DIETARY INTERVENTION FOCUSED ON PHOSPHATE INTAKE IN HEMODIALYSIS PATIENTS WITH HYPERPHOSPHOREMIA
INTRODUCTION.
Elevated serum phosphorus levels in chronic kidney disease (CKD) dialysis- treated patients have been associated with skeletal alterations and cardiovascular mortality1,2,3. Mineral metabolism control has proven effective in lowering mortality4,5. For this reason, the NKF-K/DOQI practice guidelines recommend a good control of serum phosphorus (3,5–5.5 mg/dl), calcium (8.4–9.5 mg/dl), Ca x P product (<55 mg2/dl2) and intact parathyroid hormone (PTHi) levels (150-300 pg/ml) in hemodialysis patients6.
Hemodialysis and phosphate binders have a limited efficacy to reduce serum phosphorus. Furthermore, the use or calcium- or aluminum-based phosphate binders is limited by the adverse effects of hypercalcemia or aluminum toxicity in long-term hemodialysis. Novel phosphate binders (sevelamer, lanthanum carbonate) have also efficacy- and tolerance-related problems. Therefore, only a limited number of patients accomplish the proposed NF-K/DOQI bone metabolism guidelines7,8.
Thus, dietary restriction of phosphorus is a fundamental pillar in the control of phosphorus levels. However, achieving this restriction is difficult because it requires a significant patient understanding and collaboration and may create a conflict with protein requirements in dialysis patients9.
We hypothesized that intensive dietary intervention addressing hemodialysis patients could significantly reduce phosphorus intake, improve mineral metabolism and increase the number of patients who achieve the proposed NKF-K/DOQI bone metabolism guidelines.
2 MATERIALS AND METHODS
Design. This work is a 6-month experimental study. Patients were allocated to either an experimental group with intensive dietary education or a control group with the usual dietary recommendations. Initially allocation was intended in accordance with their hemodialysis unit (group-randomized clinical trial). This form of allocation was elected to avoid a bias resulting from informative contamination between both groups (the exchange of information between patients of the same dialysis unit and shift allocated to different interventions). However, the imbalance in the number of patients made also necessary the allocation of the San Juan de Dios Hospital patients in accordance with their hemodialysis shift (figure 1). The Ethics Committees of the participating hospitals approved the study. Informed consent for inclusion was signed by all the patients.
Study population. This study was performed in the Hemodialysis Units of the Miguel Servet University Hospital, the Clinic University Hospital, the San Juan de Dios Hospital and the Military Hospital (Zaragoza, Spain) and the Regional Alcañiz Hospital (Teruel, Spain).
Inclusion criteria: 1.- Age > 18 years old. 2.- Receiving hemodialysis treatment for > 6 months, without clinical complications (free of acute illness) and correct dialysis parameters (Kt/V>1.2). 3.- Absence of feeding difficulties and normal appetite, assessed by a dietary survey previously validated by our group10. 4.- Previous 3-month average serum phosphorus > 5.5 mg/dl or Ca x P product > 55 mg2/dl2.
A dietary survey was performed at baseline and repeated at the 6-month final evaluation, using a 72-hour mixed food record method11,12. Rations were standardized using the combination of weighing, household measures, food models and photographic archives that included traditional geographical dishes. The Institute of Food Technology’s food composition tables13 were used to transform food consumption into energy and nutrients and The Healthy Food Guide 2004 (Spanish
3 Society of Community Nutrition14) was used to recording the food groups’ consumption. The patients' ideal weight , defined as a body mass index (the weight in kg/square of the height in meters) of 24, was used to calculate the recommended protein and caloric intake.
