to the mother who delivers at health facilities (focus on care seeking practices). The scheme also offers an incentive of NPR 300 for the trained health worker who conducts deliveries in homes or facilities in all districts and in the 25 low-HDI districts only the scheme also reimburses the health facility NPR 1000 for each delivery. An assessment of the management of the scheme was undertaken in Spring/Summar 2007, and an impact evaluation is underway. Data for 10 districts that was collected for the management study reveals some problems in ensuring that timely support reaches those eligible to receive it:-a) only 38% of women who delivered at a public facility received the incentive, b) 99% of health workers assisting in home deliveries received incentive, c) 53% of health institutional delivery health workers received incentive, and d) 92% of deliveries in HDI district facilities were provided free but facilities received reimbursement for only 28% of these deliveries.
Government has recently announced that basic services at health post and sub health post level will be entirely free to all users. The implications are discussed in the next section.
Overall monitoring of equity issues remains weak. A gender focal point has been established but is not active. Individual divisions may monitor coverage and access issues within their area of work, but there is no overall unit monitoring access and equity issues. Part of the problem is that the HMIS does not collect data by minority religious, caste or ethnic groups; although a pilot of disaggregated health data is being undertaken in three districts for possible adoption within HMIS.
Recommendations on Reducing Inequality MOHP is doing many of the right things to address inequality issues, and part of what needs to be done is to communicate that vision more effectively, particularly to the politicians and the EDPs. Further progress on issues such as geographical resource allocation needs to be advanced as and when the political process permits.
46 A major weakness is the lack of disaggregated data to monitor issues of inequality of access: - the results of the pilot of a more disaggregated HMIS need to be reviewed quickly, necessary modifications agreed, and training and support provided to enable all districts to begin collecting disaggregated data.
The extent to which particular caste, ethnic or religious groups are disadvantaged in access to health services will become clearer when the NDHS data on this is analysed. The implications of this analysis should be discussed during the MTR.
If, as expected, the analysis reveals that significant differences in health outcomes and health service access persist and can not be entirely explained by poverty, it is suggested that the Secretary (or even the Minister) should consider issuing guidance that:-
i. Findings on inclusion issues from the NDHS should be taken into account when drawing up work plans and budgets for 2008/09. Work plans should contain specific proposals for how issues of inequality emerging from the DHS will be addressed; ii. The inclusion content of draft AWPBs will be reviewed at division head level and in an AWPB working group to be convened by the secretary to discuss draft AWPB submissions.
It is also recommended that issues of inclusion should be a theme of the 2007/8 regional and national reviews, drawing on the NDHS, on disaggregated data from those districts that have started to collect it, and on such other data as may be locally available. Divisions, regions and districts should come to the review ready to discuss problems of inequality of access within their areas of responsibility, the effectiveness of existing approaches to tackling it, and their suggestions as to what more if anything needs to be done. This analysis will feed in to the preparation process for the design of NHSP 2.
It is recommended that the next NHSP should make more explicit reference to the objective of achieving more equal access to health services by all caste, ethnic, religious and other groupings in Nepali society. The current wording at goal level refers only to the poor and those living in remote areas, while the purpose level statement talks about equitable access and gender sensitivity, but makes no reference to forms of inequality.
The NHSP2 design process should give explicit attention to how best to mainstream inclusion issues, including the implications for institutional arrangements.
5.3 Health Sector Financing and Financial management
The Role of User Charges Annex 5 discusses the impact of the Government policy of extending free basic services to all.
47 Most EHCS services are already free to the user or nearly free from public sources. This includes the major prevention programmes (child immunisation, Vitamin A and de- worming), most family planning services, most ante-natal care, household spraying and treatment for kala-azar and malaria, treatment for TB and leprosy, and some sick child services (especially for diarrhea and pneumonia and especially if provided by community health workers).
Outside these categories, most patients have been required to pay. Costs are usually prominently displayed at the facility, to ensure transparency. Outpatients will pay a registration fee, and will be asked to pay for tests, drugs, and treatment. Inpatients are required to pay variable costs of the hospital. EHCS Services that are likely to be charged are: a. Most treatment of acute illness. In fact, the NLSS 2004 survey found that reported average payments for acute illness treatment were nearly the same in the private and the public sectors. (table 6.7) b. Most delivery costs. Studies have found substantial average costs for deliveries by the public sector, with especially high costs if emergency transport is used or if emergency obstetric care is needed. c. In the case of drugs, practice is variable. Where there is a Community Drug Program operating, as is the case in most but not all districts, drugs are likely to be charged for, with the proceeds used to purchase additional supplies. The CDPs appear to be effective in ensuring a steady supply of essential drugs, but have a mixed picture in terms of holding down prices and exempting the poor (some schemes have worked well and some have not). d. Where the CDP is not operating, drugs supplied by the Government may be given free, but the patient may need to buy items that are not in stock from a private pharmacy.
The Ministry of Health and Population (MOHP) intends to move to universal free essential health care (EHC). However, the pathway to this end is not yet defined. In July 2007, the Cabinet pronounced free inpatient, emergency and outpatient care in the 25 lowest HDI district hospitals. In other districts, the poor and vulnerable are supposed to receive free emergency treatment and in-patient care. In October 2007, the Cabinet pronounced free care for sub health posts and health posts: in effect outpatient care at this level, given that all else is free anyway. Presently the MOHP are considering the exemption of maternity care.
The GON's rationale is based on "the new dispensation” (i.e., the Interim Government’s interim constitution) which states that “basic” health care for all is a fundamental right. Basic is not defined. This has been interpreted to mean free care.
Government has made budget provision of roughly NRs 225mn for the policy in 2007/8. This would have been sufficient before the October 2007 announcement, but needs to be re-examined in the light of the decision to abolish all charges at health post and sub health post level. If the policy is to have the intended impact in reducing barriers to access, sufficient provision needs to be made for providing free drugs for both existing patients and the new patients attracted by the removal of charges (see Annex 5).
48
RTI estimate the cost of free basic services to all up to and including treatment in hospitals of 25 beds or less would be less than $1 per head. The budget cost of compensating facilities for lost revenue from user fees is only a small part of the total. The major costs are the result of Government taking responsibility for free provision of drugs and other items that patients were previously obliged to buy from the private sector. In addition to meeting these costs for existing patients, Government needs to make provision for financing the needs of additional patients attracted by free services. RTI acknowledge that the estimate is subject to a wide margin of uncertainty due to the unknown impact on demand, and necessary approximations of the cost of additional services. Taken at face value, the cost would be equal to 11% of the 2007/8 health budget, but 22% of GON financed budget expenditure on health. As a share of total 2007/8 budgeted public expenditure on all sectors, it is 0.8% of the total Red Book budget, and 1% of the total GON financed budget. This is a substantial cost, but could perhaps be phased in over two to three years as the growth in revenues permits.
Community Drug Programme The introduction of free services will have implications for the community drug programme. The community drug programmes enable facilities at district level to charge for drugs and medical supplies, using the revenue thus generated to purchase additional drugs, either drugs that are not included in the essential drugs list, or additional supplies of items that are found to be in short supply. The CDPs will lose all of the income from registration fees and other charges, 46% of the total in 2005/6, plus the majority of the income from medicine sales, which accounted for the balance. There will be a residual role for the CDPs in purchasing and selling items not included within the approved drugs list, but the implication is that they will be significantly scaled back. If all essential drugs are provided free, the continuing need for CDPs that are limited to the supply of non- essential items could perhaps be questioned. However, there may be a case for keeping the CDPs in existence for precautionary reasons, at least until Government has established a sound track-record in reliably supplying key commodities and essential drugs. If the CDPs are felt to be valuable because of their other roles, which include encouraging rational prescribing practice and ensuring reliable access to drugs, one possible institutional arrangement that might be worth exploring would be for MOHP to pay CDPs for the cost of drugs supplied free. We are not advocating this model, which would carry risks of being overly bureaucratic and resulting in payment delays and drug shortages. However, if a simple methodology could be developed that does not require multiple form filling and negotiation of long financing delays, it would be one possible route by which flexible funding might be made available in a way that reflects need.
A second implication for the CDPs is that more districts will find that bank balances accumulated in the past will not be fully required for future drug purchases. This is already the case in Kaski and several other districts that have accumulated surpluses that are considerably larger than requirements for future drug purchases, even under the existing charging regime. These balances can be used for other purposes, including recruiting additional staff or financing improvements to facilities. The usual risk aversion of staff worried about taking actions that could be criticized might have prevented the
49 funds being used in this way in some cases. There may be a need to provide guidance and support to staff and CDP management committees on how to make best use of these funds.
Community Health Insurance There has been no further progress on extending community health insurance beyond the existing small-scale pilots. The extension of free basic health services to all, up to and including treatment in district hospitals, would render community health insurance largely redundant, since most of the risks it is designed to cover would be financed directly by the state. There is a small residual gap in the safety net against risk, in so far as patients requiring referral beyond district hospital level will not have their costs covered. This rare but expensive risk can not be covered by insurance in isolation at any level of premium that would be affordable for all but the very rich. As and when Government wishes and can afford to further extend the safety net, it could begin to cover some costs of referrals to higher level institutions. This should probably not be a priority in the short term, as there are other ways to use the available health budget that would have a bigger impact on mortality and morbidity for the same cost.
Budget Management The importance of leadership can be illustrated by the long standing and Nepal wide problem of low utilisation of the approved budget. Delays occur at numerous levels, and partly reflect problems caused by an overly bureaucratic Government system of budget management, together with the reluctance of cautious civil servants to utilise the flexibility that exists. For example, up to one third of the previous year’s budget can be spent on P1 activities in advance of formal authorisation, but civil servants at all levels nevertheless tend to wait for the approval letter before starting activities. External development partners share significantly in the responsibility, as EDP funds consistently show the lowest percentage disbursement. This partly reflects late or incomplete approval of funds, and partly reflects problems in complying with the procedures of the donor, including submission of financial monitoring reports and obtaining timely ‘no objections’ to procurement proposals. Nevertheless, in 2006/7, the final figures are likely to confirm a second year of significant improvement in the rate of disbursement of the budget possibly to over 90% of the approved budget. Most interviewees ascribed the improvement to regular meetings held by the Minister and Secretary in order to check progress and ensure that necessary steps were not being delayed. Unfortunately, late finalisation of the 2007/8 budget is likely to mean that the improvement will not be sustained in the current year. This is mainly because determined MOHP advocacy for a bigger budget in 2007/8 resulted in late finalisation of budget ceilings, with knock-on effects to delay finalisation of the AWPB and subsequent authorisation stages. High level attention to budget monitoring needs to be continued, and might usefully be accompanied by a stronger role for the regional directorates in encouraging more pro-active management by the districts.
