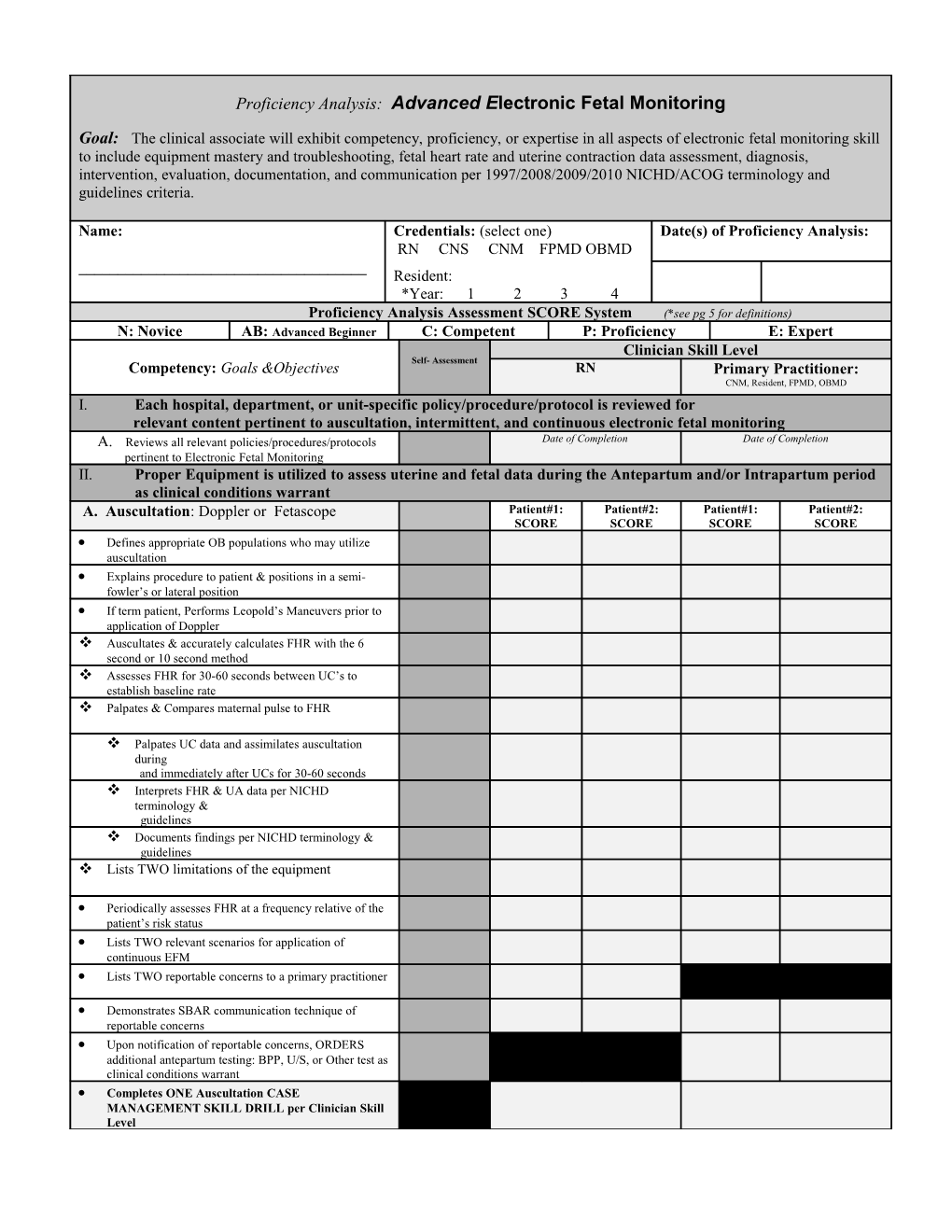
Proficiency Analysis: Advanced Electronic Fetal Monitoring
Goal: The clinical associate will exhibit competency, proficiency, or expertise in all aspects of electronic fetal monitoring skill to include equipment mastery and troubleshooting, fetal heart rate and uterine contraction data assessment, diagnosis, intervention, evaluation, documentation, and communication per 1997/2008/2009/2010 NICHD/ACOG terminology and guidelines criteria.