Intervention. Patients were divided into 2 groups: 1.- Experimental group. Patients in an initial visit with a registered dietitian received instructions (as showed in the attached document) to elaborate menus, with indications about the quantities of food and instructions on how to prepare them. The menus were designed to offer about 0.9-1 g/kg ideal weight/day of proteins, 30 kcal/kg ideal weight/day, 800-900 mg phosphorus/day and 600 mg calcium/day. One important aim was to reduce the phosphorus/protein ratio in the diet. The instructions were adapted to the patients’ dialysis shift and to Mediterranean diet characteristics. This group received an additional 30-minute diet education per month which specifically targeted phosphorus intake. 2.- Control group: the usual dietary recommendations for dialysis patients were explained in the routine medical visits15.
Clinical end-points. We selected two clinical end-points. 1 .- Change in the serum phosphorus levels between the baseline and at 6 months (end of follow-up). A variable called “decrease in serum phosphorus ” was generated. 2 .- Number of patients who achieved serum phosphorus levels < 5.5 mg/dl and Ca x P product < 55 mg2/dl2 at the end of the follow-up.
Variables. We collected data about age, gender, dry weight (kg) and height (meters) and presence of diabetes mellitus. Fasting serum samples were obtained at the baseline and at the 2-, 4- and 6-month follow-up visits, with cholesterol, triglycerides, creatinine, phosphorus, calcium, potassium, albumin, intact PTH (PTHi) and hemoglobin determinations. Analytical determinations were performed using the standard automated analyzers at each hospital. Fat-free mass was determined by an Impedance BIA 101 analyzer, using the body-gram Windows software to interpret the results. Phosphate binders treatment changes, according to serum P levels, were allowed during the follow-up. Clinicians who made decisions about binder dose were
4 blinded to the patients study group. Changes were categorized as none, reduction or increase.
Sample size calculation. To calculate sample size, we considered the results of the studies which suggest that dietary interventions, aimed to reduce phosphorus intake 100-200 mg/day, can reduce serum phosphorus levels more than 1 mg/dl without compromising protein intake16,17,18. We considered clinically significant a 30% difference in the patients number who accomplished a serum phosphorus level of < 5.5 mg/dl between both groups, because this difference could reduce > 10% cardiovascular mortality risk2. With approximately 40 patients per group, we had a 90% power to detect this difference at an alpha risk of 5%. Therefore, we include 90 patients because we estimated that 10% of the patients would leave the study due to clinical complications, renal transplantation or death.
Statistical methods. The quantitative and qualitative variables were described by means and standard deviations and by frequency distribution, respectively. The quantitative variables were compared with a either a Student’s t-test or a non parametric Mann-Whitney U-test, as indicated, and proportions were compared by the χ squared test. The degree of linear association between the quantitative variables was performed using Pearson’s correlation coefficient. The significance of the change of the quantitative variables during the follow-up was evaluated by the Friedman test. Since baseline allocation was performed in accordance with two different cluster-level randomization (the hemodialysis unit and the hemodialysis shift), and since the number of patients was limited, a cluster-analysis was not possible, and we supposed that a selection bias could result. So, in order to improve internal validity of the study, data analysis was focused on individuals instead of clusters, but with a multivariate adjustment for potential confounders. The “decrease in serum phosphorus” difference between groups was adjusted in a multivariate linear regression for age, gender, phosphate binders treatment changes at follow-up, initial phosphorus intake and baseline serum phosphorus levels. The odds ratio (OR) of achieving serum phosphorus levels of < 5.5 mg/dl or a Ca x P product of < 55 mg2/dl2 through intensive dietary intervention, and adjusted for the same factors outlined above, was calculated using multivariate binary logistic regression models. We calculated the
5 95% confidence intervals (CI) of the estimated parameters. P values < 0.05 were considered statistically significant.
6 RESULTS
Ninety-one dialysis patients were selected for participation of whom 80 completed the study, 41 in the experimental group and 39 in the control group. Eleven patients were lost: 3 clinical complications, 3 renal transplant, 2 dialysis unit change, 3 consented withdrawals. At baseline, patients were well balanced as shown in table I. Only hemoglobin levels were significantly lower in the control group.