50 5.4 Management Reform To Support Better Health Outcomes
Performance Management From the viewpoint of improving health outcomes, the most important management reform agenda concerns how best to address the difficult problem of improving staff performance.
The increase in demand following abolition of charges for basic services is likely to vary substantially between districts and between institutions. Although it is cost that is the major constraint to utilization in some areas, in others it may be the absence of staff or the difficulty of travel that is more important. Staff motivation may itself be damaged by the policy, since free services will reduce the income of the private pharmacies that are operated by many health staff, while increased demand will oblige them to work longer hours. If the policy is not to be discredited, MOHP needs to find a way to motivate the staff to provide better services, while also responding flexibly to supply the varying increase in the quantity of drugs and consumables that different districts and facilities require in order to meet the increased demand. To ensure that the policy narrows inequality as intended, it will also be important to study those districts where demand remains low, in order to identify and act on the other constraints that inhibit patient demand, for example by improving staff availability and training, or finding ways to bring services closer to those who should be using them.
The extra demand will only be sustained if staff behaviour changes in order to ensure that facilities are open, staffed, and stocked with drugs at the times and in the locations where people need them. A number of alternative approaches could be taken to address the need for improved staff performance and flexible budgets that reflect the pattern of demand. Approaches that have been tried in a number of developed and developing countries involve negotiating targets for managers and staff, and providing incentives for reaching or exceeding them. Simple tables of comparative performance can be effective in encouraging competition with peers that can raise performance even without financial inducement. The incentives can be individual or collective, can be in the form of extra budget resources for delivering services or extra compensation for staff, and can be in financial form or in less tangible forms of recognition via favourable performance assessments linked to promotion or prizes. The precise approach matters less than recognition that performance needs to be addressed, and that the approach to budget allocation needs to become flexible enough to respond to new patterns of utilisation, patterns that the introduction of free services could change quite quickly towards a distribution of demand that differs substantially from the current allocation of the budget.
A 3-district pilot scheme for introducing performance incentives had started in 2006/7 but was interrupted when the budget was not released. However, a detailed model has been developed and could be adapted. There may also be lessons to be learned from other sectors and from the design of incentives under the local government development programme.
51 It is recommended that the development of a system of performance management linked to budget provision should be part of the design process for the next NHSP. Developing such an approach will only work if MOHP management support it, MOF and NPC are willing to approve the necessary budget, and DOHS and district staff understand and accept that the approach is fair and reasonable. It needs to be developed in a participatory manner, and steered by MOHP. External pressure from EDPs to meet time-bound objectives enshrined in logframes is in this case likely to prove unhelpful to the objective of putting in place an approach that is generally accepted within MOHP.
Management Reform and the NHSP Log-Frame Management reform in terms of the NHSP logframe indicators is perceived to have been sluggish, with the outputs envisaged in the NHSP mostly unachieved. This partly reflects the difficulty of making progress in a period of political turmoil, but there has also been a problem of lack of capacity, with the Health Sector Reform Unit virtually consisting of one person, and headed at too junior a level to be fully effective as the driver of the reform process. Recent changes should improve matters, with the appointment of a new head at Joint Secretary level, an additional staff member added, and technical assistance from RTI co-located in the MOHP building. Nevertheless, serious problems remain. The technical assistance studies that are intended to identify necessary organisational changes to MOHP have been fragmented (three reports by different consultants on MOHP organisational change, a further three by different consultants on human resources). Making sense of overlapping and potentially conflicting recommendations, and turning them into a feasible action plan with clear responsibilities, will be a difficult task. It will require strong and determined leadership from the top of the Ministry, something that has perhaps not been consistently in evidence in the first three years of NHSP.
5.5 Human Resources Management MOHP policy is to upgrade the skills of lower level staff, replacing the Village Health Worker cadre with AHWs, and upgrading MCHWs to ANMs in order to increase the numbers of skilled birth attendants. The main concern with this approach is that the two cadres that are being phased out are the locally resident and therefore accessible and accountable staff that have, together with the unpaid FCHVs, been mostly responsible for successful implementation of public health programmes. VHWs provide nearly all the childhood immunizations in Nepal and are usually the supervisors for FCHVs. Both VHWs and MCHWs are active in providing family planning supplies and are considered with FCHVs as “community health workers” in CB-IMCI. The AHWs and ANMs that would replace them may be better qualified, but are less often from the community, more often commuting to work, and are less willing to do tasks such as EPI or FCHV supervision which they may consider below their level. Although some of the upgrading may take place by accredited training of VHW and MCHWs, many of the present incumbents have not completed their education to SLC level, the minimum educational qualification required by PSC to upgrade them. It is also likely that present incumbents may be reluctant to embark on demanding training if the final result is to stay doing essentially the same job, albeit at higher pay.The impact on coverage of public health programmes needs to be monitored as the upgrading progresses, and the policy re- considered if there is evidence of a weakening of the public health interventions.
52 Another major HR issue is frequent staff transfers imposed for reasons of patronage without respecting civil service rules on minimum length of posting. This disrupts health service functioning, especially when applied to management positions, and needs to be resisted. Greater transparency, monitoring of numbers, and a greater willingness to draw public attention to cases, might have some impact on discouraging frivolous moves.
It is acknowledged that most program areas plan their own training without regard to other programs, so that there is sometimes overlap in training content and training for some government staff may be excessive (keeping them away from patient services or routine work). We considered possible approaches to reducing this, such as preparing and annually agreeing a comprehensive training plan, but fear that the bureaucratic effort required would be disproportionate to the benefits. It would require considerable effort on the part of the government and EDP projects for all programs to share and coordinate training plans, and even more effort to change plans so as to avoid these problems. It is recommended that DOHS directors should meet to discuss the issue, together with the national health training centre, and try to reach agreement on a simpler approach to information exchange that would provide opportunities for better coordination and possibly for some more consolidation of training programmes to serve the needs of more than one division.
5.6 Managing the SWAP
Integrating the JAR within the MOHP Review At present, the JAR is a separate exercise from the MOHP internal review. The two should be combined. The November/December review should continue to focus on performance in the previous year, but that review of performance should trigger EDP decisions on their future level of support.
There is a strong case for starting the AWPB process in January, in order to involve the districts, as was done with a limited number of so called devolved districts in 2007/8, and to give time for more meaningful engagement by EDPs. The EDP involvement in the annual work plan and budget happens to a limited extent at division level, but the more formal June/July JAR discussion happens too late in the process to have any influence on it. Involving the DPs (who are expected to provide half of the budget) more formally in the AWPB could be helpful in working jointly to:- identify programme areas for expansion and other spending pressures that need to be accommodated; identify expected resources from all sources Prioritise available funds to ensure that the most important programmes are fully funded.
If there is greater involvement and transparency between partners during the planning and budgeting process, then the June/July JAR could become an opportunity to confirm and adjust resource assumptions and priorities that have already been extensively discussed. Ideally, greater involvement in the process will build mutual trust in an
53 AWPB with overall priorities that all partners understand and own, even if differences of detail remain.
Longer Term, Predictable Finance Nepal is one of the first eight countries to sign up to the International Health Partnership, the ‘compact’ for which was signed in London in September 2007. The ‘compact’ commits external development partners to provide longer-term financial support, and to be accountable for actually delivering the financial and technical support that they commit, reporting annually on their performance. These two undertakings are extremely important for the sustainability of public health services. The wording in the compact is much stronger than in the ‘code of conduct’ recently agreed by the development partners supporting NHSP. The code of conduct only commits EDPs to ‘provide relevant budget estimation information’ to GON by March 15th. There is no commitment to actually provide aid at indicated levels, and the whole draft is so full of caveats that it commits EDPs to nothing other than a set of principles they agree to ‘work towards’ at some unspecified future date and only ‘to the extent possible’. It is of little help to MOHP or MOF in predicting what support might be received. We recommend that:-
1. Wherever possible, EDP commitments or at least indications should be multi- year. Alterations to announced figures should be minimised. 2. The date by which EDP estimates of their spending for the following year should be provided to MOHP should be advanced to January 15th, to give more time for a more participatory AWPB process. 3. If EDPs have to adjust their spending, or feel compelled to do so because of concerns about performance, the sanctions should apply only from the next budget year, not the current one, and MOHP should be given clear guidance on whether previously indicated figures can be restored, and what actions are needed to secure this. 4. All formalities for donor support should whenever possible be completed before the July start to the financial year in which it is to be provided, to ensure that late approval by EDPs does not become a cause of disruption in the NHSP programmes.
These changes will be easier for some donors than for others, but it is important that all go as far as their procedures will permit. The EDPs finance more than half of the health budget. They are therefore co-responsible for what happens in the sector. Although EDPs have been frustrated by some aspects of MOHP performance, the Ministry has done more than enough in reducing mortality to merit predictable funding from the donors. Delayed or reduced EDP disbursements have real consequences for health outcomes.
Reforming Pool Funding (and attracting more donors) In an effort to increase budget certainty, there is a strong case for moving the pooled fund towards a fixed cash commitment rather than a percentage of the actual MOHP spending. The intention of the current approach of reimbursing a percentage of actual spending is to provide an incentive for improved budget execution. The result, however, is that DFID, which manages itself on a cash rather than a commitment basis, faces unnecessary
54 difficulty in managing its budget, and the Nepal program and the MOHP loses money that is not spent within the financial year. It is in our view unlikely that the approach has the intended positive impact on MOHP incentives to spend. It makes no difference to MOHP how much the pool fund donors disburse, since their spending ceiling is determined by the approved budget and the spending authorisations given by MOF. The main impact of the current approach is likely to be a negative effect on the size of the health budget, since MOF/NPC know that they can not rely on receiving the full value of the pooled fund if MOHP does not disburse the required amount, a factor that is likely to encourage them to discount the pool donor commitments when deciding how much budget they can afford to allocate to MOHP. The percentage share approach also makes it more complicated than it needs to be to incorporate other donors in the pool. A simple cash commitment would be more in line with the spirit of the IHP ‘compact’, would encourage more donors who work to a cash budget to participate in the pool, and could more easily accommodate the needs of donors who may wish to harmonise but who can not avoid some nominal earmarking of their support.
