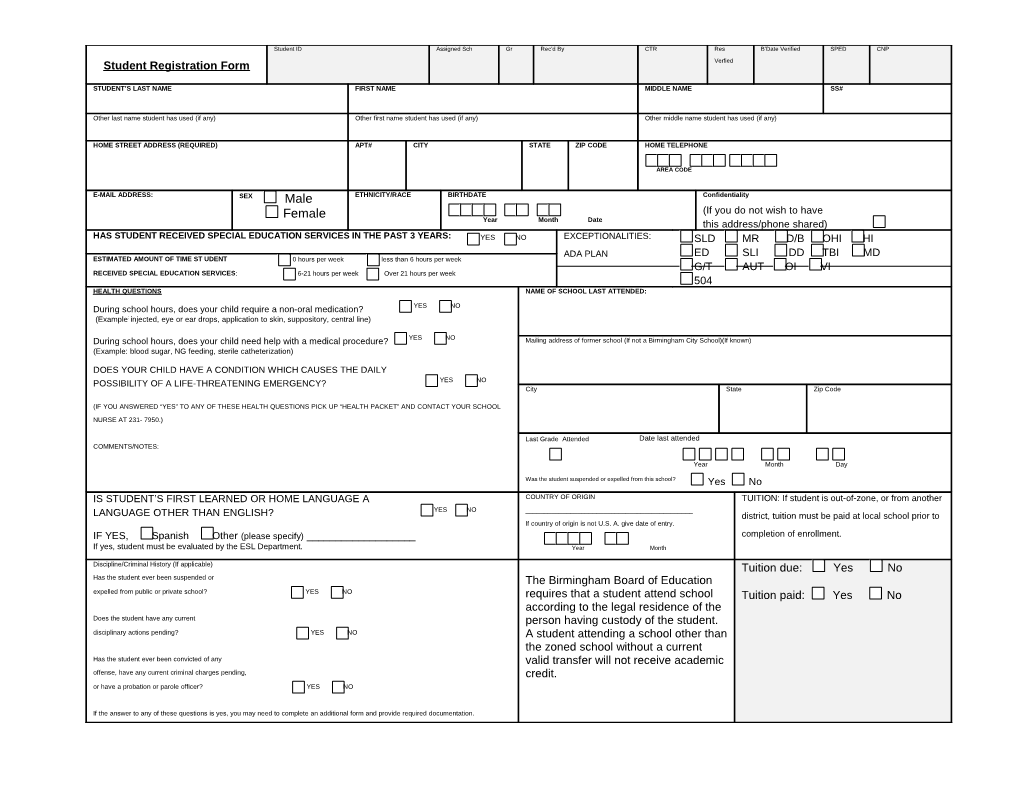
Student ID Assigned Sch Gr Rec’d By CTR Res B’Date Verified SPED CNP Student Registration Form Verfied
STUDENT’S LAST NAME FIRST NAME MIDDLE NAME SS#
Other last name student has used (if any) Other first name student has used (if any) Other middle name student has used (if any)
HOME STREET ADDRESS (REQUIRED) APT# CITY STATE ZIP CODE HOME TELEPHONE
AREA CODE
E-MAIL ADDRESS: SEX Male ETHNICITY/RACE BIRTHDATE Confidentiality Female (If you do not wish to have Year Month Date this address/phone shared) HAS STUDENT RECEIVED SPECIAL EDUCATION SERVICES IN THE PAST 3 YEARS: YES NO EXCEPTIONALITIES: SLD MR D/B OHI HI ADA PLAN ED SLI DD TBI MD ESTIMATED AMOUNT OF TIME ST UDENT 0 hours per week less than 6 hours per week G/T AUT OI VI RECEIVED SPECIAL EDUCATION SERVICES: 6-21 hours per week Over 21 hours per week 504 HEALTH QUESTIONS NAME OF SCHOOL LAST ATTENDED:
During school hours, does your child require a non-oral medication? YES NO (Example: injected, eye or ear drops, application to skin, suppository, central line)
During school hours, does your child need help with a medical procedure? YES NO Mailing address of former school (If not a Birmingham City School)(If known) (Example: blood sugar, NG feeding, sterile catheterization)
DOES YOUR CHILD HAVE A CONDITION WHICH CAUSES THE DAILY POSSIBILITY OF A LIFE-THREATENING EMERGENCY? YES NO City State Zip Code
(IF YOU ANSWERED “YES” TO ANY OF THESE HEALTH QUESTIONS PICK UP “HEALTH PACKET” AND CONTACT YOUR SCHOOL NURSE AT 231- 7950.)