The dietary survey showed a significantly reduced phosphorus intake in the experimental group (991 ± 252 mg/24 hours baseline vs. 702 ± 168 mg/24 hours end of follow-up; p<0.0001) and in the control group (1033 ± 283 mg/24 hours baseline vs. 872 ± 242 mg/24 hours end of follow-up; p=0.017). Furthermore, at the end of the 6-month follow-up, phosphorus intake was lower in the experimental than in the control group (702 ± 168 vs. 872 ± 242 mg/24 hours; p=0.002). A borderline significantly reduced phosphorus/protein ratio intake was noted in the experimental group (14.1 ± 3.6 baseline vs. 12.8 ± 2.2 end of follow-up; p=0.06), and no modifications were observed in the control group (13.8 ± 2.8 vs. 13.6 ± 2.5; p=ns). However the difference at the end of follow-up between both groups was no significant. There were no significant differences between the experimental group and control group, at the end of follow-up, in either Kcal/kg/day intake (20.8 ± 4.6 vs. 21.8 ± 6.8) or protein/kg/day intake (0.86 ± 0.23 vs. 0.9 ± 0.33).
During the follow-up, serum phosphorus and Ca x P product significantly reduced in both the experimental and control groups (Figures 2 and 3). The PTHi values did not change significantly in either group (Figure 4). Serum phosphorus decreased 1.67 mg/dl in the experimental group and 0.58 mg/dl in the control group, with an unadjusted 1.1 mg/dl difference between both groups (95% CI 0.4-1.8; p=0.002). The serum phosphorus decrease was greater, although not statistically significant, in the patients who reduced the phosphate binders dose (1.9 ± 2 mg/dl) than in those patients with no modification (1.1 ± 1.6 mg/dl ) or increase (0.85 ± 1.4 mg/dl). Besides, the higher the baseline phosphorus serum levels, the greater the serum phosphorus decrease (r=0.56; p <0.01). The decrease of serum phosphorus in the multivariate analysis, adjusted for these factors besides age and gender, was significantly higher in the experimental group (0.93 mg/dl, 95% CI 0.34-1.52;
7 p=0.003). The decrease of Ca x P product was 17 mg2/dl2 in the experimental group and 6 mg2/dl2 in the control group (multivariate-adjusted difference 10.6 mg2/dl2; 95% CI 4.5-16.7; p=0.001). The number of patients achieving serum phosphorus of < 5.5 mg/dl at the end of the follow-up was higher in the experimental group than in the control group (51 vs. 18 %; p=0.002). In the multivariate analysis, the OR of achieving levels of phosphorus < 5.5 mg/dl through intensive dietary intervention was 11 (95% CI 2.7- 44.2; p=0.001). The number of patients achieving Ca x P product < 55 mg 2/dl2 at the end of the follow-up was also higher in the experimental group than in the control group (71 vs. 36 %; p=0.002). In the multivariate analysis, the OR of achieving levels of Ca x P product < 55 mg2/dl2 through intensive dietary intervention was 7.7 (95% CI 2.4-24.7; p=0.001).
Intensive dietary intervention did not deteriorate the patients’ nutritional status. No significant differences were found in the experimental group between the baseline and the end of follow-up values for BMI (25.5 ± 4 vs. 25.7 ± 4), serum albumin (3.8 ± 0.5 vs. 3.7 ± 0.4 g/dl) or fat free mass (44.3 ± 9 vs. 44.7 ± 9.5 %). There were no significant differences between the experimental group and control group, at the end of follow-up, in either BMI (25.7 ± 4 vs. 27.5± 6.1), serum albumin (3.7 ± 0.4 vs. 3.7 ± 0.6 g/dl) or fat free mass (44.7 ± 9.5 vs. 48.4 ± 11.2 %). .
8 DISCUSSION
We found that an intensive 6-month dietary intervention focusing on phosphorus intake reduction is able to obtain an adjusted decrease of 0.93 mg/dl in serum phosphorus levels and increases the probability of obtaining a serum phosphorus level < 5.5 mg/dl by ten.