A related simplification that could have a positive impact on disbursement would be to de-link pooled fund disbursements from the need for quarterly financial monitoring reports. The intended approach at present is that the pooled fund works on an ‘advance and replenish’ system, with quarterly financial monitoring reports triggering requests to replenish the pool, exactly as if the MOHP budget were a large World Bank project. To some extent, the link has already broken down because of the inability of MOHP to provide the reports on time. If the system were working properly, the percentage disbursement of pool fund commitments should be exactly the same as for the GON financed budget, but in fact they have fallen far short, indicating problems in meeting the requirements. The simpler alternative of fixed cash commitments would break the direct in-year link between pool fund disbursements and budget implementation. Donors would commit their funds in advance, and disburse them at agreed intervals in the financial year. MOHP would draw on them as required, without requiring FMRs to support requests to replenish the pool. Pool donors would still ask for quarterly and annual monitoring reports on budget execution, which would be the same reports as are required by MOF/NPC, and would show sources and expenditures reconciled to bank accounts, including the pool fund. Donor disbursements could be front-end loaded, enabling MOHP to start activities earlier, or the timing could be adjusted to make best use of flexibility due to differences in GON and EDP financial years. This does not imply any meaningful loss of financial accountability. By shifting the focus away from generating specific reports for pool donors it should release capacity for ensuring that MOHP complies with GON financial regulations. Annual commitments can if desired be adjusted if progress on financial management is not maintained, but funds committed for a particular budget year would be fully disbursed within that year.
55 6. Recommendations
6.1 Changes to the NHSP Log Frame 1. Consider modifications to the log-frame and indicators as proposed in Annex 3 and Annex 4, including:- a. Drop the target on health share in the national budget b. Drop target on handing over health facilities pending establishment of elected local bodies c. Drop targets that are inconsistent with the new policy on free basic services for all, including those related to community health insurance and local resource mobilisation. d. Drop outputs targeting specific institutional forms such as handing over a specified number of hospitals to private or NGO management e. Modify EHCS indicators as proposed, to ensure that they are measurable and meaningful.
6.2 Future priorities for EHCS 2. Maintain and scale up successful public health interventions listed in 5.1
3. Prioritise maternal and newborn care, which will require high level institution based care , supported by expanding successful piloting of community based approaches
4. Monitor UNICEF supported malnutrition pilot, consider scaling up if successful
5. Review the causes of 16% higher death rates among adult males, and whether specific action is feasible and merited to reduce the gap
6. Undertake a more detailed cost estimate for extending free services, to inform phasing and design of the policy
6.3 Inequality of Access 7. Further progress on issues such as geographical resource allocation needs to be advanced as and when the political process permits.
8. The results of the pilot of a more disaggregated HMIS need to be reviewed quickly, necessary modifications agreed, and training and support provided to enable all districts to begin collecting disaggregated data.
9. The implications of forthcoming NDHS analysis of the extent to which particular caste, ethnic or religious groups are disadvantaged in access to health services should be discussed during the MTR.
56 10. If, as expected, the NDHS shows that significant differences in health outcomes and health service access persist and can not be entirely explained by poverty, it is suggested that:- a. The Secretary issue guidance that findings on inclusion issues from the NDHS should be taken into account by those responsible for drawing up work plans and budgets for 2008/09. Work plans should contain specific proposals for how issues of inequality emerging from the DHS will be addressed; b. The Secretary should convene a working group to discuss draft contributions to the MOHP AWPB. Inter alia, this working group should review the treatment of inclusion issues in drafts prepared by the departments and divisions. c. Inclusion should be a theme of the 2007/8 regional and national reviews, drawing on the NDHS, on disaggregated data from those districts that have started to collect it, and on such other data as may be locally available. Divisions, regions and districts should come to the review ready to discuss problems of inequality of access within their areas of responsibility, the effectiveness of existing approaches to tackling it, and their suggestions as to what more if anything needs to be done. This analysis will feed in to the preparation process for the design of NHSP 2.
11. It is recommended that the next NHSP should make explicit reference to the objective of achieving equal access to basic health services irrespective of poverty, gender, caste, ethnic origin, or religious faith.
12. The NHSP2 design process should give explicit attention to how best to mainstream inclusion issues, including the implications for institutional arrangements.
6. 4 Management and Related Reforms 13. To ensure that free basic services have the intended positive effect on utilisation of basic health services of reasonable quality, ensure that the policy is accompanied by:-
a. Flexible allocation of additional budgets in response to the location of increased demand; b. Piloting and phasing in of measures to improve performance management, possibly including performance-based incentives for staff meeting or exceeding agreed targets; c. Monitoring of the causes of continuing low demand in areas not experiencing significant demand increase, linked to initiatives to identify and address the constraints.
14. Design performance management proposals through a participatory process steered by senior management, aimed at gaining wide acceptance within GON and MOHP; time-bound targets monitored by the EDPs may not be helpful and should be avoided.
57 15. Explore the scope for supporting isolated staff in district hospitals and PHCs by developing relationships with regional zonal and private hospitals
16. Consider funding tertiary hospitals exclusively by fixed block grant budgets, while leaving them freedom to mobilise their own revenues
17. Facilitate the further development of health insurance for modern sector employees
18. High level attention to budget monitoring needs to be continued, and might usefully be accompanied by a stronger role for the regional directorates in encouraging more pro-active management by the districts
19. Monitor the impact of upgrading VHW and MCHW on public health programmes, reconsider the policy if coverage drops
20. Monitor transfers outside the rules, use transparency to resist trivial moves
6. 5 Managing the Sector Wide Approach 21. Combine the end year JAR with annual MOHP review
22. EDPs should where feasible:-
d. Provide multi-year commitments, as implied by the IHP ‘compact.’ e. Indicate funding for the following FY by January 15th, completing necessary financing agreements and other formalities to permit disbursement to commence at the start of the budget year. f. Avoid changes to committed funding levels where possible, and ensure that any alterations that do become necessary are applied to the following year to avoid disrupting implementation of the current AWPB; g. All formalities should whenever possible be completed before the financial year in which funds are to be disbursed, to ensure that late approval by EDPs does not become a cause of disruption in the NHSP programmes. 23. Shift poled funding to fixed cash commitments, based on a budget support modality, dropping the linking of replenishment to FMRs
58 ANNEX 1 TERMS OF REFERENCE NEPAL HEALTH SECTOR PROGRAMME
MID- TERM REVIEW: TERMS OF REFERENCE
1. Background The NHSP –IP is now into its third year (of a five year period). It is the first health sector wide programme in Nepal and incorporates all existing public health programmes as well as a reform agenda to improve the sector’s performance in order that coverage and quality is improved nation wide.
The review takes places during a unique period in Nepal’s history. The interim Government is challenged to ensure ongoing peace and security as well as the delivery of elections for a constituent assembly. In parallel, the expectations of Nepali citizens for improved services have increased and the social sectors are required to deliver immediate gains. The National Planning Commission is in the process of developing a three year interim Plan which guides development planning.
The 2006 DHS results demonstrate remarkable improvements in health outcomes and health impact (except for malnutrition). All NHSP stakeholders are encouraged by this and eager to understand the relationship between NHSP and the results (so far as this is possible).
Whilst the programme is meeting its health outcomes against the Logframe, it is not meeting any of the reform milestones. Therefore, progress is despite, and not due to reform. This situation is emerging in Bangladesh.
Conducting the mid term review (MTR) is a requirement for the pooled donors: the World Bank and DFID. The Joint Financing Arrangement (JFA) signed between the Government of Nepal and Pooling Donors stipulates that the JFA Signatories will jointly conduct a MTR after two years of NHSP. Under the JFA, independent technical reviews were envisaged. Although some thematic ones have taken place, no independent review of the sector’s performance has taken place and hence an element of independent monitoring is required under the MTR.
Recently the World Bank commissioned public financial management and procurement report has been published which will assist the MOHP in advancing its financial management improvement plan. This report will form the heart of the forthcoming fiduciary risk assessment due in the summer.
A review needs to be commissioned. The results will form be used by the EDPs and the MOHP during the MTR event itself which will be the next Joint Annual Review (JAR) which will probably be held in November or December.
A small team is required with multi donor funding/engagement envisaged. These TORs relate to the core team to be led by a team leader.
2. Purpose
59 To lead, and provide the substantive analysis for NHSP MTR. The MTR will review NHSP progress against its own targets, assess its contribution to health gains in Nepal and make recommendations for the remainder of the NHSP lifetime.
The MTR review report will be central to the December Joint Annual Review (JAR). This biannual review, will be the MTR event.
3. Objectives
The lead consultant and his contracted team in consultation with one of more consultants to the MTR (funded by another source) will:
1. To review the overall progress of NHSP 2. To ascertain, to the extent possible, the relationship between NHSP and the DHS results and apply the implications of this analysis to (3) 3. To recommend changes in policy or strategy or implementation for the remainder of NHSP
Outputs A MTR report. Electronic copy of report shall be submitted by the end of October A dissemination event in country in October.
Tasks
Review progress against the programme’s performance framework: NHSP-IP Logframe NHSP- IP Reform milestones World Bank Project Appraisal Document
Review progress against performance reports to date Annual Health Management Information System Annual Reports Financial Monitoring Reports (FMRs) Bi annual Joint Annual review Aide Memoirs Independent review of NHSP – September 2006 (Foster/Regmi) Financial Management and Procurement report (Upadya commissioned by the World Bank 2007)
Review independent assessments of public health functioning and Nepal’s health status Review UNOCHR reports on service functioning (largely from NGO sources) Review health service functioning from documentation from EDPs over the last year DHS 2006 Poverty Reduction – NLSS 1993/4 and NLSS 2003/04 - 2006
In reviewing NHSP progress the following will be assessed
Relevance:
60 How relevant is the NHSP-IP document, including the outputs, implementation strategies, modalities and activities in the current situation? Can NHSP respond to the changed situation in Nepal? There are major tensions existing now as the MOHP expect the MOHP to produce some “early wins”. To what extent is this possible? Can this expectation advance reform – or undermine reform? What implementation challenges did the conflict produce and are these now abating? Are there new implementation challenges? Is NHSP sufficiently pro poor or pro addressing excluded groups?
Effectiveness and efficiency To what extent is the achievement to the NHSP Logframe and DHS results are a result of the NHSP Within that, to what extent are the results due to “business as usual” – i.e. some semi vertical donor supported programmes that have delivered very well? Has the reform agenda provided any value added? Has the new ways of working between EDPs and the MOHP, MOF, OAG provided any “value added” to the status of health care? If so, how and to what extent? To what extent has NHSP advanced donor harmonisation?
Sustainability Institutional and financial sustainability of the strategies and implementation modalities
The review will be in two Parts
Part 1 Assimilate all available documentation from the EDPs and other sources (e.g. OCHA www.un.org.np) to ascertain the degree of public sector delivery from non MOHP sources
The above needs to be conducted before the in country MT R process takes place
Part 2 Desk review of Part 1 under Tasks. Review the outcome of Part 1 Facilitate thematic focus group discussions based on actual findings and assumptions
It will not be necessary to review financial management or procurement as the 2007 World Bank commissioned ex post review and the forthcoming DFID commissioned sector fiduciary risk assessment will appraised progress in this area.