Name: Credentials: (select one) Date(s) of Proficiency Analysis: RN CNS CNM FPMD OBMD ______Resident: *Year: 1 2 3 4 Proficiency Analysis Assessment SCORE System (*see pg 5 for definitions) N: Novice AB: Advanced Beginner C: Competent P: Proficiency E: Expert Clinician Skill Level Self- Assessment Competency: Goals &Objectives RN Primary Practitioner: CNM, Resident, FPMD, OBMD I. Each hospital, department, or unit-specific policy/procedure/protocol is reviewed for relevant content pertinent to auscultation, intermittent, and continuous electronic fetal monitoring A. Reviews all relevant policies/procedures/protocols Date of Completion Date of Completion pertinent to Electronic Fetal Monitoring II. Proper Equipment is utilized to assess uterine and fetal data during the Antepartum and/or Intrapartum period as clinical conditions warrant A. Auscultation: Doppler or Fetascope Patient#1: Patient#2: Patient#1: Patient#2: SCORE SCORE SCORE SCORE Defines appropriate OB populations who may utilize auscultation Explains procedure to patient & positions in a semi- fowler’s or lateral position If term patient, Performs Leopold’s Maneuvers prior to application of Doppler Auscultates & accurately calculates FHR with the 6 second or 10 second method Assesses FHR for 30-60 seconds between UC’s to establish baseline rate Palpates & Compares maternal pulse to FHR
Palpates UC data and assimilates auscultation during and immediately after UCs for 30-60 seconds Interprets FHR & UA data per NICHD terminology & guidelines Documents findings per NICHD terminology & guidelines Lists TWO limitations of the equipment
Periodically assesses FHR at a frequency relative of the patient’s risk status Lists TWO relevant scenarios for application of continuous EFM Lists TWO reportable concerns to a primary practitioner
Demonstrates SBAR communication technique of reportable concerns Upon notification of reportable concerns, ORDERS additional antepartum testing: BPP, U/S, or Other test as clinical conditions warrant Completes ONE Auscultation CASE MANAGEMENT SKILL DRILL per Clinician Skill Level 2
Objective must be performed on a LIVE patient
Clinical Competency Analysis: Advanced Electronic Fetal Monitoring
Copyright © 2014.LAMMICO.All Rights Reserved. Clinician Skill Level
Competency: Goals &Objectives Self- Assessment RN Primary Practitioner: CNM, Resident, FPMD, OBMD B. Electronic Fetal Monitor: (Make & Model: ______) 1. Test Button Locates & Explains implications for use Runs a TEST & Interprets results correctly Outlines proper procedure for abnormal TEST results 2. Mark Button Locates & Explains implications for use 3. Time/Date/Clock Locate & Demonstrates how to adjust settings 4. Logic/Artifact Eliminator/ECG Disabled Locates & Demonstrates how to adjust settings List TWO Fetal clinical conditions necessitating disabling the button (extreme rate abnormalities or dysrhythmias) 5. Tocodynamometer Explains how equipment collects & interprets data Locates point of maximum intensity & Palpates UC’s & resting tone prior to placement Demonstrates how to adjust & reset baseline Identifies proper cleaning and storage 6. External Ultrasound Explains how equipment collects & interprets data Demonstrates proper connection to monitor & placement on patient for quality data collection If term patient, Performs Leopold’s Maneuvers prior to application & places device over point of maximum intensity Demonstrates how to improve channel quality Palpates & Compares maternal pulse to FHR Identifies proper cleaning and storage 7. Fetal Electrocardiogram (FECG) Explains how equipment collects & interprets data Identifies indications/contraindications to placing the FECG Demonstrates proper application of the FECG Demonstrates proper connection to monitor LISTS TWO troubleshooting techniques to improve data collection & quality 8. Intrauterine Pressure Catheter (IUPC) Explains how equipment collects & interprets data Identifies indications/contraindications to placing the IUPC Demonstrates proper application of the IUPC (*RN Approval for application varies per State Licensure guidelines) Demonstrates proper connection to monitor 3 Demonstrates how to zero transducer Performs periodic palpation to validate data collected LISTS TWO troubleshooting techniques to improve data collection & quality
Clinical CompetencyCopyright Analysis: © 2014.LAMMICO.All Advanced Rights Electronic Reserved. Fetal Monitoring