The phosphorus concentration in the extracellular space is determined by the interactions among intestinal absorption, renal excretion and exchanges with bone and the intracellular space. A normal diet contains approximately 1500 mg of phosphorus, of which approximately 900–1000 mg are absorbed in the intestine (60-70%). Total dialytic phosphorus removal is about 800-1000 mg/session or about 300 mg/day19. Therefore phosphorus retention, with increased serum phosphorus levels, is usual in dialysis patients20. Phosphate binders only partially reduce phosphorus absorption (approximately 40%) with limited tolerance and the need for a large number of tablets. This treatment regimen could results in poor compliance; in fact, some studies have described noncompliance in 40% of patients7,21.
These hemodialysis and binders limitations7,8 make dietary restriction a cornerstone for the prevention and treatment of hyperphosphoremia. However, the typical approach to dietary education and intervention is frequently inadequate. The majority of hemodialysis patients were unaware of the basic facts about the implications of high levels of phosphorus and Ca x P product. Besides the high association of serum phosphorus with hyperkalemia, but not with KTV, suggests poor dietary compliance instead of inadequate dialysis22,23.
The close association between phosphorus and protein intake makes it difficult to restrict dietary phosphorus content without restricting dietary protein intake9. The guidelines recommend a minimal protein intake of 1.2 g/ kg/day for dialysis patients, but these guidelines could be inappropriate. Shinaberger et al.24 found that higher and lower phosphorus levels increased the risk of death (the first association may be due to an elevated protein intake without appropiate P restriction and the second to a decline in protein intake). In fact, an elevated protein intake, which has not proved beneficial, could prevent reaching reasonable levels of serum phosphorus25.
9 In this setting, patients should be encouraged to avoid unnecessary dietary phosphorus (milk, dairy products, certain vegetables) and processed food (the food processing include the addition of phosphorus: fast foods, processed meat, ham and bacon, canned and frozen fish, baking industry, soft drinks, cola drinks)26,27. On the other hand, the bioavailability of phosphorus from various food sources should be considered. Phosphorus in meat is well absorbed, but the low bioavailability of phosphorus in plant proteins means that only 60% of phosphorus from a mixed diet is absorbed. This percentage changes depending on the predominant food groups and the degree of processing foods. This point was contemplated when designing the diet to be used, in which fresh, unprocessed foods predominated28. Thus, a protein intake of 0.9-1 g/Kg/day, with restrictions of non protein sources of phosphorus, and a reduced phosphorus/protein ratio might be the best dietary option.
In our study, intensive dietary intervention attains a clinically important and statistically significant reduction in phosphorus intake and in phosphorus/protein ratio. It is noteworthy that our intensive dietary intervention leads to a decrease in serum phosphorus of 1.67 mg/dl and significantly increases the number of patients accomplishing the recommended serum phosphorus and Ca x P product values. Since it was allowed to adjust the phosphate binders dose according to the clinical criteria in the follow-up, it is not surprising that the doses of those patients with major decreases of serum phosphorus were lowered. Besides, the decline of serum phosphorus is directly proportional to the initial values (regression to the mean). Despite adjusting for these parameters in the multivariate analysis, the difference in the serum phosphorus decrease (0.93 mg/dl) and in the Ca x P product decrease (10.6 mg2/dl2) between both groups is clinically important and statistically significant. In fact, this difference may result in lowering the relative risk of total mortality by 4 % and the relative risk of cardiovascular mortality by 9 %. We failed to demonstrate a decrease in PTHi levels, which is probably attributable to the large range of values and to the limited duration of the study.
The study limitations should be considered. Firstly, allocation was intended in accordance with their hemodialysis unit or shift to avoid a bias resulting from informative contamination between both groups. We recognize that a selection bias
10 could result from this form of participants´ assignment. However, the 2 groups showed a well balanced baseline, and the main results were significant after controlling for potential confounders. Secondly, the nutritional survey is not error- free; this fact may explain why there is no change in nutritional status parameters despite a survey-estimated drop in caloric and protein intake. So, the estimated caloric and protein intake could have been lower than real intake. Thirdly, the number of patients enrolled was limited, although we were able to demonstrate the statistical significance of effect that we consider to be of clinical importance. Finally, the serum vitamin D levels were not measured, making difficult to interpret PTHi changes.