61 Annex 2 List of Contacts
List of individuals met by MTR team Persons Organization Mr. R. C. Bahadur Shingh, Secretary MOHP Dr. N. M. Shrestha, Chief Specialist MOHP Mr. Binod Gyawali, Jt Sect MOHP Mr. Kapil Ghimire, Chief Coordinator MOHP/HRSU Dr. Baburam Marashini HRSU/MOHP Ms. Susan Clapham, Senior Health Advisor DFID Mr. Purushottam Acharya, health Advisor DFID Mr. Roshan Bajracharya, Senior Economist WB Dr. N. Sharma, Health Advisor WB Dr. Sunder Gopalan, WB WB Dr. Govinda Ojha, DG DOHS DOHS Dr. B. K. Subedi, Director FHD DOHS Dr. Mingma Sherpa, Director LMD DOHS Dr. Y.B Pradhan, Child Health Dr. S. S. Tiwari, Director, Management DOHS Dr. Ann., Chief Health Division USAID Dr. Sheron USAID MR. Shushil Sharma-Chief FCGO Mr. Shiva Prasad Pandit Mr. Diwakar Rimal Mr. Yogendra Gauchen – Chief MOHP Mr. Loknath Gupta- (Account Officer) Ms. Indira Shrestha, NPC Member NPC Dr. Bina Pradhan- Advisor, Mr. Gyanendra Shrestha, Director Health Program Mr. Subash Gurung Mr. S. Pandey KFW Dr. Kan Tun, Representative WHO Dr. Birthe UNICEF Dr. Amit Bhandari GTZ-HSPP Mr. Sonathan Gishing GTZ-HSPP Mr. Shyam Sunder Sharma KFW Consultant Mr. Devi Prasai RTI Consultant Mr. Ajit Pradhan SSMP Dr. Mahesh Maskey, Coordinator, Policy Advisory MOHP Committee Dr. Bhola Rijal Private Health Institutions Dr. Lok Bikram Thapa Association
62 Dr. S. Bajaj Dr.
Mr. Asha Lal Tamang, BNMT Mr. Mr. Giridhari Pouel FPAN Ms. Maureen Dariang UMN Mr. Lok Raj SC Network Mr. Dandi Ram Biswakarma SDC Mr. Harka Thapa Ms. Genevie??? Dr. J. S. Kang, WB Teleconference Dr. Egnesh??? Teleconference
Date: 2063-6-14 Sisuwa PHC, Kaski S.N. Name Status 1. Mr. Laxmi Prasad Tripathi Gen. Member, Management Committee. 2. Mr. Somlal Kadel Gen. Member, Mgmt. 3. Mr. Harka Bahadur Shrestha Chair, Mgmt. 4. Ms. Kripa Paudel Gen. Member, Mgmt. 5. Ms. Mathura Subedi Gen. Member, Mgmt 6. Ms. Rewati Aryal Chair, Aama Samuha 7. Ms. Rishimaya Tripathi Member, Aama Samuha 8. Mr. Bishnu Paudel Member, Aama Samuha 9. Mr. Surya Banjara Vice Chair, Aama Samuha 10. Ms. Kharika Subedi Member, Aama Samuha 11. Ms. Tara Adhikari FCHV 12. Ms. Sarada Bastola Ma. Swa. Se 13. Ms. Indra Maya Bhujel Ma. Swa. Se 14. Ms. Uma Bastola Member, Aama Samuha 15. Ms. Kharika Subedi Member, Aama Samuha 16. Ms. Sita Devi Adhikari Ma. Swa. Se 17. Ms. Saraswoti Khanal Ma. Swa. Se 18. Ms. Jamuna Pangebi Ma. Swa. Se 19. Ms. Laxmi Tripatihi Ma. Swa. Se 20. Ms. Bishnu Maya Adhikari Ma. Swa. Se 21. Mr. Bishnu Jammarkettel Ma. Swa. Se 22. Ms. Ujeli Baral Member, Mothers Group 23. Ms. Chimkala Lamichane Member, Aama Samuha 24. Ms. Hem Kumari Gurung Ma. Swa. Se 25. Ms. Sarita Adhikari Ma. Swa. Se 26. Ms. Radhika Paudel Ma. Swa. Se 27. Ms. Radha Baral Ma. Swa. Se 28. Ms. Bodhraj Subedi Ja. Swa. Ni.
63 29. Mr. Rabindra Shrma Bastakoti Lab Assistance
Pokhara and Syngja S.N. Name Status 1 Dr. S. S. Mishra, Regional Director MOHP/RD Western Region 2 Dr. Narayan Ojha, SPHO DPHO, Kaski 3 Dr. S.P Kapoor, MS Manipal Teaching Hospital, Pokhara Dr. Dey, Chief Community Medicine Department Manipal Medical Collage Pokhara Dr. V. M. Alulkar, Dean Manipal Medical Collage Pokhara Dr. Somat Singh Tulachan, Chairperson Gandaki Regional Hospital Management Board Mr. Indra Mani Paudel, Chief Finance Section Gandaki Regional Hospital Mr. Jabbar Ali, Accountant DHO, Syngja Mr. Shankar Karki, PHI DHO, Syngja
64 Annex 3 Suggested Revisions To EHCS Targets and Indicators Note: Indicators highlighted in red are either redundant or have no easy way to be measured and so are recommended to be dropped. Indicators highlighted in yellow are recommended to be added (or suggestions for definitions) Indicator 1990 NHSP Baseline Target Latest Actual Tar MD (Year) 2006 (Year) get G 200 201 9 5 Outcomes (all are from DHS) MMR/100,000 live births 850 539 325 281 300 207 (1996) (2006) IMR/1000 100 64 50 48 45 (2001) (2006) <5MR/1000 162 91 70 61 65 48 (2001) (2006) Total Fertility Rate 4.1 3.8 3.1 3.5 (2001) (2006) Selected Intermediate Outputs Contributing to Outcomes 1. Family Planning, CPR (modern 24% 35% (2001DHS) 43% 44%(2006DHS) 4733 method) 34%(2000/1HMIS) 42%(2005/6HMIS) % 2. Reduce Maternal and Newborn Mortality Skilled attendance at birth (%) 7% 13% (2001DHS) 22%34 20%(2006DHS) 35 Health worker attendance at birth (%) 8.1% 2000/1HMIS 23.4% 2005/6HMIS % Births in health facilities 9% 2001 DHS 18% (2006DHS) % Births in EOC facilities % ANC (any health worker) 49% (2001 DHS) 72% (2006 DHS) 35% 2000/1HMIS 73% (2005/6HMIS) % of ANC patients receiving 4 visits 37% 100% 47.7% 100 100 2002/3 HMIS 2005/6HMIS % % % 15-44 women receiving TT vaccines % FCHV activities complete 3,4,5 Reduce IMR and <5MR % children with pneumonia receiving appropriate treatment Pneumonia cases in public sector 72 136 (including community) per 1000 kids 2000/1 HMIS 2005/6 HMIS % children with diarrhea receiving 46% 41% appropriate treatment 2001 DHS 2006 DHS % <1 immunised against measles 64% 2001 DHS 78% 80% 2006 DHS 85 77% 2000/1HMIS 88% 2005/6HMIS % % children fully immunized (age 12-23 66% 2001 DHS 83% 2006 DHS months) % Vit A coverage 81% 2001 DHS 90% 2006 DHS % iodized salt coverage (any and 97% 96% adequately iodized salt % of HHs) 2004 Mini-survey 2006 Mini-survey % malnutrition (>2SD under weight for 43% 39% age) 2001 DHS 2006 DHS 6 -9, 11 Reduce infectious disease burden DOTS available to all patients % TB prevalence
33 BP has 50% for 2009 34 BP 27%
65 Indicator 1990 NHSP Baseline Target Latest Actual Tar MD (Year) 2006 (Year) get G 200 201 9 5 % case finding of TB patients (of 11.1% 71% 80% 65% 90 expected smear positives) (1997) 2004 HMIS 2005/6 HMIS % DOTS treatment success rate 85% 87% 88% 2004 HMIS HMIS 2005/6 Leprosy prevalence rate (per 10,000 2.84 1.96 population) 2003/4 HMIS 2005/6 HMIS Leprosy new case detection rate (per 2.41 1.65 10,000 population) 2003/4 HMIS 2005/6 HMIS HIV prevalence, gen population 60,000 70,000 (numbers of infected adults) (2003 NCASC) (2005 NCASC) HIV prevalence, high risk groups (range for sex workers) % vul population using condoms for 63%-74% 66%-77% safe sex (sex workers on last contact (IBBS surveys (IBBS surveys 2006) with client) 2004) Malaria incidence (API) 0.36 0.32 (2004 HMIS) (2006 HMIS) Malaria deaths Leishmaniasis incidence (cases per 26 100,000 population at risk) (2006 HMIS) JE incidence (cases per year of acute 1,908 2,824 encephalitis syndrome) (2000/1 HMIS) (2004/5 HMIS)
Some of the indicators suggested for the NSHP-IP should be revised. Indicators that do not have any definition need to have one established, or can be dropped. Others have no reasonable source of information, or are not a priority at the strategic level (although they may be useful at the program level). On the other hand, some indicators that were not included may be more useful or available. The following are our observations and recommendations for ECHS indicators.
Mortality indicators. - These are all acceptable. - May want to add adult mortality (cumulative chance of death between ages 15 and 49), since that can be calculated from the DHS module that measures maternal mortality. It is only available when the maternal mortality measurement is done (maybe every 10 years). As under five mortality declines it is important to look at deaths in young adults and see if there are opportunities to reduce mortality beyond current programs (i.e. tuberculosis, maternal mortality reduction and HIV).
Family planning - Current indicators are good.
Safe motherhood/newborn - % of births attended by a SBA – Good - Number of BEOC/CEOC facilities per 500,000 population – Good, although the actual status is not reported in the HMIS volumes I have seen.
