1. Paternity testing
Jack and Jill have a baby called Payle who is 6 months old. However, Jack hears rumours from his friends that Jill may have been unfaithful to him about 15 months ago. Jack is now unsure if Payle is his own child. He therefore requests a paternity test. DNA was extracted from white blood cells from all three individuals and subjected to RFLP analysis. The results are shown below:
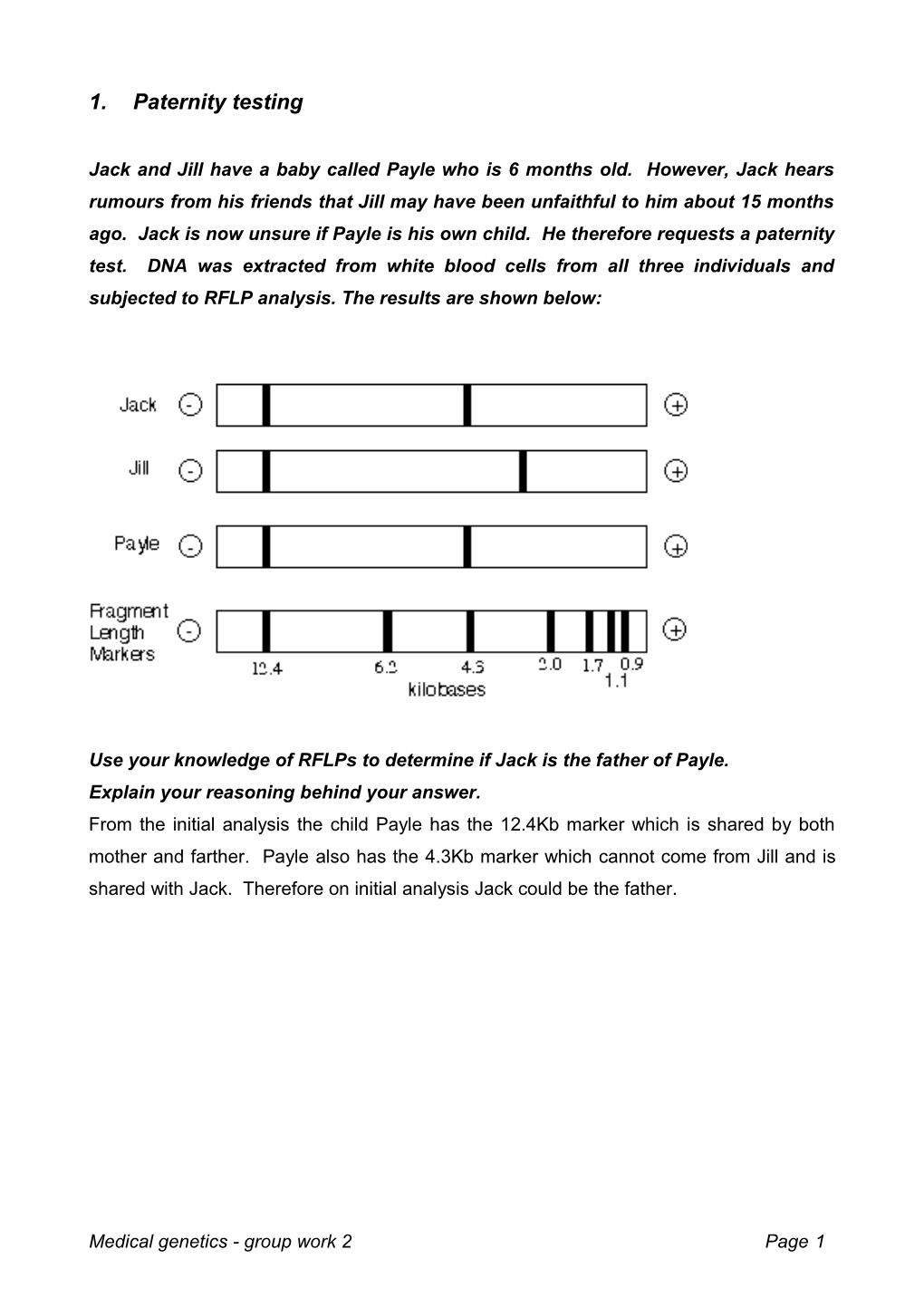
Use your knowledge of RFLPs to determine if Jack is the father of Payle. Explain your reasoning behind your answer. From the initial analysis the child Payle has the 12.4Kb marker which is shared by both mother and farther. Payle also has the 4.3Kb marker which cannot come from Jill and is shared with Jack. Therefore on initial analysis Jack could be the father.
Medical genetics - group work 2 Page 1 RFLP analysis can be unreliable and therefore it is often the situation that a number of analyses will be performed before a true diagnosis is presented. To be certain, several more RFLP loci would be tested. It would be highly unlikely that two men (other than identical twins) would share multiple RFLP patterns and so paternity could be confirmed. In the case of Jack and Jill a second RFLP analysis was performed using a different marker.