In conclusion, current dialysis and phosphorus binder treatments are not sufficient to assure normal serum phosphorus levels in dialysis patients. A dietary intervention, with a moderate restriction of protein intake (0.9-1 g/kg/day), an increased consumption of fresh foods and a restricted consumption of processed, fast and convenience foods, can reduce phosphorus intake, improve phosphorus-calcium metabolism and maintain adequate nutritional parameters. Finally, because these nutritional recommendations are often unknown to the dialysis patients, it needs to be more extensively disseminated among healthcare professionals dealing with dialysis patients.
11 TABLES AND FIGURES
Table I .- Baseline data for 80 hemodialysis patients categorized into 2 groups: experimental group and control group.
Control Group Experimental group P N = 39 N = 41 Age (years) 63 ± 16 61.3 ± 15 ns Women 46.2 % 48.8 % ns Diabetes Mellitus 22 % 20 % ns BMI (kg/m2) 27.6 ± 6.1 25,5 ± 4.1 ns Serum Creatinine (mg/dl) 8 ± 2.4 8.6 ± 2.2 ns Potassium (meq/l) 5.3 ± 0.9 5.4 ± 0.8 ns Serum albumin (gr/dl) 3.8 ± 0.5 3.8 ± 0.5 ns Cholesterol mg/dl 137 ± 28 140 ± 26 ns Tryglicerides mg/dl 144 ± 64 154 ± 58 ns Serum Phosphorus (mg/dl) 6.8 ± 0.8 7.1 ± 1.5 ns Calcium (mg/dl) 9.4 ± 0.6 9.5 ± 0.7 ns Ca x P product (mg2/dl2) 63.8 ± 8 67.9 ± 13 ns Intact PTH (pg/ml) 491 ± 431 428 ± 446 ns Blood Hemoglobin (g/l) 11.8 ± 1.1 12.3 ± 1.2 0.03 Dietary survey: - Kilocal/Kg/24 h intake 23.1 ± 7.1 25.1 ± 6.9 ns - Protein/Kg/24 h intake 1.13 ± 0.4 1.16 ± 0.4 ns - Phosphorus/protein ratio 13.8 ± 2.8 14.1 ± 3.6 ns - Calcium intake (mg/24 h) 655 ± 264 648 ± 230 ns - Phosphorus intake (mg/24 h) 1033 ± 283 991 ± 252 ns
12 Figure 1: Baseline allocation of the patients to experimental and control groups
MSUH: Miguel Servet University Hospital, CUH: Clinic University Hospital, SJDH: San Juan de Dios Hospital, ALCH: Alcañiz Hospital and MZH: Military Zaragoza Hospital.