66 - % of all births in EOC facilities. I have not seen a source for this data or any report on it except for selected districts. If the HMIS is not going to be revised to show this it would be easier to track percent of births in any facility. - % of women receiving 4 ANC visits. This is sometimes written as % of women receiving ANC who get four visits. Either of these is not as relevant as a simple measure of % of women with at least one ANC visit. At least at this time ANC should be from any health worker. If limited to skilled birth attendants it gives the impression that ANC coverage is less than what it actually it. Also much of the difference is given by MCHWs, who are not SBA, but who are trained and expected to give ANC. Recommend tracking % of expected pregnancies with at least one ANC visit from any health provider. - % of women 15-49 receiving TT vaccine. It is not clear what this means. The adult TT campaign finished several years ago and so this is not a program area. A better indicator is % of pregnant women protected against NNT by TT. - Pregnant women target. The HMIS target for pregnant women for ANC and TT is too high (960,734 in 2006/2007). If we take the total population for the same year (26.2 million) times the NDHS 2006 birth rate 28.4 this give us 744,080 live births. The target is 29% higher than this. A few percent could be added to the live births to account for stillbirths (2.3% in the NDHS 2006) and late miscarriages (not measured). If even 5% is added the target should be 781,284. It appears that the HMIS is including early miscarriages, which occur in perhaps 15% of pregnancies. These occur in the first trimester nearly always before women present for ANC or TT services and so it is better to exclude them in a target for these services. - % of FCHV activities complete. There is no definition of this indicator. Recommend dropping this.
Sick Child programs - % of children with pneumonia who receive appropriate treatment. Since it appears that about half of children with pneumonia are treated in the private sector it is not possible to measure appropriate treatment. The DHS does not actually measure pneumonia so it does not provide information for this indicator. The nearest (and limited) proxy would be the rate of pneumonia treatments in the public sector per 1000 children per year (from the HMIS). This is good in showing whether the public sector is finding and treating more children as CB- IMCI expands, but it is limited in that there is no “target” rate and it is not known how this influences private sector treatments. - % of children with diarrhea who receive appropriate treatment. The DHS does measure diarrhea directly and one measure of appropriate treatment would be oral Rehydration Therapy (either ORS or more fluids of any sort at home), possibly along with zinc treatment. This is only available every five years.
Immunizations. - % of children under one with measles immunization. This is available from the HMIS annually. There are also problems that in the past immunization data was over-reported compared to the DHS, although that is not the case in 2006.
67 - The HMIS target for EPI for 2006/2007 is 748,074, which is roughly equivalent to live births based on HMIS population and DHS birthrates. This may be a few percent higher than children of EPI age, but is close enough. - % of children with all immunizations. This is not available directly from the HMIS, but only from the DHS and only every five years.
Nutrition - % Vitamin A coverage. This is available annually from the “mini-surveys” of about 18 districts and can be checked every five years from the DHS - % Iodized salt coverage. This is available annually from the “mini-surveys”. It is not in the DHS but can be checked against other periodic national surveys (last ones in 1998 and 2005). This should be tracked as two figures. % of households using iodized salt (any level) and % using adequately iodized salt (15 PPM). The first figure is over 90% and the second around 50-60%/ - % Malnutrition. The logframe does not indicate, but the most common single indicator is % of children below five years of age who are more than two standard deviations below the norm. The DHS provides this data. The international standard changed for the 2006 DHS, so corrections of prior survey figures have to be made. The HMIS tracks malnutrition, but the figures reported are much lower than the DHS results. The reasons for this are not clear, but it may be that mostly young infants are weighed at time of immunization. Since most malnutrition develops between 6-18 months of age, weighing infants younger than this will miss it. Recommend against using the HMIS figures for malnutrition.
Tuberculosis. - DOTS availability. Since all parts of Nepal have been covered since 2001 there is no reason to keep this indicator. By 2006 there were 560 DOTS centers and 2,795 sub-centers and their number has kept rising, but this is not needed as a target. - Case finding for sputum positive. This is a standard international measure and should be kept. - Treatment success rate for sputum positive. This is a standard international measure and should be kept.
Leprosy - Key indicators are Prevalence rate (which is rate of patients under treatment). The international goal for leprosy elimination as a public health problem is for this to fall below 1/10,000 population. In Nepal it is gradually nearing this goal (1.96 per 10,000 in 2005/6 compared to 2.84 per 10,000 in 2003/4) - New Case Detection Rate (new patients found per year) is another main indicator, which is also falling (1.65 per 10,000 in 2005/6 compared to 2.41/10,000 in 2003/4) - % of new cases with grade 2 or higher disability (which should stay low if cases are found promptly). - The above three indicators are enough to say that the program is doing well. In fact just the first indicator would be enough overall.
68 HIV. - Prevalence rate in general population. This is actually in the adult population. It is estimated every two years by the National Center based on surveys of high risk populations and extrapolations. Changes can occur as new data sources become available, so small changes may or may not reflect actual trends. Still it is a useful indicator (it may occasionally need to be adjusted post-facto). - Prevalence in high risk groups. This is based on periodic surveys of high risk groups. One problem is that with geographic divisions there are 5-10 such groups with varying numbers of surveys done, so this is actually a lot of indicators. - % Vulnerable population using condoms. This is based on the same periodic surveys of high risk groups and has the same problem of a number of groups surveyed.
Malaria incidence. This is usually the Annual Parasite Index, which is the number of laboratory confirmed malaria cases in the public sector per 1000 population (at risk). The problem is that most malaria patients do not present to the public sector and most that do come do not get a blood slide taken. The indicator can still track trends if the proportion coming and tested stays stable. If not, changes in the API will not necessarily reflect changes in the disease. The API for 2006 is 0.32, for 2005 is 0.25 and for 2004 is 0.36. The denominator is based on “at risk population” (65 districts). Although not optimal, the API is probably the best indicator for the malaria program. - The malaria program also collects a wide array of other information on number of slides examined per 100 population (ABER), the % of slides examined that were positive for malaria (SPR), the number of cases treated without a diagnosis, etc. These are useful for management within the program, but are not needed for ECHS tracking. - Malaria deaths. This is not reported in the HMIS Annual report chapter. The Hospital inpatient morbidity tables for 2005/06 showed 8 malaria deaths (and 852 inpatients), which may not be reliable, and even if it is, would indicate that malaria is a rare cause of death. I would drop this indicator.
Kala-azar. Cases registered. These are cases registered for treatment in the public sector Deaths. Known deaths among cases registered are shown for 2005/6. Patients who die before treatment or who drop out and die after treatment are not counted. 2004 2005 2006 Cases 794 1,169 1,341 Deaths 15 (Note – The HMIS hospital morbidity table shows 1,218 admissions and 19 deaths for 2005/06. Not all Kala-Azar needs to be admitted so the figures are not inconsistent.) - Disease rate is 26/100,000 per year in the 12 endemic districts (5.6 m population). This rises and declines from year to year.
69 - From a public health perspective the success of this program is in finding and curing a high percentage of cases, in what is without treatment a frequently fatal disease. It is not clear if the program actually reduces new cases over the long term. We could track mortality rates in registered cases, but the cure rates are always very high, so we would not have any targets other than to keep this high.
Japanese encephalitis - Between 800 and 2800 clinical cases of JE are reported each year from hospitals. (average about 1600). - Case-fatality rates are 5-20% depending on the year. This was much higher more than 10 years ago and is thought to have declined due to better nursing care. An average of 200 deaths per year are reported. Unfortunately many cases of JE have long term neurological damage, so deaths do not capture all the impact of this disease. - It is not known what percentage of JE cases do not come to the hospital. - In 2006 most JE clinical cases received laboratory testing, but only 22% were positive for JE. It is not known if this means that most clinical JE is not JE, or if the lab tests are missing most cases. - From a public health perspective, measuring whether the immunization programs have an impact on cases and deaths is the most interesting. This is not a simple indicator. - I do not have a recommendation for a simple indicator for this program.
Lymphatic Filariasis - There is no report of incidence for this disease in the LF chapter of the Annual report. Nearly the entire country is considered to be at risk. - 542 “filariasis” patients are reported in the morbidity listings of the Annual report. - The main program effort is universal drug treatment one a year for five years. This is underway in five districts and more are planned. - An indicator would be percentage of target districts (and/or target population) either having universal drug treatment in the past year or having completed five rounds.