Last Grade Attended Date last attended COMMENTS/NOTES: Year Month Day Was the student suspended or expelled from this school? Yes No IS STUDENT’S FIRST LEARNED OR HOME LANGUAGE A COUNTRY OF ORIGIN TUITION: If student is out-of-zone, or from another YES NO ______LANGUAGE OTHER THAN ENGLISH? district, tuition must be paid at local school prior to If country of origin is not U.S. A. give date of entry. IF YES, Spanish Other (please specify) ______completion of enrollment. If yes, student must be evaluated by the ESL Department. Year Month Discipline/Criminal History (If applicable) Tuition due: Yes No Has the student ever been suspended or The Birmingham Board of Education expelled from public or private school? YES NO requires that a student attend school Tuition paid: Yes No according to the legal residence of the Does the student have any current person having custody of the student. disciplinary actions pending? YES NO A student attending a school other than the zoned school without a current Has the student ever been convicted of any valid transfer will not receive academic offense, have any current criminal charges pending, credit. or have a probation or parole officer? YES NO
If the answer to any of these questions is yes, you may need to complete an additional form and provide required documentation. STUDENT’S LAST NAME FIRST NAME MI STUDENT’S SS# ID
1 LAST NAME FIRST NAME EMERGENCY CONTACT #1 #
______n
a Last Name First Name i RELATIONSHIP TO STUDENT d
r ______
a Daytime Phone Relationship to Student
u ADDRESS EMERGENCY CONTACT #2 G /
t ______n Last Name First Name e r
a ______(THE PERSON LISTED AS PARENT/GUARDIAN #1 MUST HAVE THE SAME ADDRESS AS THE STUDENTS’ HOME ADDRESS AS SHOWN ON PAGE 1.) P Daytime Phone Relationship to Student HOME PHONE Check here if unlisted. CELL PHONE PHYSICIAN/HEALTH CARE PROVIDER PHONE
EMPLOYER WORK PHONE (INCLUDE AREA CODE) EXT. *WHO HAS LEGAL CUSTODY STUDENT LIVES WITH(CHECK ONE BOX) OF THIS STUDENT? (CHECK ONE BOX) Both Parents
2 LAST NAME FIRST NAME
Both Parents
# Father
n RELATIONSHIP TO STUDENT Mother a
i Mother
d Father r
a Guardian(s)
u ADDRESS Guardian(s)
G Grandparent (s) / t Ward of Court n
e Agency/Social Service r Grandparent (s) a Foster Parent(s) P HOME PHONE Check here if unlisted. CELL PHONE Independent Spouse/Partner Parenting Plan EMPLOYER WORK PHONE EXT. (INCLUDE AREA CODE) (Shared custody) Alone
Other Relative(s) *Copy of Court documents may be required.
3 LAST NAME FIRST NAME TRANSPORTATION INFORMATION:
#
n RELATIONSHIP TO STUDENT STUDENT RIDES A BUS YES a i NO d r a
u ADDRESS STUDENT RIDES A DAY CARE VAN YES LIST DAY CARE NAME AND NUMBER. G /
t NO n IS A BUS/CAR RIDER ONLY IN INCLEMENT YES e r
a WEATHER NO P HOME PHONE Check here if unlisted. CELL PHONE WALKS HOME YES NO
EMPLOYER WORK PHONE (INCLUDE AREA CODE) EXT. IS A CAR RIDER YES NO
BIRMINGHAM CITY SCHOOLS CERTIFICATION OF RESIDENCE FOR THE SCHOOL YEAR 2012-13
Date: ______School: ______
To The Birmingham Board of Education:
I, ______Circle Correct Title “Parent-Legal Guardian - Person Having Legal Custody”
Of the school children names below, I am a bona fide resident of the City of Birmingham with residence located at
______Zip Code Telephone Number
I have resided at this address since ______
My residence is at this address, and I have no other in the city. Yes ______No ______
The children listed below reside with me at this address. Yes ______I will notify the school when my address changes. Yes ______
Name of the children enrolled in school Race Sex Grade Level (2012-13) (Please Print)
1.______
2.______
3.______
4.______
Name of children “not” enrolled in school (Please Print) 1.______
2.______
3.______
4.______
______Date Signature of Parent, Legal Guardian or Person Having Legal Custody
The Birmingham Board of Education requires that a student attend school according to her/his legal residence. MEDIA RELEASE PERMISSION
Student ______Grade ______
School ______
I hereby give the Birmingham City Schools the right and permission to publish/use photographs or video and/or audiotapes of my child, a student registered in a Birmingham City School.