Total Patients n: 236
MSUH CUH SJDH ALCH MZH n: 66 n: 70 n: 155 n: 35 n: 10
Excluded Excluded Excluded Included Included Included Excluded Included Excluded Included n: 51 n: 112 n: 50 n: 16 n: 19 n: 43 n: 26 n: 11 n: 8 n: 2
Control group n: 14 Control group n: 10 Control group n:1 Control group Morn: 9 / Aft: 5 Morn: 6 / Aft: 4 Morn: 1 / Aft: 0 Control group n: 14 n: 0 Morn: 9 / Aft: 5
Experiment Experimental group n: 17 Experimental group n: 24 Experimental group Experimental group n: 0 group n=0 Morn: 12 / Aft: 5 Morn: 15 / Aft: 9 n: 0 n: 0
Withdrawn n: 2 Withdrawn n: 5 Withdrawn n: 1 Withdrawn n: 1 Withdrawn n: 2 Experimental n 1 Experimental n 2 Experimental n 1 Experimental Experimental n 1 Control n 1 Control n 3 Control n 0 n:0 Control n: 1 Control n 1
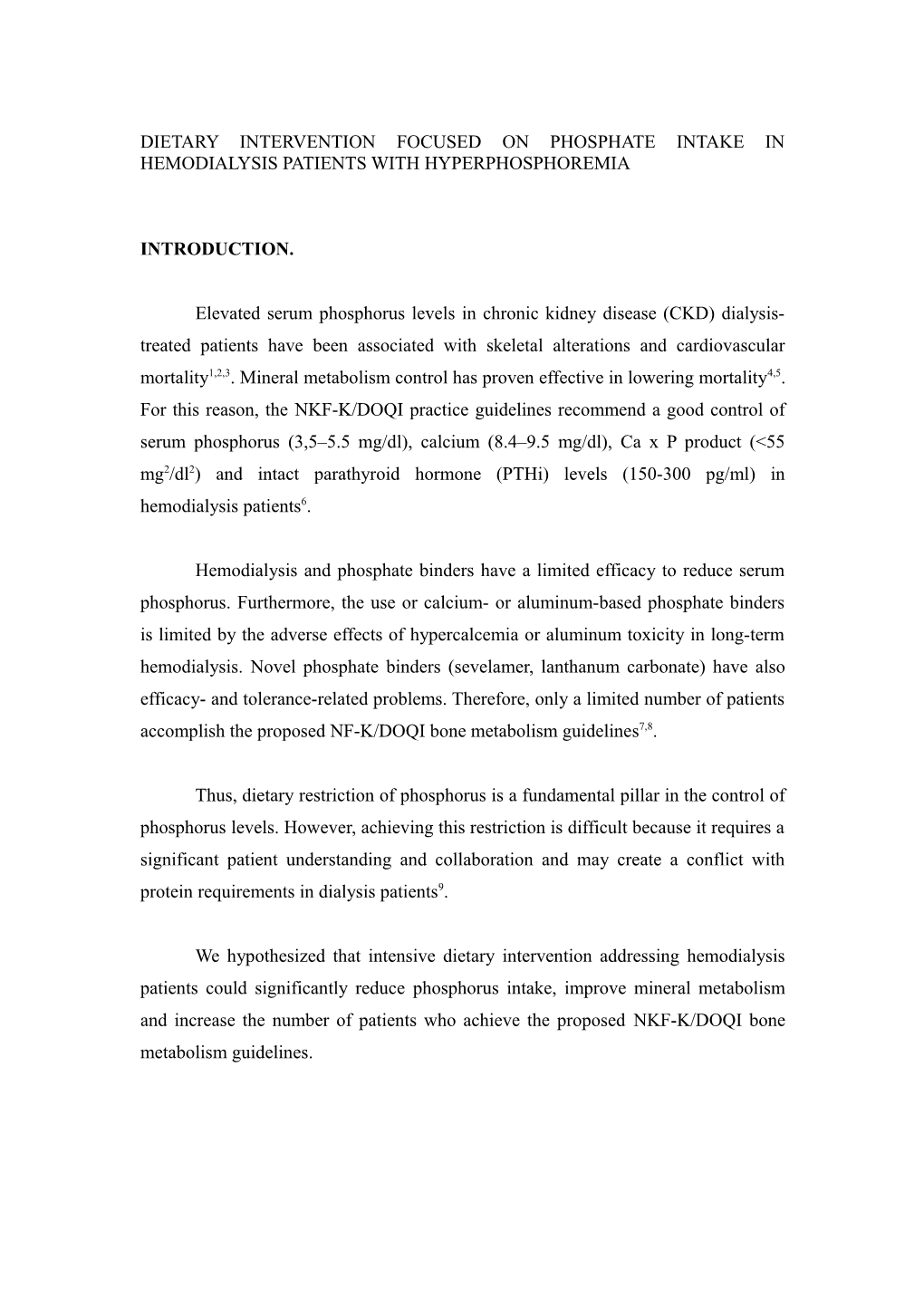
13 Figure 2: Serum phosphorus (P)during the follow-up (mg/dl)
7,5 7 7,1 EXPERIMENTAL CONTROL 6,8 6,5 6,6 p=0,005 6 6,2 6,1 6,2 5,5 5,5 p<0,001 5 5,2 4,5 4 P basal P 2 meses P 4 meses P 6 meses