70 Annex 4 Status Of NHSP Log-Frame Targets
Output, Current Status Comment Target, Indicator 1. Essential Health EHCS has been costed. Key programmes delivering the main Need to cost free services Care Services: EHCS health benefits are reaching the poor via comprehensive and scaling up and costed, allocated the coverage, services that are elective and that impose charges extending for NHSP-2 necessary resources mainly benefit the non-poor and implemented. Clear system in place to ensure that the poor and vulnerable have priority for access. 50% of health facilities A 3 year scaling up plan has been prepared for safer Indicator is difficult to provide prioritised motherhood, FP, child health, communicable disease control measure meaningfully, and elements of EHCS by interventions presently implemented only in selected districts. should be replaced by a 2006/7, rising to 75% Current status is:- limited number of more in 2009 Reproductive health- FP - all health facilities, Safe specific indicators related motherhood- antenatal/ post natal care- all health facilities; to specific EHCS BEOC- 47 district -67 sites, CEOC -32 districts- 36 sites, safe programmes, taken from abortion 71 districts -170 sites (81 private) their forward plans. Every Child health – immunization all health facilities; IMCI - all service is being provided health facilities of 48 districts, scale up to all districts in next at health facilities, but 2 years; nutrition- all health facilities there are quality and Control & prevention of communicable diseases – malaria- access issues. The all health facilities of endemic area, TB- 60% health facilities proposed service delivery of all types and 100% at district level, condom distribution for survey will (inter alia) help prevention of HIV infection - all health facilities to check quality and Outpatient care- all health facilities access, draft TOR has been developed,
50% of population Coverage of most public health interventions exceeds 50%, Replace target with a utilising prioritised but OPD contacts per head of population are 38% in 2005/6, limited number of more services by 2006/7, % not increasing since 2002/3. specific coverage rising to 75% in 2009 indicators. -User charges are a major constraint on utilisation of curative services, together with low quality services 1.3. Proportion of poor - Only 8% of poorest attended by health worker, SBA is even Impact evaluation is accessing skilled birth lower. More SBAs being recruited and upgraded, facilities underway attendants increases. being improved, maternity incentive scheme started July 2005 to address demand side and staff incentive issues; but unclear guidance, delays in payment by DFID, financial management problems have so far limited the impact. % of poor using Low coverage of pilot schemes, small percentage of poor Delete this indicator. community health receiving subsidy Limited relevance of insurance indicator as free services are extended 2. Decentralisation: Local responsible bodies are capable of managing health facilities in a participative,
71 Output, Current Status Comment Target, Indicator accountable and transparent way with effective support from the MOHP and its sector partners. 5 year rolling plan for Decentralisation on hold pending clarification of future federal Lack of decision-making extending devolved structure. Very centralized system prevails, MOHP controls authority encourages health service staff, determines plans and budgets (over-riding district plans), passivity and inhibits management, taking undertakes most procurement. Districts have little discretion implementation. Increased account of the security other than over funds they mobilize via CDP, and detailed delegation need not await situation, endorsed by planning of funds within centrally determined earmarked political decentralisation. July 2005 budgets to be spent in conformity with detailed guidelines prescribed by central DOHS directors. Deconcentration of Decentralisation on hold pending clarity on State structure. management to 15 MOHP recently initiated a process of delegating some Districts by 2006, 30 logistics and financial authorities to district level, some district by 2009 procurement, but limited in scope and mixed results (e.g. higher prices for ORS). Increase in district budgets, but all earmarked. 1800 SHP managed by 1424 facilities in 28 districts, orienting 12,816 staff and some Delete this target, at least LHMC by 2006 management committee members. no new ones added in 2006 until there are local elected bodies established to own the handed over facilities. Ownership but no power to manage staff or significant resources- no elected bodies 5 autonomous District A total 17 District hospitals granted increased autonomy under Suggest dropping this Hospitals by 2006, 10 a Management Board. In total, 52 of the 88 public hospitals of target or clarifying by 2009 all types have semi-autonomous status, though the extent of objectives and scope. their autonomy varies. No progress on public private ‘Autonomy’ mainly relates partnerships to run public hospitals, of the 2 cases, 1 predated to freedom to set charges NHSP, 1 added in 2004/5 (Dec 05 Aide Memoire Annex 5). and manage own collected Revised proposal to contract out two more district hospitals by revenues, little discretion May 2006 not implemented. over other budgets or centrally recruited staff. 2.3. Five districts More than 45 districts prepared District Periodic Plans (DPPs) - MOHP and DOHS did having their own five for 5-7 years including health; however, budgets do not relate not recognize DPPs and year plan including to the plans, implementation was not effective in all sectors did not provide resources health by 2006/7 and including health. and policy support to 10 by 2009. district level institutions for implementation. Drop as a quantitative target, might replace with agreement on a more participatory AWPB process. 3. Private/NGO sector development: The role of the private sector and NGOs in the delivery of health services is recognised and developed with participative representation at all levels which ensure
72 Output, Current Status Comment Target, Indicator consumers get access to cost-effective high quality services that offer value for money. Strategic plan, Committee formed and met once, but the objectives of PPP The ‘strategic plan’ may timeframe, regulatory are not clear in the absence of a policy and strategy or a be a solution looking for a framework for MOHP, consensus on way forward. Private sector is engaged and problem, a more pragmatic NGO, private working with MOHP in some key areas (e.g. training doctors). case by case approach to partnerships produced Private sector assessment proposal with WB funding is under choosing the best by MOHP and key NPC consideration, and if implemented may help clarify institutional arrangements stakeholders, endorsed issues. in specific areas would by July 2005, 1st wave make more sense. implemented with private and NGO partners by July 2006 Coordinating body Not done, procurement & contract consultants not able to be Benefits of the contracting with legal and contract recruited. out model are unproven in management capacity Nepal context, drop this established in MOHP target and meeting monthly by Sept 2004 Number of service Nothing new since start of NHSP Drop this target. Rationale delivery agreements is unclear. A solution with private looking for a problem sector/NGOs At least 5 hospitals - Bayalpata Hospital, Achham partnership proposal is under Drop this target. There has fully transferred to study been rapid growth in NGO/private sector Am Pipal Hospital, Gorkha -2004 with community private hospital beds, it is operation unclear why transferring 5 GON hospitals should be an objective Service provider A couple of examples (Kalimati NGO Chest hospital for Drop this target. agreements, including Rheumatic fever, HOPE Nepal for supporting district Commitment should be to those enabling transfer planning) sound institutional of public resources to arrangements for NGOs and private sustainable and efficient sector, designed and service delivery, not to a endorsed by July 2008, specific ideological operational by July approach 2009 Number of EDPs No system for collecting this information, unclear what use it Drop this target. MOHP supporting NGO or would be if we had it. No progress on harmonizing support to will wish to know what private partners via non-Government health partners? large NGO and private MoH budget, or using partners are doing (though harmonized reporting have limited capacity to and management process the data), and procedures for such sustainability may be support marginally more likely if funds go via the budget, but slow and inflexible GON procedures may damage scope to support innovation. 4. Sector management Coordinated and -Health Sector Strategy -2003 & Nepal Health Sector Program JARs are parallel and consistent sector as a sectoral program operational additional to MOHP management (planning, -Initiation of sectoral budget support from DFID & World planning and budgeting
73 Output, Current Status Comment Target, Indicator programming, Bank as a pool fund & other EDPs as earmarked projects processes. budgeting, financing, -‘Statement of Intent’ signed by 11 EDPs in Feb 2004. Impact of NHSP on health and performance -‘Code of Conduct’ agreed by EDPs sector outputs or outcomes management) in place - JAR meetings held twice per year is debatable (see text). within MOHP - Health Sector Development Partners Forum and EDP forum See recommendations on supported by the EDPs, established and meet regularly SWAP management. to support service - Health Sector Reform Unit (HSRU) established. delivery with the involvement of NGOs and private sector MOHP restructuring, MOHP restructuring has not progressed since 2005 merger of strengthened planning, population wing in FHD. There is some duplication and programming, serious over-centralisation, but DoHS planning and budgeting, monitoring, programming is effective at divisional level. Weak links from and deconcentration to plan to budget partly reflect systemic problems, though some Regional & District progress could be made towards more transparency and level planned, agreed, greater delegation to program managers. NHSP progress has implemented been limited by inability to recruit staff and consultants, but recent strengthening of HSRU and start of TA support should help. Detailed MOHP Relevant consultancy studies on re-organisation nearly It is not clear that MOHP organisational analysis complete, but fragmentation of organisation reform studies restructuring can solve the including HR systems, will be unhelpful to agreeing an overall action plan. main management information systems, problems, which are partnerships at all system-wide and related to levels. Restructuring attitudes and incentives plan produced and rather than organizational endorsed by July 2006, structures. Phase 1 implemented by July 2007 Efficiency savings None yet identified (or likely to be?) Drop this target reflected in MTEF Partnership policy and ‘Statement of Intent’ signed Feb 2004 Code of conduct is a vague framework document Code of conduct agreed by EDPs, MOHP unclear if they need statement of intent, no agreed (timing to sign it clear obligations agreed to unspecified) by EDPs No of joint annual EDPs are involved in joint planning at division level, e.g. Drop this target (can’t be planning and review consensus forecasting of FP supplies. Limited involvement of measured, meaningless if it EDPs in overall MOHP planning and review processes, JARs could). Quality of overall are separate participation in joint planning and budgeting of NHSP is the key point, coordination across programmes and across NHSP remains weak 5.Health financing resource management: Sustainable development of health financing and resource allocation across the whole sector including alternative financing schemes in place
74 Output, Current Status Comment Target, Indicator % of HMGN Budget Has Drop target, no basis for for Health increased increased deciding what priority from 5% (year?) to steadily health should receive 6.5% in 2006/7, 7.7% to 7.2% relative to other sectors. in 2009 Could replace with softer in 2007/8 requirement for domestic financed health spending to share in the growth in real domestic revenue. Number of EDPs using WB and DFID the only donors providing pooled funding. No Drop this target (indicator harmonised reporting progress on wider harmonisation agenda? is not defined nor and management measurable) procedures, and making financial contributions to partnerships directly through MOHP budget, even if earmarked. At least 10% of health No elected local bodies in place. Requires field survey to Drop target pending clarity spending born by collect data, but no PER undertaken since May 2004 due to on decentralisation. elected local bodies by lack of HEFU capacity. - Some budget from local bodies 2006/7 (DDC, VDC) goes to local health facilities; size of budget provided is not consistent. At least 5% of health No progress on CHI, but CDP revenue NR53mn, less than 1% Drop target given new user expenditure born by of health budget. Community developing emergency health charge policy. local communities in funds in many districts public health facilities by 2006/7, e.g. CDP,CHI Increased financial No information available (waiting for NHA report). User Drop target or define it contribution from charge policy implies reduced role for out of pocket better. Private share in private sector expenditure on basic services, private role in tertiary continues financing is too high for to grow. - Private Health Sector Assessment is planned equity objectives, and should fall with user charge policy; private investment in health is dynamic, but MOHP only influences it indirectly. Efficiency savings None identified yet, limited significance given employment Drop target until efficiency from organisational policies and scaling up of expenditure savings are identified. review factored into MTEF by July 2005 Tertiary share of EHCS 70% of 2006/7 budget, as envisaged in NHSP-IP, and spending frozen, EHCS was 60% of planned and actual spending in 2004/5. increased from 2006 Needs based resource A draft has been completed, agreement unlikely until federal Drop target for now allocation system structure is agreed. designed and piloted by 2008 Alternative financing Extension of free basic services for the poor in some districts Monitoring the impact of and safety net and demand side subsidy for safe deliveries was implemented changes in user fee policy arrangements for most from 2006, free basic services policy for all is now being is a high priority, together vulnerable piloted by phased in at SHP/HP level initially with reacting to changes in 2007 demand in order to ensure quality does not suffer. National guidelines for Policy has moved rapidly, recently promulgated guidelines user fees produced and already overtaken by further extension of free services to all
75 Output, Current Status Comment Target, Indicator adopted by 2007 SHP/HP. Different models of No progress Drop target given policy community health on user charges. insurance designed and piloted by 2007 6. Logistics management: Systems established and resources allocated within MOHP for the effective management of physical assets and procurement, distribution and rational use of drugs, supplies and equipment Stock outs of EHCS Drug availability stock out study completed, and shows some indicator commodities improvement. fall - pull and push system initiated. - CDP in place. - buffer stock of drugs initiated at Regional Medical Store level Drug financing On track. By end 2004/5, 27 districts operating, 5 more Drop target, given schemes in 50% of initiating activities, 4 endorsed a district plan of action to implications of abolishing districts by 2006/7 introduce CDP, a total of 36 from 75 (48%) charges for basic services LMIS with Will be implemented as decentralisation proceeds. decentralised data processing at district implemented by 2008 Procurement decisions Procurement plan for 2006/7 not prepared and shared with are based on LMIS by EDPs by June 2006 (when was it?) 2006/7 Procurement systems Some modest decentralisation of equipment procurement to RTI to support training in reformed by 2008 hospitals and districts in 2006/7. Buffer stock established for new procurement act medical stores. Essential drug Started in 6 districts in 2004/5, training started to extend to a procurement converted further 8 in 2005/6. from ‘push’ to ‘pull’ by Update from what source? Check annual report 2006 National drug policy Draft is ?still? awaiting Cabinet approval. developed and implemented by 2007 Plans for disposal of National Waste management Steering Committee formed T2 biomedical waste 2006/7 developed and implemented by 2008 Equipment in all Annual maintenance plan prepared and is being used to inform facilities maintained to budget priorities a bit vague, how is it being used? MOHP norms and standards (included in purpose column, but no OVI defined) 7. Human resource Effective HR policies development: Clear undermined by inability of and effective HRD HURDIS to produce policies, planning essential basic data on staff systems, and programs establishment, in post, and
76 Output, Current Status Comment Target, Indicator developed and vacancies functional % (unspecified) of Vacancy rates low for most staff except Doctors, where action Replace with more specific public health facilities to recruit is having significant impact in reducing the gap (200 and measurable will have appropriate recruited c.f. 300 shortage in 2005/6).Proposed study of disaggregated indicators of mix of HR by 2006/7 staffing skill mix and actual deployment not started, some vacancy rates for skilled limited data collected in 2006 drug study. Useful measures to staff. increase training of doctors, make registration dependent on 2 year service with MOHP HR master plan HR management master plan is available, but is not being produced, endorsed by implemented. MOHP, implemented by July 2006 HRD unit reformed Done, with additional officers, but has not improved HR and re-located within management MOHP by 2005 Training information TIMS introduced, begun to populate it with data, though only Does not address lack of management system training included in the budget ‘Red Book’ is being captured. coordination between redesigned to capture programmes on training all major training course data by 2005 % (unspecified) of Important, but no source of data has been identified for this transfers and postings indicator. in line with published policies and rules Medium term training Under procurement, though response to the invitation to bid This is a core, annual strategies for AWPB was disappointing. planning and management by all Divisions and responsibility, consultancy centres by 2005, studies will be quickly reviewed for outdated and of little help consistency with HNSP-IP All training facilities Unclear target appraised by 2006 A ‘mechanism’ Unclear target, drop established to respond to projected health personnel needs by 2007 8. Integrated MIS: Comprehensive and integrated management information system for the whole health sector designed and functional at all levels as well as quality assurance mechanism in place for public and private sectors Comprehensive & Achieved for public sector, with monthly reporting Main gaps are incomplete integrated MIS in place consolidated centrally, annual report with summary and reporting from private and at all levels by 2007 district level detailed statistics published within 6 months of NGO service providers, year end. lack of integration of performance and financial data, data on gender and minorities.
