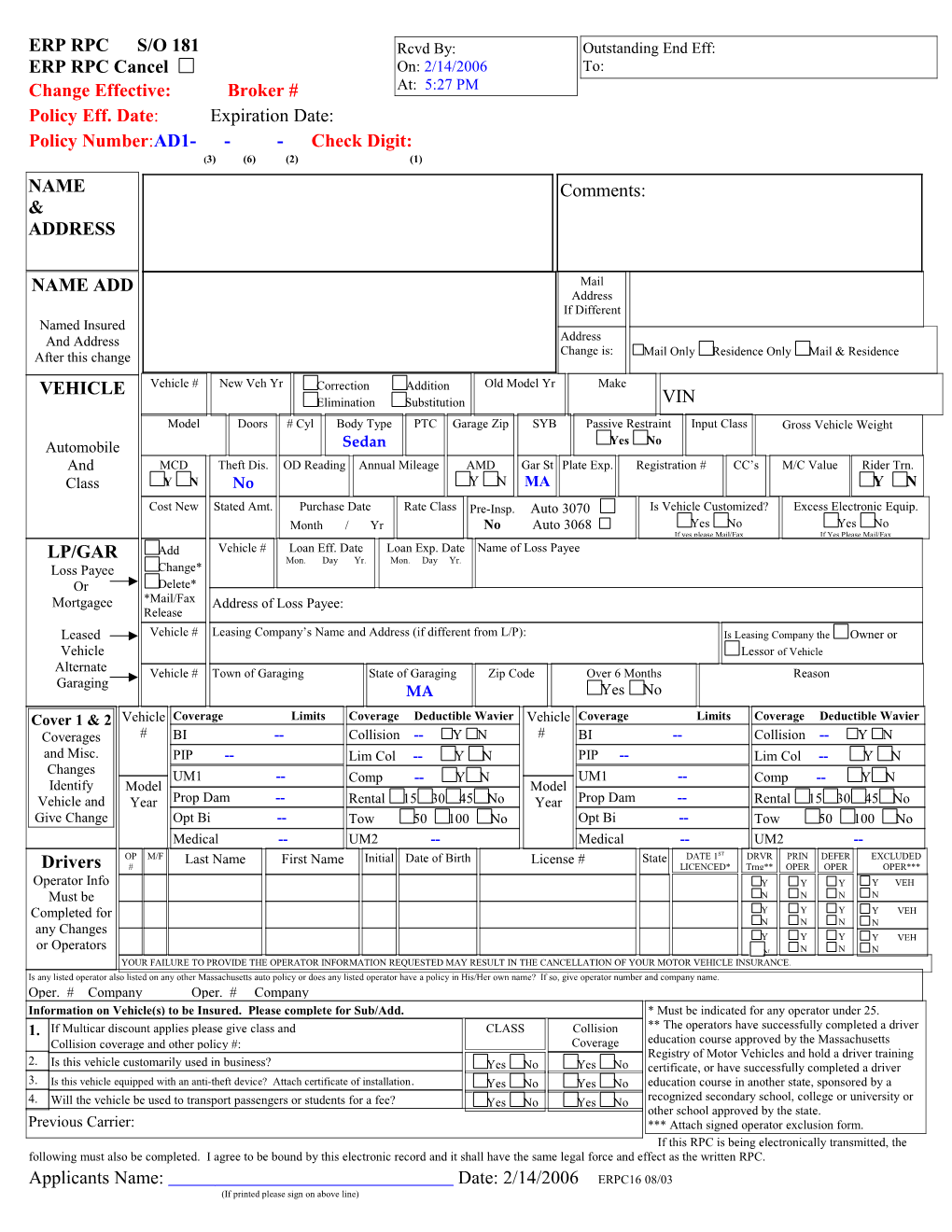
ERP RPC S/O 181 Rcvd By: Outstanding End Eff: ERP RPC Cancel On: 2/14/2006 To: Change Effective: Broker # At: 5:27 PM Policy Eff. Date: Expiration Date: Policy Number:AD1- - - Check Digit: (3) (6) (2) (1) NAME Comments: & ADDRESS
NAME ADD Mail Address If Different Named Insured And Address Address After this change Change is: Mail Only Residence Only Mail & Residence VEHICLE Vehicle # New Veh Yr Correction Addition Old Model Yr Make Elimination Substitution VIN Model Doors # Cyl Body Type PTC Garage Zip SYB Passive Restraint Input Class Gross Vehicle Weight Automobile Sedan Yes No And MCD Theft Dis. OD Reading Annual Mileage AMD Gar St Plate Exp. Registration # CC’s M/C Value Rider Trn. Class Y N No Y N MA Y N Cost New Stated Amt. Purchase Date Rate Class Pre-Insp. Auto 3070 Is Vehicle Customized? Excess Electronic Equip. Month / Yr No Auto 3068 Yes No Yes No If yes please Mail/Fax If Yes Please Mail/Fax Add Vehicle # Loan Eff. Date Loan Exp. Date Name of Loss Payee LP/GAR Mon. Day Yr. Mon. Day Yr. Loss Payee Change* Or Delete* Mortgagee *Mail/Fax Address of Loss Payee: Release Leased Vehicle # Leasing Company’s Name and Address (if different from L/P): Is Leasing Company the Owner or Vehicle Lessor of Vehicle Alternate Vehicle # Town of Garaging State of Garaging Zip Code Over 6 Months Reason Garaging MA Yes No Cover 1 & 2 Vehicle Coverage Limits Coverage Deductible Wavier Vehicle Coverage Limits Coverage Deductible Wavier Coverages # BI -- Collision -- Y N # BI -- Collision -- Y N and Misc. PIP -- Lim Col -- Y N PIP -- Lim Col -- Y N Changes UM1 -- Comp -- Y N UM1 -- Comp -- Y N Identify Model Model Vehicle and Year Prop Dam -- Rental 15 30 45 No Year Prop Dam -- Rental 15 30 45 No Give Change Opt Bi -- Tow 50 100 No Opt Bi -- Tow 50 100 No Medical -- UM2 -- Medical -- UM2 -- OP M/F Last Name First Name Initial Date of Birth License # State DATE 1ST DRVR PRIN DEFER EXCLUDED Drivers # LICENCED* Trng** OPER OPER OPER*** Operator Info Y VEH Y Y Y Must be N N N N Completed for Y Y Y Y VEH any Changes N N N N Y Y Y Y VEH or Operators N N N N YOUR FAILURE TO PROVIDE THE OPERATOR INFORMATION REQUESTED MAY RESULT IN THE CANCELLATION OF YOUR MOTOR VEHICLE INSURANCE. Is any listed operator also listed on any other Massachusetts auto policy or does any listed operator have a policy in His/Her own name? If so, give operator number and company name. Oper. # Company Oper. # Company Information on Vehicle(s) to be Insured. Please complete for Sub/Add. * Must be indicated for any operator under 25. 1. If Multicar discount applies please give class and CLASS Collision ** The operators have successfully completed a driver Collision coverage and other policy #: Coverage education course approved by the Massachusetts Registry of Motor Vehicles and hold a driver training 2. Is this vehicle customarily used in business? Yes No Yes No certificate, or have successfully completed a driver 3. Is this vehicle equipped with an anti-theft device? Attach certificate of installation. Yes No Yes No education course in another state, sponsored by a 4. Will the vehicle be used to transport passengers or students for a fee? Yes No Yes No recognized secondary school, college or university or other school approved by the state. Previous Carrier: *** Attach signed operator exclusion form. If this RPC is being electronically transmitted, the following must also be completed. I agree to be bound by this electronic record and it shall have the same legal force and effect as the written RPC. Applicants Name: Date: 2/14/2006 ERPC16 08/03 (If printed please sign on above line)