14 Figure 3: Calcium x Phosphorus product (CaxP) during the follow-up (mg2/dl2).
70 68 EXPERIMENTAL CONTROL 65 64 62 60 58 58 58 p=0,007 55 51 p=<0,001 50 49 45
40
35
30 CaxP in CaxP 2m CaxP 4m Caxp 6m
15 Figure 4: Intact parathyroid hormone (PTHi) levels during the follow-up (pg/ml).
530 480 491 473 EXPERIMENTAL CONTROL 461 450 430 428 407 380 330 347 280 230 p=ns 180 130 80 30 PTHi PTHi 2 m PTHi 4 m PTHi 6 m basal
16 BIBLIOGRAPHY
17 1 Moe S, Drüeke T, Cunningham J, Goodman W, Martin K, Olgaard K, Ott S, Sprague S, Lameire N, Eknoyan G; Kidney Disease: Improving Global Outcomes (KDIGO): Definition, evaluation and classification of renal osteodystrophy : a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 2006; 69:1945-1953.
2 Marco MP, Craver L, Betriu A, Belart M, Fibla J, Fernández E. Higher impact of mineral metabolism on cardiovascular mortality in a european hemodialysis population. Kidney Int 2003; 85: S 111- 114. 3 Block G, Klassen P, Lazarus JM, Ofsthum N, Lowrie EG, Chertow GM. Mineral metabolism, mortality and morbidity in maintenance hemodialysis. J Am Soc Nephrol 2004; 15:2208-2218.
4 Block G, Klassen P, Danese M, Ofsthum N, LaBrecque J, Kim J, Lazarus JM. Association between proposed NKF-K/DOQI bone metabolism and disease guidelines and mortality risk in hemodialysis patients. J Am Soc Nephrol 2003; 14: 474 A.
5 Young EW, Albert JM, Satayatham S. Predictors and consequences of altered mineral metabolism: the Dialysis Outcomes and Practice Patterns Study. Kidney Int 2005; 67:1179-1187.
6 National Kidney Foundation. K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 2003; 42 (suppl 3):S1-202.
7 Young E, Akiba T, Albert JM, McCarthy JT, Kerr PG, Mendelssohn DC, Jadoul M. Magnitude and impact of abnormal mineral metabolism in hemodialysis patients in the dialysis ouctomes and practice patterns study (DOPPS). Am J Kidney Dis 2004; 44 (suppl 2):S34-38.
8 Kim J, Pisoni RL, Danese MD, Satayathum S, Klassen P, Young EW. Achievement of proposed NF-K/DOQI bone metabolism and disease guidelines: Results from the dialysis outcomes and practice patterns study (DOPPS). J Am Soc Nephrol 2003; 14:269A.
9 Rufino M, De Bonis E, Martin M, Rebollo S, Martin B, Miquel R, Cobo M, Hernandez D, Torres A, Lorenzo V. Is it possible to control hyperphosphataemia with diet, without inducing protein malnutrition?. Nephrol Dial Transplant 1998; 13 (suppl 3): S65-67.
10 Lou LM, Gimeno JA, Paúl J, Sanz París A, Gutiérrez Dalmau A, Gómez R, Pérez J, Boned B. Evaluation of nutrient intake in hemodialysis patients. Validity of an appetite and diet assessment and of protein catabolic rate determination. Nefrología 2002; 22:438-447.
11 Arija Val V. y Fernández Ballart J. Métodos de valoración del consumo alimentario. En: Nutrición y dietética clínica. Sales-Salvadó J, Borrada A, Trallero R y Engracia Saló M (eds.). Barcelona: Ediciones Doyma SL: 2000, pp. 55-67.