77 Output, Current Status Comment Target, Indicator Quality assurance Process underway for agreeing draft QA policy involving all policy for public and stakeholders. District QA teams have been established, there private sectors created are plans to train them. and implemented (date unspecified in Log Frame)
78 Annex 5 The Impact Of Free Basic Services
Current Policy On Charges Policy on user charges has moved quickly, and statements in different sources are not always consistent with each other. The Ministry of Health and Population (MOHP) intends to move to universal free essential health care (EHC). However, the pathway to this end is not yet defined. This annex tries to present a coherent picture based on the study by RTI, the Government ‘operational guidelines’ produced in 2007, and the consolidated comments on the first draft that were prepared by the EDPs. The three sources are not entirely consistent with each other.
By October 2007, various extensions to the policy had resulted in the following services being declared to be free of charges:- Following an anouncement in October 2007, all services at health post and sub health post level in all districts; In low-HDI districts, both in-patient and out-patient care in district hospitals; In other districts, out-patient care in district hospitals continues to levy charges, while in-patient and emergency care is in principle free for the poorest (those able to feed the household for six months or less) and subsidised for the poor (those able to feed the household for six to twelve months).
In all districts, those assessed as having an income sufficient to feed the household for six months or less are supposed to receive free emergency and in-patient treatment in district hospitals, covering everything from registration to consultation, treatment, minor surgery, obstetric emergency, X-rays and lab services, drugs for the first week, and other logistic charges. Those with an income thought to provide food for 6-12months are charged half the normal price.
Health facilities are intended to receive additional funds from central Government to compensate them for the loss of income, plus provision for the additional costs they will incur as a result of increased demand resulting from the price reduction.
Budget provision was made for the initial policy in 2006/7, and has been further increased in 2007/8. The detailed guidance on the policy contains tables showing budget provision for ‘emergency and free services for the poor and marginalised’ of NRs 80mn, plus a further provision of 114mn for free services including drugs, plus NRs 17.6mn for ‘social exclusion’, and increased provision of drugs for hospitals of NRs 13mn based on a standard NRs200,000 per hospital. This sums to NRs225mn. It is not readily identifiable in the budget, but we were told that it is shown as ‘subsidy social security’, part of the big increase in provision for ‘integrated district health program’. This includes a provision of 226mn, which is of the right order of magnitude. The detailed cost tables in the guidance show that the budget includes associated training, sensitization, and printing costs for forms and registration documents. The budget allocation table shows all districts receiving a significant budget increase for free services, though the more detailed cost
79 calculations imply that some services will be focused on low human development index districts. The budget provision for the policy does not appear explicitly in the AWPB.
A key question concerns whether the budget provision is adequate to cover the policy commitment without damaging the quality of the service, and what additional provision will be needed in order to further extend the coverage of the policy to universal free basic care, as the Minister of Health wishes to do.
If taken at face value, the targeted policy would apply to roughly 60% of the population in the selected districts, with 30% receiving the designated services for free, and a further 30% receiving the 50% subsidy. The experience of other countries suggests that this objective will prove difficult to achieve without an investment in the targeting mechanism that is unlikely to be justified if undertaken for health alone. Experience from other countries suggests that it is not too difficult to administer a system in which nearly everyone pays, or one in which almost nobody does, but the intention to exempt 30% and charge half price to a further 30%, in a situation in which the criteria are discretionary and hard to apply, invites disputes, and has the potential to encourage corrupt inducements. In the district that we visited, where the policy of targeted subsidies for emergency and in-patient care has been applied since July 2006, we were told that just 237 patients were supported for free or subsidized treatment, less than 10% of emergency and in-patients treated in the district hospital alone. The district health officials commented that there has been no increase in demand as such, but the scheme was useful in helping patients to cope with high bills. Of course, it would be absurd to generalize from one district. However, the finding that institutions draw their definition of who is poor very narrowly was also found in evaluations of the CDP, and is repeatedly found across the world, especially where the criteria are hard to assess, and the institution is unsure whether and when the loss of income will be replaced. We were told that patients know they must pay, and they do not make the journey to the facility without first scraping together the cash. The fact that they can pay does not mean that they necessarily should be asked to: - they may have incurred debt or sold assets or called on the charity of equally poor neighbours, and the cash reserves used to pay the bill may mean the household going hungry, especially if it is the breadwinner who is hospitalized
Cost Of Free Basic Services Parasai has estimated the cost of free in-patient and outpatient services up to and including district hospital level based on varying assumptions as to the number of districts covered, the extent to which services are universal or targeted to the poor, and the impact on service utilisation35. The real resource costs of the policy are the costs of meeting the additional demand for services that is expected to result from the reduction in price, in other words the extra medicines, materials, staff time and other costs incurred in providing additional services. In addition to these real costs, Government has to provide for the shift in the burden of paying for them, away from the users of the service towards the Government as the provider. If existing and increased patient demand is to be met without loss of quality, Government needs to provide an additional budget to health facilities in order to compensate them for both the loss of income from existing patients, plus the need to provide for whatever additional demand results from the policy.
Table 5.6, based on Parasai, summarises the estimated financial cost to Government.
35 RTI, 2007
80 Table 5.6 Estimated Cost of Free or Subsidised Services
TARGETED TO THE POOR UNIVERSAL Free to poorest 30%,half price to next 30% Free to all Total demand, Numbers Total cost Rs 000s benefiting Mns Total cost Rs Mn Outpatients, 25 low HDI districts 25% demand increase 3570 2177 96.5 210.6 75% demand increase 4998 3049 135.1 294.9
Outpatients, all districts 25% demand increase 13943 8,366 370.2 819.3 75% demand increase 19521 11,713 518.3 1147.1
Emergency Care, all districts 20% increase 198 121 40.4 87.0 30% increase 214 131 43.8 94.2
Inpatient care, all districts 20% demand increase 123 102 49.1 85 30% demand increase 149 110 53.2 92.1
TOTAL COST 1.OPD just 25 districts Low demand increase 3891 2400 186.0 382.6 High demand increase 5361 3290 232.1 481.2
2. All districts Low demand increase 14264 8589 460 991 High demand increase 19884 11954 615 1333 Source: Parasai, September 2007
The Parasai paper uses the best available secondary sources in order to estimate unit variable costs, and applies them to estimate the total costs. It is assumed that, given the under-utilisation of both staff and facilities, the additional demand can be met without further investment and without requiring additional staff to be hired. This is a reasonable starting point although the staff assumption could perhaps be questioned, on the grounds that some performance-based financial inducement may be required in order to encourage staff to spend more time on their official duties, which will require them to squeeze the time available for their private practice. Arguably a more questionable assumption is that the costs of identifying the target population and managing the administration of targeting appear not to be included. The argument used is that there will be other policies that require the poor and the poorest to be identified for the purpose of targeting benefits to them, and the costs should not be applied to health alone. However, experience from elsewhere is that the administration costs of maintaining records on which households should receive free health care, plus the additional costs to facilities of reporting costs incurred and obtaining reimbursement can be substantial as a percentage of the total benefits provided. The cost estimate also does not include the initial start-up costs of orienting staff and patients to the new system of charging.
At the time of writing, RTI were also trying to clarify what adjustments need to be made for the fact that a significant proportion of outpatient visits are already free of charge for specific categories of patient and specific diseases. The actual incremental cost could
81 therefore be significantly lower when services that are already free are taken into account. This means that the cost of extending free services to existing users is over-estimated, although the additional demand that will be attracted presumably relates to paid services only, since there should be no impact on services that are already free.
There are dangers that the policy may result in a perceived decline in quality if free services are not accompanied by a sufficient increase in the budget to fully fund the increased cost, including prescriptions for the additional patients attracted into the system. The table appears to suggest that the previous policy, before the extension of entirely free services at health post and sub health post level, would have cost NRs186- 232mn, which is in line with the budget provision. However, it is far short of the likely cost of extending entirely free services at this level, unless ‘free’ is defined to exclude the cost of drugs that would need to be bought from either a private pharmacy or from the CDP. If patients are still faced with significant out of pocket costs for drugs, the objective of significantly reducing barriers to access will not be achieved.
The table sheds light on the affordability of extending the policy to free and universal access to OPD , inpatient, and emergency services up to district hospital level. This approach is more likely to encourage people to attend when they are sick, and to bring patients earlier in their illness when full recovery is both more likely and less expensive in treatment. It avoids the risk of poor patients being incorrectly asked to pay, at the cost of providing free services to some who could have paid. Although some of the better off will benefit, many of them will continue to patronize private services, or will demand additional services not covered by the policy (for example, drugs not included in the key commodities or the essential drugs list, or in forms such as capsules not normally provided). Some of those who will benefit may not be within the poverty definition, but may be at risk of becoming poor as a result of user charges and the loss of income through illness.