I understand that such reproductions could be used to publicize/promote the school district though its own media productions or through the commercial media.
I waive any right to inspect and/or approve the finished product and do release the Birmingham City Schools from any liability by virtue of distortion by processing. I further agree that items these may be used for publication, broadcast, or reproduction without limitation, or reservation or any fee.
In addition, I accept responsibility, knowing that this release form is on file, to have it removed when and if I deem it disadvantageous or inadvisable to have my child featured in such a manner. (If you prefer your child not be involved in these types of activities, we will respect your wishes.)
YES______NO ______
Parent signature ______
Date ______BIRMINGHAM CITY SCHOOLS
Home Language Survey
Student' name:______Date:______
Age:______Date of birth______Last grade attended:______
Parent's name:______Country of origin:______
What was the student's language at infancy?______Language used to
communicate now?______Language spoken at home?______
Student can read in the following languages:______
Parents can read in the following languages:______Student's signature (If in grades 9-12) Parent/guardian’s signature
Encuesta del lenguaje materno
Nombre del/a estudiante______Fecha______
Edad______Fecha de nacimiento______Año escolar______
Nombre del padre______Nombre de la madre______País de
origen______Idioma de la infancia______Idioma que el/la
estudiante usa más frecuentemente______Idioma hablado en
casa______El/la estudiante lee, habla y escribe en los siguientes idiomas ______
Los padres leen, hablan y escriben en los siguientes idiomas______
______Firma de/la estudiante (Si están en grados 9-12) Firma de los padres
SIGNED COPY MUST BE RETAINED IN STUDENT'S CUM FOLDER, IF ANOTHER LANGUAGE IS INDICATED ANYWHERE, PLEASE CALL MAGALY MONZON, 231-7954 FOR TESTING. Birmingham City Schools (STUDENT RESIDENCY QUESIONNAIRE)
BCS School Name: ______2012-2013 School Year PLEASE COMPLETE ONE (1) FORM FOR EACH STUDENT BEING ENROLLED
Student Name: Male Female Birth Date: / / (mm/dd/yy)
Social Security #:
Current Address: (Include City, State and Zip) Telephone #:
Previous Address: (Include City, State and Zip) Cell #:
Last School Attended: Last Date Attended: Current Grade Level:
Name of Parents/Guardians: (Please Print)
Signature of Parent/Guardian: Date:
I hereby attest that the information above is true and correct and I understand that if i falsely enroll the student named above in a school not in his/her proper attendance zone, the student may be denied any credit for school work completed while improperly attending the out-of-district school.
This questionnaire is intended to address the McKinney-Vento Homeless Education Assistance Improvement Act 42 U.S.C. 11435. The answers to this questionnaire will help school system personnel determine if the student qualifies for additional services. 1. Is someone else other than you listed as the primary owner/renter of the above address (i.e. you are not listed IN/ON the lease agreement)? □ YES □ NO 2. Is your current housing situation temporary and/or unstable (i.e. you plan to move within the next 6 months, living in hotel/motel, living in transitional housing, etc.)? □ YES □ NO 3. Is your current living situation due to an eviction, house fire, domestic violence, financial hardship, etc.? □ YES □ NO 4. Are you enrolling a student for whom you DO NOT have legal custody and/or have received an Emergency Permission to Enroll? □ YES □ NO 5. Are you a high school student, NOT living with either parent, enrolling yourself in school? □ YES □ NO *If you answered “YES” to (1) one or more of the above questions, please complete the next section* **If you answered “NO” to ALL of the above questions, please return to school personnel** The student lives in the following situation (please check one):
TS1 Shelter/Transitional Housing Program (i.e. Penelope House, Salvation Army Women’s Shelter, Family Promise/IHN, Alabama Baptist Children’s Home, Housing First Transitional/Disability Housing, Wilmer Hall, St.Mary’s Children’s/Transitional Home, Catholic Social Services Disability Housing, etc.) TS2 Doubled-Up (living with family/friends on a temporary basis) Please provide the name of the homeowner/renter: ______ TS3 Unsheltered (i.e. cars, parks, campgrounds, etc.) TS4 Hotel/Motel (includes regular hotels/motels and pay-by-the week motels/apartments) TS5 Unaccompanied Youth (unable to locate parents, parents are incarcerated, military parents, DHR removal etc.) TS6 Other______SCHOOL USE ONLY