Clinician Skill Level Competency: Goals &Objectives Self- Assessment RN Primary Practitioner: CNM, Resident, FPMD, OBMD III. Each clinician will identify, intervene, evaluate, categorize, document, and communicate all reassuring and nonreassuring FHR and UA data per NICHD guidelines and terminology A. RISK Assessment & Interpretation Defines AWHONN/ACOG standards for evaluation of FHR & UA data during latent phase, active phase, and second stage of the LOW & HIGH RISK PATIENT B. Uterine Contraction Analysis Identifies UA data for frequency, intensity, duration, & resting tone at fundal point of maximum intensity & at appropriate intervals per patient risk status Promptly Identifies causation of nonreassuring/abnormal findings (ie: tachysystole, hypertonus, polysystole, tentanic etc) Intervenes initially with the least invasive methods to improve maternal, fetal, and uterine conditions if nonreassuring findings persist Evaluates resolution of nonreassuring findings & alters plan of care accordingly C. FHR Analysis(Baseline: FHRB & Variability: FHRV) Identifies ALL FOUR Characteristics of a Normal/Healthy FHR pattern Identifies FHR data for FHRB, normal range, exclusion criteria, and segment criteria per NICHD guidelines Promptly Identifies causation of nonreassuring/abnormal FHRB findings (ie: tachycardia, bradycardia, dysrhythmias, or sinusoidal pattern) Identifies FHR data for FHRV per NICHD guidelines (absent, minimal, moderate, marked) Promptly Identifies causation of nonreassuring/abnormal FHRV findings (ie: absent, minimal, or marked) Intervenes initially with the least invasive methods to improve maternal, fetal, and uterine conditions if nonreassuring findings persist Evaluates resolution of nonreassuring findings & alters plan of care accordingly D. Periodic or Episodic Pattern Analysis Define the term Periodic, Episodic, Abrupt, Gradual, intermittent, & recurrent per NICHD criteria Identifies FHR data for ACCELERATIONS per gestational age requirements as outlined in NICHD guidelines Identifies FHR data for EACH DECELERATION per NICHD guidelines
Promptly Identifies causation of nonreassuring/abnormal PERIODIC OR EPISODIC findings (ie: recurrent late, variable, or prolonged decelerations, intermittent or recurrent severe late or variable decelerations) Intervenes initially with the least invasive methods to improve maternal, fetal, and uterine conditions if nonreassuring findings persist Evaluates resolution of nonreassuring findings & alters plan of care accordingly E. NICHD Three Tier FHR Interpretation System Categorize FHR Patterns according to new NICHD System F. EVOLUTION Evaluates Evolution of the FHR/UA Data Periodically at Patient Hand-off, Rounds, or Shift Report G. COMMUNICATION Demonstrates SBAR communication technique of reportable concerns
If Delay or NO Response from Clinician, communicates reportable concerns to administrative leadership in a timely manner 4 H. DOCUMENTATION Documents FHR/UA data in an objective & concise format via electronic or paper technique Documents FHR/ UA data periodically per protocol using NICHD terminology & categorization with supplemental terminology as outlined in additional references as indicated Completes TWO EFM SKILLS ANALYSIS ALGORITHMS per Clinician Skill Level
Clinical CompetencyCopyright Analysis: © 2014.LAMMICO.All Advanced E Rightslectronic Reserved. Fetal Monitoring
Goal: The clinical associate will exhibit competency, proficiency, or expertise in all aspects of electronic fetal monitoring skill to include equipment mastery and troubleshooting, fetal heart rate and uterine contraction data assessment, diagnosis, intervention, evaluation, documentation, and communication per 1997/2008/2009/2010 NICHD/ACOG terminology and guidelines criteria. Clinical Skill Level Competency: Goals &Objectives Primary RN Practitioner CNM, Resident, FPMD, OBMD IV. Each clinician will perform non-electronic & electronic fetal monitoring skill at a level of competency, proficiency, or expert prior to independent patient care
Final Cumulative Score: N AB C P E
Recommended for Remediation o NO o NO o YES o YES If YES, Remediation Action Plan for Improved Performance includes: (select all that apply) Instructional Methods: Methods of Evaluation: o (DT) Didactic Teaching w/ resources o (SA) Self Assessment o (PP) Policy/Procedure/Protocol Review o (PO) Preceptor Observation o (SLM) Self-Learning Module o (AP0) Advanced Practice Observation (NP, CNM, MD) o (T/P) Textbooks or Periodicals o (SC) Skills Checklist o (PCL) Patient Care Literature o (RD) Return Demonstration o (CS) Case Study Analysis/Presentation o (CA) Chart Audit o (CT) Computer Tutorials o (PR) Peer Review (PT) Post Testing o (VID) Video Tapes o o (AUD) Audio Tapes o (DEM) Demonstration
IF YES, Date for Reassessment of Skills Recommended for Annual Reassessment o NO o NO o YES o YES I am qualified clinician with PROFICIENT skill & knowledge regarding non-electronic & Instructor Credentials: (select one) electronic fetal monitoring assessment techniques, NICHD terminology & guidelines, and current evidence-based literature supporting additional terminology and management RN CNS CNM FPMD OBMD options regarding nonreassuring findings. To the best of my ability and without assistance Resident: to the clinician, I have evaluated their skill in advanced EFM. *Year: 1 2 3 4 Proficiency Analysis Instructor: ______
Clinician Electronic Signature: ______5 Final Competency Assessment Score: This area will be an ongoing assessment until the clinical associate demonstrates a level of “C for Competent” or greater. All clinical associates must meet a level of “C for competent” or greater to perform as an unsupervised individual practitioner within the unit.