12 Burrowes JD, Powers SN, Cockram DB, McLeroy SL, Dwyer JT, Cunniff PJ, Paranandi L, Kusec JW. Use on an Appetite and Diet Assessment Tool in the Pilot Phase of a Hemodialysis Clinical Trial: Mortality and Morbidity in Hemodialisys Study. J Renal Nutr 1996; 6:229-232.
13 Mataix Verdú J. Nutrición y Alimentación Humana I. Nutrientes y alimentos. En: José Mataix Verdú (ed.) Madrid, Ed. Ergón, 2002.
14 Calañas-Continente AJ. Alimentación saludable basada en la evidencia. Endocrinol Nutr 2005; 52 (suppl 2):S8-24. 15 Sanders H, Narvarte J, Bittle P, Ramírez G. Hospitalized dialysis patients have lower nutrient intakes on renal diet than on regular diet. J Am Diet Asso 1991; 91:1278-1280.
16 Martínez I, Saracho R, Ocharán J, Muñoz RI, Montenegro J. Role of the diet in the management of renal osteodystrophy in progressive renal failure. 2003; Nefrología 23 (Suppl 2): S57-63. 17 Cupisti A, D´Alessandro C, Baldi R, Barsotti G. Dietary habits and counseling focused on phosphate intake in hemodialysis patients with hyperphosphatemia. J Ren Nutr 2004; 14:220-225.
18 Tanner JL, Craig CB, Bartolucci AA, Allon M, Fox LM, Geiger BF, Wilson NP. The effect of a self-monitoring tool on self-efficacy, health beliefs, and adherence in patients receiving hemodialysis. J Ren Nutr 1998; 8:203-211.
19 Chauveau P, Poignet JL, Kuno T, Bonete R, Kerembrun A, Naret C, Delons S, Man NK, Rist E. Phosphate removal rate: a comparative study of five high-flux dialyzers. Nephrol Dial Transplant 1991; 6 (suppl. 2):S114-115.
20 Ramirez JA, Emmett M, White MG, Fathi N, Santa Ana CA, Morawski SG, Fordtran JS. The absorption of dietary phosphorus and calcium in hemodialysis patients. Kidney Int 1986; 30:753- 759.
21 Hutchinson AJ. Lanthanum and phosphate: science, policy and survival. Kidney Int 2009; 75:355- 357.
22 Poduval RD, Wolgemuth C, Ferrel J, Hammes MS. Hyperphosphatemia in dialysis patients: is there a role for focused counseling?. J. Ren Nutr 2003; 13:219-23.
23 Ford JC, Pope JF, Hunt AE, Gerald B. The effect of diet education on the laboratory values and knowledge of hemodialysis patients with hyperphosphatemia. J Ren Nutr 2004; 14:36-44.
24 Shinaberger CS, Greenland S, Kopple JD, Van Wyck D, Mehrotra R, Kovesdy CP, Kalantar- Zadeh K. Is controlling phosphorus by decreasing dietary protein intake beneficial or harmful in persons with chronic kidney disease?. Am J Clin Nutr 2008; 88:1511-1518.
25 Uribarri J. The obsession with high dietary protein intake in ESRD patients on dialysis: is it justified?. Nephron Physiol 2000; 86:105-108.
26 Uribarri J. Phosphorus homeostasis in normal health and in chronic kidney disease patients with special emphasis on dietary phosphorus intake. Semin Dial 2007; 20:295-301.
27 Sullivan C, Sayre SS, Leon JB, Machekano R, Love TE, Porter D, Marburg M, Sehgal AR. Effect of food additives on hyperphosphatemia among patients with end-stage renal disease: a randomized controlled trial. JAMA 2009; 301:629-635.
28 Uribarri J, Calvo MS. Hidden sources of phosphorus in the typical American diet. Does it matter in nephrology?. Semin Dial 2003; 16:35-41, 2003.