Homeless Liaison determination of student: Student and parent live with another family – NOT homeless Student qualifies as homeless under the McKinney-Vento Act Signature of Homeless Liaison: Date: Comments:
*Keep original at school in separate file – Do NOT put in cumulative folder!!! *Send copy of all “Yes” questionnaires to Josephine Hollins, Fax: 231-7616 and for questions please call 231-7938. Birmingham City Schools, May 2010 ALABAMA STATE DEPARTMENT OF EDUCATION EMPLOYMENT SURVEY
SCHOOL SYSTEM: BIMRINGHAM CITY SCHOOLS/0114 SCHOOL YEAR : _____
SCHOOL: ______GRADE: ______
Dear Parents or Guardians; Please, complete the following survey. The results of this survey will be used to determine if you are possibly eligible for the Migrant Education Program. Student Name: ______Name of Parent or Guardian: ______Address: ______Telephone Number: ______
1. Have you moved during the last 3 years to work or to seek work even if it was for a short period of time? YES _____ NO ______2. Are you or your spouse working or have you worked in an activity directly related to some of the following? Please, check (√) all applicable:
The production or process of harvests, milk products, poultry farms, poultry plants, cattle farms. Fruit farms The cultivation or cutting of trees Work in nurseries or sod farms Fish or shrimp farms Worm farms Catching or processing sea food (shrimp, oysters, crabs, fish, etc…) 3. From what city, state or country did you come from? ______4. What type of work did you or your spouse do before coming here? ______Revised 6/1/08 V.2
ATTENTION SCHOOL PERSONNEL SEND COMPLETED SURVEYS TO THE ATTENDANCE DEPARTMENT AT THE END OF EACH MON Important Notice to Parents
Assisting a student with prescribed medication during the school day enables the student to remain in school, to maintain or improve health, and improve potential for learning. Students will receive medication only as prescribed by a licensed physician.
Beginning in the 2004-2005 school year schools must meet certain standards when giving medication during school hours. The following regulations and procedures will be strictly followed. Schools will be periodically audited to ensure compliance.
Parents are to give any morning dose of medication before sending child to school. If your child has breakfast at school, you can give medication with crackers or give 30 minutes before arrival at school.
All proper forms must be on file in the office with the doctor and parent signatures. Original signatures are required. We can no longer accept faxed copies.
Medication must be in the original prescription bottle/box when delivered to the school office. Medication must be brought to the office by an adult. Medication will be counted and verified with a signature at the time of delivery.
If your child is taking oral medication we encourage you to supply water cups and a calibrated measuring device such as a measuring tube or medication cups.
If your child is starting a new medication, we encourage you to give the first dose at home. This will allow you to observe any adverse reactions.
No medication will be given before or after school. We hope that with this advanced notification that you will begin making preparations before school starts to be in compliance.
As always, the health and safety of the children is our chief concern. Thank you for your cooperation.
Respectfully,
______Principal School Nurse
Student Anti-Harassment / Anti-Violence Reporting Form
There are forms available in every school to report alleged bullying, harassment, or intimidation that occurred on school property; at a school-sponsored activity or event off school property; on a school bus; or on the way to and/or from schoolin the current school year. Bullying, harassment, or intimidation are serious and will not be tolerated.
Bullying, harassment, or intimidation means intentional conduct, including verbal, physical, or written conduct, or an intentional electronic communication, that creates a hostile educational environmentby substantially interfering with a student’s educational benefits, opportunities, or performance, or with a student’s physical or psychological well-being and is:
motivated by an actual or a perceived personal characteristic including race, national origin, marital status, gender, gender orientation, gender identity, religion, ancestry, physical attribute, socioeconomic status, familial status, or physical or mental ability or disability; or threatening or seriously intimidating and occurs on school property, at a school activity or event, or on a school bus; or substantially disrupts the orderly operation of a school.