Novice: A beginner (New graduate or New skill) with minimal practical skills & the inability to apply theory into practice; dependent on constant direct supervision. Independent patient care inappropriate & unsafe.
Advanced Beginner: Exhibits a basic knowledge with practical experience regarding routine or stable patients; lacks organization and needs support in priority setting; independent with routine care but dependent with advanced EFM skills and/or techniques. Needs supervision until consistent.
Competent: Functions completely independent with stable or routine EFM patients yet continues to expend excess energy when making decisions in complex patient situations; independent yet seeks unit expert with complex EFM scenarios.
Proficient: Functions independently in both routine and complex EFM clinical situations. May act as a preceptor and/or instructor for EFM skills.
Expert: Exhibits a highly evolved understanding of EFM theory and knowledge and offers exceptional clinical expertise in all complex clinical situations.
Resources: Copyright © 2014.LAMMICO.All Rights Reserved.
1. American Academy of Pediatrics and American College of Obstetricians and Gynecologists (2007).Guidelines for Perinatal Care, 6th ed.): Elk Grove Village, IL: Author.
2. American College of Obstetricians and Gynecologists (ACOG). (2010/2013). Management of Intrapartum Fetal Heart Rate Tracings Surveillance (Practice Bulletin #116). Washington, DC: Author.
3. ACOG. (2009/2013). Intrapartum fetal heart rate monitoring: Nomenclature, interpretation, and general management principles (Practice Bulletin #106). Washington DC: Author.
4. AWHONN. (2008). Fetal Heart Monitoring (Position Statement). Washington, DC: Author.
5. AWHONN. (2004). Amniotomy and Placement of Internal Fetal Spiral Electrode through Intact Membranes (Clinical Position Statement). Washington, DC: Author.
6. AWHONN. (1998). Competence Validation for Perinatal Care Providers: Orientation, Continuing Education, and Evaluation. Philadelphia PA: Lippincott.
7. Curran, C., & Torgersen, K. (2006). abcdEFM: The TEXTBook, Electronic Fetal Monitoring. Virginia Beach, VA: Clinical Specialists Consulting, Inc.
8. Feinstein, N.F., Sprague, A. & Trepanier, M.J. (2008). Fetal Heart Rate Auscultation (2nd ed.). Washington DC: Author.
9. Freeman, R, Garite, T, & Nageotte, M. (2003). Fetal Heart Rate Monitoring (3rd Ed). Philadelphia, PA: Lippincott, Williams, & Wilkins.
10. Lyndon, A., & Ali, L. U. (Eds.). (2009). Fetal Heart Monitoring: Principles and Practices (4th Ed.). Dubuque, IA: Kendall Hunt Publishing.
11. Macones, G. A., Hankins, G. D., Spong, C. Y., Hauth, J., & Moore, T. (2008). The 2008 National Institute of Child Health and Human Development Workshop Report on Electronic Fetal Monitoring: Update on definitions, interpretation, and research guidelines. Obstet & Gynecol ; 112(3):pp. 661-666.
12. Menihan, CA, & Zottoli, EK. (2007). Electronic Fetal Monitoring: Concepts and Applications (2nd Ed). Philadelphia PA: Lippincott, Williams, & Wilkins. 6 13. National Institute of Child Health and Human Development (NICHD) Research Planning Workshop. (1997). Electronic fetal heart rate monitoring: Research guidelines for interpretation. Am J Obstet Gynecol, 177(6):1385-1390, and J Obstet Gynecol Neonat Nurs, 26(6): 635-640.
Copyright © 2014.LAMMICO.All Rights Reserved.