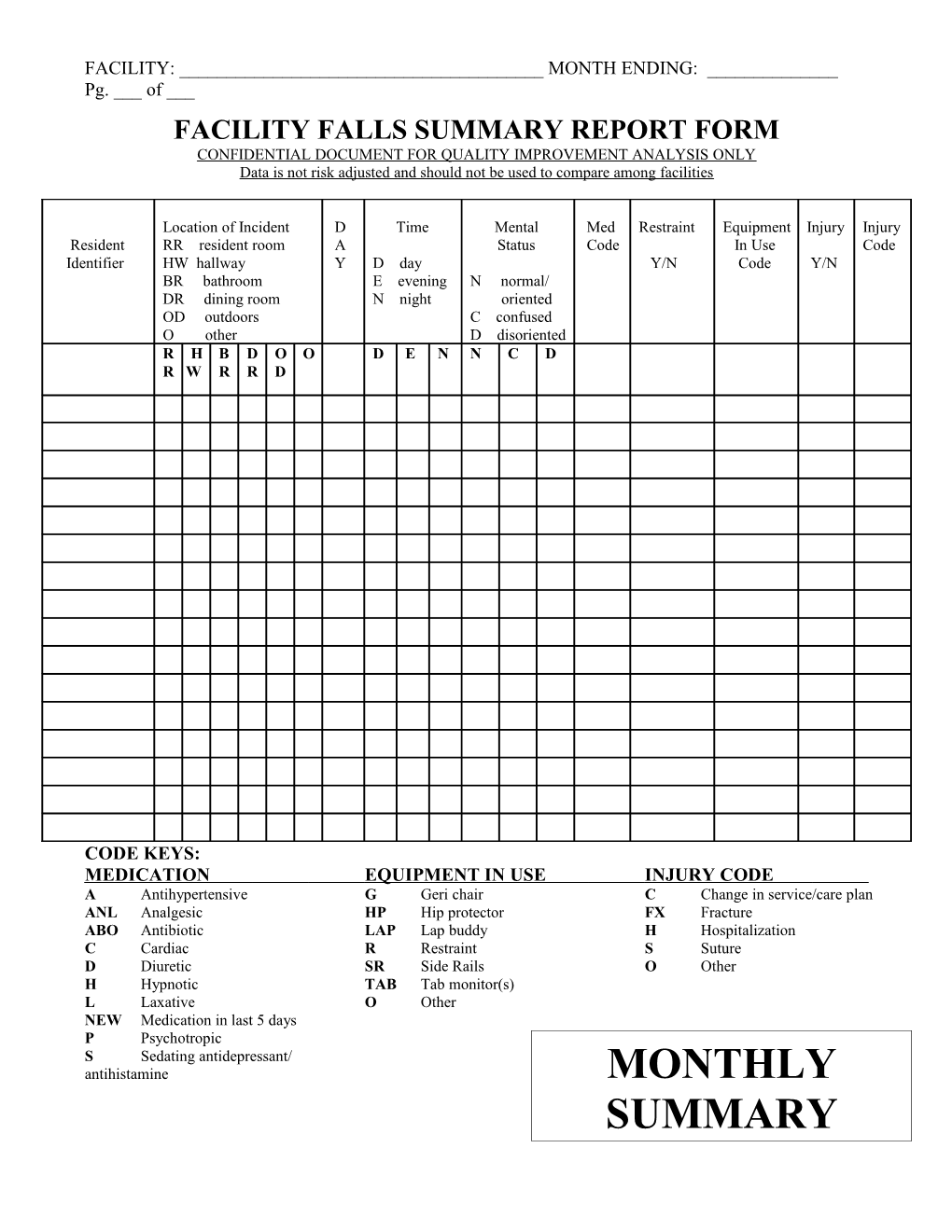
FACILITY: ______MONTH ENDING: ______Pg. ___ of ___ FACILITY FALLS SUMMARY REPORT FORM CONFIDENTIAL DOCUMENT FOR QUALITY IMPROVEMENT ANALYSIS ONLY Data is not risk adjusted and should not be used to compare among facilities
Location of Incident D Time Mental Med Restraint Equipment Injury Injury Resident RR resident room A Status Code In Use Code Identifier HW hallway Y D day Y/N Code Y/N BR bathroom E evening N normal/ DR dining room N night oriented OD outdoors C confused O other D disoriented R H B D O O D E N N C D R W R R D
CODE KEYS: MEDICATION EQUIPMENT IN USE INJURY CODE A Antihypertensive G Geri chair C Change in service/care plan ANL Analgesic HP Hip protector FX Fracture ABO Antibiotic LAP Lap buddy H Hospitalization C Cardiac R Restraint S Suture D Diuretic SR Side Rails O Other H Hypnotic TAB Tab monitor(s) L Laxative O Other NEW Medication in last 5 days P Psychotropic S Sedating antidepressant/ antihistamine MONTHLY SUMMARY FACILITY: ______MONTH ENDING: ______Pg. ___ of ___ FACILITY FALLS DATA SUMMARY CONFIDENTIAL DOCUMENT FOR QUALITY IMPROVEMENT ANALYSIS ONLY Data is not risk adjusted and should not be used to compare among facilities
1. Total number of falls …………………………………………………………………………………………………………….
2. Total number of falls with injury ……………………………………………………………………………………..
3. Total number of residents who fell ………………………………………………………………………………….
4. Total number of residents with two or more falls ……………………………………………………….
5. Total number of falls per resident computed only for residents who fell: …………….. (#1 above divided by #3 above)
6. For the month, total resident days: ………………………………………………………………………………..
(average daily census x number of days in this month)
7. Falls per 1,000 resident days: ………………………………………………………………………………………….. (#1 above x 1,000, divided by #6 above)
8. Falls with injury per 1,000 resident days: ……………………………………………………………………..
(#2 above x 1,000, divided by #6 above) FACILITY: ______MONTH ENDING: ______Pg. ___ of ___
Note: For the purposes of this report, “injury” means any fracture, any sutures, any need for hospitalization or other immediate medical attention, and any changes in functional ability requiring a change in the service/care plan. Injury does not include minor skin tears or bruises.