Electronic communication means a communication transmitted by means of an electronic device, including a telephone, cellular phone, computer, or pager. State of Alabama Department of Education Health Assessment Record School Year: 2012-2013
To Parent or Guardian: The purpose of this form is to provide the school nurse with additional information regarding your child’s health needs. The school nurse may contact you for further information. The information requested is essential for the school nurse to meet the health needs of your child. This information will be kept strictly confidential. To be completed by parent/guardian. PLEASE PRINT. Return to the School Nurse. Name of Student (Last, First, Middle) Birth Date Sex
Address (Street) Race/Ethnicity □ American Indian □ White, not of Hispanic origin (City and Zip code) □ Asian □ Hispanic/Latino □ Black, not of Hispanic origin □ Other Home Telephone Number Cell Telephone Number School Grade
Name of Parent/Guardian (Last, First, Middle)
Transportation □ Bus Rider □ Car Rider □ Special Needs Bus □ After School Program Part I – Health Information Place where your child receives regular Place where your child receives regular Type of Insurance health care: dental care: your child has:
□ Health Department □ Health Department □ Medicaid □ Hospital Clinic □ Hospital Clinic □ No Insurance □ Community Health Center □ Community Health Center □ Private Insurance □ Private Doctor/HMO □ Private Doctor/HMO □ ALLKIDS □ Other ______□ Other ______□ Other: ______□ No regular place □ No regular place
Physician’s Name:______Dentist’s Name: ______
Address: ______Address: ______
______
Tel: ______Tel: ______
Authorizations: □ I authorize the school nurse, the registered nurse (RN) or licensed practical nurse (LPN), to talk with the physician(s) should a question come up about my child’s medical conditions.
□ I do NOT authorize the school nurse, the RN or LPN, to talk with the physician(s) should a question come up about my child’s medical conditions.
□ I authorize for my child to participate in all school health screenings, such as vision, hearing and scoliosis.
□ I authorize the yearly review of my child’s Certificate of Immunization (Blue Slip) by the local Public Health Department.
FOR OFFICE USE ONLY Acuity Scale: Level A Level B Level C Level D Nursing Dependent Medically Fragile Medically Complex Health Concerns
Page 1 SHR 1/2011 v.3 State of Alabama Department of Education Health Assessment Record School Year: 2012-2013
Part II – Medical History □ NO KNOWN HEALTH PROBLEMS ( If no, please go directly to the bottom of the page and provide parent/guardian signature.) □ Attention Deficit Disorder (ADD) □ Requires medication? (Requires medication authorization from physician) OR □ Attention Deficit Hyperactivity Disorder (ADHD) □ To be given while at school? □ Allergies: Please Specify : □ Hives/rash? □ Food ______□ Insects ______□ Breathing difficulty? □ Environmental ______□ Medications ______□ Epi-pen? (Requires medication authorization from physician) □ Asthma: □ He/She uses an inhaler at school?(Requires authorization from physician) □ He/She uses an inhaler at home? □ Bleeding Problems: □ Requires medication? Please explain: (Hemophilia, Von Willebrand’s, frequent nosebleeds) (Requires medication authorization from physician) □ Cancer/Leukemia: Please explain: □ Cerebral Palsy: Please explain: □ Cystic Fibrosis: Please explain: □ Dental Problems: □ Braces? OR Please explain: □ Diabetes:(Requires medication and procedure authorization from physician) □ Monitors Blood Sugars while at school? □ Type 1 Diabetic □ Requires Insulin at school? □ Glucagon order? □ Type 2 Diabetic □ Insulin pump? □ Managed with diet? □ Emotional/Behavioral/Psychological: Please explain: □ Gastrointestinal/Stomach Problems: Please explain: □ Genetic Disorder: Please explain: □ Headaches: Please explain: □ Hearing Problems: □ Right Ear □ Left Ear □ Both ears □ Tubes □ Hearing loss? □ Hearing aid? □ Cochlear Implant □ Heart Condition: Please explain: Are there any activity restrictions? Any medications taken at home only?
□ Hypertension (High Blood Pressure): □ Juvenile Arthritis/Bone-Joint Problems: Please explain: □ Kidney Problems: Please explain: □ Scoliosis: □ No Treatment □ Wears Brace □ Surgery □ Seizures/Convulsions: Please explain: Type of seizure: ______□ Diastat order □ Sickle Cell Anemia: □ Spina Bifida: □ Special Diet: Please explain: □ Vision Problems: □ Wears glasses □ Wears contacts □ Other, ______□ Other Medical Conditions: Please include any medications taken at home only.
Part III – Medical Equipment /Procedures Required at School □ Catheter □ Gastric Tube □ Nebulizer Treatments □ Oxygen Supplement □ Tracheostomy □ Vagal Nerve Stimulator (VNS) □ Ventilator □ Wheelchair □ Walker Required Signatures
Signature of parent(s) or guardian:______Date:______
Signature of school nurse: ______Date:______
Page 2 SHR 1/2011 v.3