The cost of universal access, based on Parasai, is in the range Rs990-Rs1333mn pa ($17- $22mn). On his assumptions, the bulk of these costs relate to free outpatient services. This estimate assumes that all existing out-patient contacts cost the patient NRs59, and thus it may over-estimate the marginal cost if a significant share of them are in fact free. The alternative approach of targeting 30% poorest for free services and a further 30% for half-price would, on the same assumptions, cost Rs460-Rs615mn ($8mn-10mn). The additional costs of extending free services to all are thus only $9-$12mn per annum on assumptions that may in fact be pessimistic. Moreover, to make a fair comparison, we need to add to the cost of targeted services a realistic estimate of the costs of setting up and maintaining a system for identifying the poor, ensuring that they receive the benefits they are entitled to, recording the free services given, and ensuring that the institutions providing services receive the necessary increase in their budgets to compensate for the additional financial costs. Allowing for these targeting costs, the additional financial burden of universal free services compared with subsidies targeted to the poorest 60% will be negligible, and could even be negative.
82 The free service policy transfers costs from private pockets to the Government budget. For existing patient demand, before considering any increase as a result of price reduction, the figures imply that Government would incur costs of Rs370mn ($6mn p.a.) just to provide for free and universal services to existing patients at district level and below. This cost is far higher than the reported user charges that are collected via the Community Drugs Programme, which were around NRs53mn in 2005/6. The remaining Rs317mn difference may partly reflect the problem previously discussed, that a significant share of existing OPD contacts are in practice already free. It may also reflect user charges not captured in the CDP figures (there are charges in some districts where CDP does not operate). The largest element, however, is likely to represent the cost of Government taking responsibility for out of pocket costs that are at present met by the patient purchasing from the private sector, often from pharmacies run by the staff of public health institutions.
It is common for medical staff to prescribe drugs that are not available in the public facility, or to require the patient to supply their own consumables such as gauze, bandages, or plaster for fractures. Free and universal basic services implies that the Government would take over the responsibility for financing these costs. If this is done by the facility directly supplying the required drugs and consumables, the implication is that private pharmacies and other suppliers would lose turnover of up to Rs300mn, on which a 20% profit would amount to Rs60mn. We have been told that private pharmacies are nearly universal among health sector medical staff. Most of their income is said to come from sale of drugs and other items rather than via consultation fees. Government taking on responsibility for directly supplying medicines and consumables required for extending free services therefore implies a loss of income to these staff. There are nearly 8,000 medical staff, in all categories, working in regional health directorates. If 80% of the lost profit would have accrued to MOHP workers via their private pharmacies, the average income loss would be Rs7,500 or $125 per annum. This is significant, as staff are in effect being asked to work longer hours in order to see more patients, while their income suffers from reduced private income from their pharmacies. The scale of the reduction in income, based on these figures, is not catastrophic, and could be made up as a result of additional prescription items charged to those not satisfied with the range of drugs and supplies available for free. Nevertheless, there is a strong case for piloting a performance based scheme to give staff appropriate incentives to treat the additional patient load, while helping compensate them for additional hours and reduced income. The ADB have designed such a scheme that is ready to be piloted, and would be a useful complement to phased introduction of free services.
The analysis by Parasai makes a good attempt to estimate the rough order of magnitude of the impact of abolishing user fees based on available secondary sources, but this discussion shows that there are considerable uncertainties regarding the costs and the scale of the increased demand. The assumed 20-30% increase in inpatient demand could for example turn out to be an under-estimate in some areas where physical access is not a barrier and where staff are relatively more available. One of the problems with abolition of fees is that the impact is likely to vary considerably by district, and by institution. A resource allocation formula that applies the same average increase across the board will
83 over-compensate facilities in areas where lack of staff or high transport costs limit demand; whereas facilities in high-demand areas may find the budget provision is grossly inadequate. Introduction of free services needs to be allied to introduction of a new approach to allocating resources between districts. This needs to be a balance between responding to where demand is strong (and providing staff with budget and other incentives to increase it), while tackling both demand side and supply side barriers that may result in low utilization of services and poor health outcomes in some districts.
Affordability of Free Basic Services The 2007/8 health budget is NRs12.1bn. The NR1.3bn upper estimate of the cost of free and universal public services would thus represent an increase of about 11% on existing red book spending levels on health, but 22% of GON financed budget expenditure on health. As a share of total 2007/8 public expenditure on all sectors, it is 0.8% of the total Red Book budget, and 1% of the total GON financed budget. This is a significant increase in the health budget, and would pre-empt spending on other critical expenditures that need to be scaled up and that will have a more predictable short-term impact on mortality and morbidity. The extension of free universal basic services is being phased in by starting with the health post/sub health post level, the services that are especially heavily used by the poor. Extension to PHC and District Hospital level could perhaps be phased in gradually, starting by extending it to more relatively low HDI districts, and gradually extending to more districts as the growth in Government revenue permits. This would ensure that the initial impact concentrates the benefits mainly on the poor. Alternatively, the definition of what is covered could be extended more narrowly, explicitly limiting what is covered to defined specific treatment interventions that would be covered for major causes of death and morbidity, in other words further extending the current NHSP practice of exempting specific health interventions from charges. . This would also help to limit the cost by preventing over-prescribing financed from Government funds.
84 Annex 6 List of References Acharya,Dr. Meena ,UNFPA, Gender Equality and Empowerment of Women, 2007
Code of Conduct for Partnership in Health
Department of Health Services, Ministry of Health and Population, Annual Report 2004- 2005
Department of Health Services, Ministry of Health and Population,, Annual Report 2005- 2006
Department of Health Services, Ministry of Health and Population , New Era, USAID, Nepal Demographic Health Survey, 1996, 2001, 2006
DoHS, MoHP, National FCHV Program Revised Strategy, 1990
DOHS Family Health Division, Consolidated Report of Regional Review Report/Orientation Workshop, RH program, 2007
Equitapproject, Working Paper #3, Who benefits from public spending on health care in Asia?
Foster, Mick and Raghav Regmi, Review of Nepal health Sector programme, A Background Document For The Joint Annual Review , October 2006
Government of Nepal, Consolidated Financial Statement, 2005/6, Financial and Comptroller General’s office,2007
Institute of Medicine, Tribhuvan University/United Nations Population Fund (UNFPA), Status of Reproductive Morbidities in Nepal ,2006
Ministry of Finance, Nepal: - Estimates of Expenditure for Fiscal Year 2006/7 and 2007/08, - Source Book of projects Financed with Foreign Assistance, 2006/7 and 2007-08
Ministry of Health, 2004, Nepal Health Sector Programme – Implementation Plan 2004- 2009, October 2004
Ministry of Health and Population, Three year Plan, 20064/65-2066/67
Ministry of Health and Population, Business Plan for Health Sector, FY 2006/07-2008/09
85 Ministry of Health & Population, Department of Health Service Annual Work Plan & Budget 2064/65(2007-2008)
Ministry of Health and Population, Health Sector Reform Unit Government of Nepal, August, Budget Analysis 2007-08, Ministry of Health and Population, 2007
Ministry of Health and Population Government of Nepal ,Functional Analysis of Ministry of Health and Population, 2006
Ministry of Health and Population, with the technical support of Health Sector Reform – Support Programme, RTI International, Draft: Rapid Costing of Free Health Care, Policy of Government of Nepal, Health Economics and Financing Unit, l, 2007
Ministry of Health and Population , Survey of Availability, Distribution, Use and Management of Drugs, Vaccines and Medical Supplies in Government Health Facilities, 2006
MoHP, Health Sector reform Unit, Nepal Health Sector Program, Status Report, Fifth Joint Annual Review of Health Sector, 25 June-1 July 2007
MoHP, NHSP , Joint Annual Reviews, Aide Memoires July 2007, Dec2006
MoHP , JAR status report work results update 2006
MoHP, HSRU, Report presentation JAR
MoHP, HSRU, Updates on second JAR report
MOHP Family Health Division, New ERA, USAID, An Analytical Report on National Survey of Female Community Health Volunteers of Nepal, June 2007
MoHP National Skilled Birth Attendants Policy Supplementary to Safe Motherhood Policy 1998
MOHP, Health Sector Reform Unit, Draft: Equity Analysis in Resource Allocation to Districts, (A review of the existing resource allocation pattern and development of formula for resource allocation to districts) , 2007
Ministry of Health and Population, Operational Guideline of "25 bed hospital, PHCC, HP, SHP based Free Essential Health care services to Poor and ultra poor patients" 2007
86 MOHP, Piloting of Performance-based Management System in Ministry of Health and Population, Highlights of Activities and Draft performance Improvement Plan for Sub- Health Posts, February 2006
MoHP, DoHS, Maternal Incentive Scheme, 2005
Nepal Family Health Program (NFHP)/ /Valley Research Group (VaRG) Nepal Family Health Program Mid-Term Survey September 2005
Nick Simon Institute/C T E V T, A Focused Study of CTEVT Mid-Level Pre-service Health Training Programs in Nepal 2006
Quinley, John, The Treatment of Childhood Illness in Nepal. The roles of the public sector, private sector and FCHVs. Analysis based on the NDHS 2006. DRAFT REPORT September 23, 2007
Powell-Jackson, Timothy,Suresh Tiwari,Basu Dev Neupane,Jo Morrison,Anthony Costello, Evaluation Of The Maternity Incentive Scheme, Report of the Process Evaluation, September 2007
REGMI, SS, Report on Health Sector Decentralization Strategy of Nepal, 2004
RTI International, Supplemental Workplan, 17 Septembet 2007- 30 June 2010
Shrestha, IB, An Outcome Assessment of Sub-health Post Handover in selected health institution(2005)
UNGASS National Report: Nepal HIV/AIDS Country Annual report, 2005
Upadhya T R and Company, Findings of Financial Management Review of Health Sector Program (HSP) for FY 2004/05 & FY2005/06, March 2007
World Bank Nepal, International NGOs and NGOs in Health (Contribution, effectiveness and expenditures) and Framework of partnership between public and private not-for profit sector , 2004
World Bank, Nepal - Resilience amidst conflict: an assessment of poverty in Nepal, 1995-96 and 2003-04
World Health Organisation, International Health Partnership- Concept Note for Nepal, and accompanying working papers on essential health care services, HMIS, user fees, community drug programme, skilled birth attendants, decentralisation, and the referral system
87 88