From the second analysis would you change your diagnosis? Explain your answer as fully as possible including all possible explanations.
Further analysis using a different marker shows Jack may not be the farther. The second marker has a size of 5.8Kbp and is unique to Payle. Neither Jack nor Jill has this marker. Since Jill is the mother, the marker must arise from another source. It is therefore probable that Jack is not the farther. However there is a slight chance that Payle could have a new SNP which changes his RFLP trace. The chances of this are however very small >1 in 1 000 000. Currently 13 different RFLP makers are use in each criminal or paternity case.
Medical genetics - group work 2 Page 2 2. Blood disorder You are a doctor who has taken a 2 year placement in a small African country. In this country the tropical disease Malaria is prevalent. Within the genome of Africans a single nucleotide polymorphism can occur which changes the binding characteristics for the protein haemoglobin producing HbS. These mutations can confer a resistance to malaria and are beneficial to an individual when in the heterozygous state but can be lethal in the homozygous situation.
From your knowledge of the disease why is the homozygous state potentially dangerous and what common African disease does it confer? The disease is called sickle cell anaemia and the homozygous state affects the movement of red blood cells through the body. Sickle cell suffers frequently have problems in a sickle cell crisis.
A B C D E
A family enter your hospital concerned about the potential for their new born child to have the homozygous trait. Upon questioning you discover that of their 4 current offspring one already suffers from the symptoms consistent with acute anaemia (A). You take blood from the whole family and perform an RFLP analysis.
What is your prediction for the current pregnancy (E)? The child will be a sickle cell sufferer. Mum and Dad are carriers and A has the disease therefore E will have the disease. The higher marker co-segregates for disease.
Medical genetics - group work 2 Page 3 3. Genetic pedigrees On March 7, 1964, the baby known as Pierre was born in a remote part of Quebec Province in Canada. He appeared to be a healthy six-pound twelve-ounce child, except he did not eat well. Over the weeks after his birth, he became progressively more lethargic, vomiting periodically. Most peculiarly, his urine smelled of rotten cabbage, and soon the smell permeated his clothes and body. By the time he was admitted to the hospital on September 14, his muscles were weak and his ribs were showing. Baby Pierre had only gained half a pound in the six months since his birth. The doctors kept him alive by feeding him through a tube threaded through his nose and into his stomach. He gained weight and strength for a while, then suddenly took a turn for the worse. On November 30, baby Pierre vomited blood and died. It soon became increasingly apparent that other babies in the Chicoutimi area of Quebec Province had similar symptoms, and people recalled similar deaths in this remote area 120 miles north of Quebec City. Some families lost several children to Pierre's disease. In those families stricken, it soon became clear that the parents were normal, but about one quarter of their children were afflicted. Boys and girls were equally afflicted. Specialists soon concluded that all of the facts indicated that this was a genetic disorder. 1. If a genetic disorder was the cause, which answer is most likely correct? (A) A pollutant is causing mutations. (B) Multiple alleles are involved. (C) The disease is caused by a dominant allele. (D) Baby Pierre's parents are homozygous for a recessive allele causing the disease. (E) The disease is due to an autosomal recessive. Explain the reason for your choice. There is no reason to suspect that answer (A) is correct from the data given. Pollutants are highly unlikely in remote Quebec and they are not likely to casue specific mutations. The fact that 1/4 of the children are afflicted when the parents aren't suggests a simple 2 allele system involving a defective recessive allele, so answer (B) isn't likely. Answer (C) can't be correct because if a dominant allele causes the disease, the parents would also show it. Answer (D) can't be correct because the parents cannot be homozygous for the disease causing recessive; if they were, they too would have the disease. Answer (E) is the correct choice. The disease clearly is recessive and since females and males were equally afflicted, it is autosomal and not a sex-linked trait.
Baby Pierre and the other stricken children were victims of hereditary tyrosinemia. The children lacked the normal gene which produces a liver enzyme that breaks down the amino acid tyrosine. Without the enzyme, tyrosine builds up in the liver and kidneys
Medical genetics - group work 2 Page 4 leading to the cabbage-like smell of the urine. Lethal side-effects follow. (A liver transplant is the only long-term treatment of the disease as of 1997.) Below is a pedigree of three generations of Canadians.
2. Using the symbols of "a" for recessive allele and "A" for the dominant normal allele write the genotype for the following individuals. A ______Aa______I ______aa______
D ______Aa______K ______Aa or AA______
E ____ _AA or Aa______R ______Aa or AA______
3. Is the above pedigree consistent with a sex-linked trait?
No, otherwise males and females would be affected differently.
4. What is the likelihood that female K will have a normal child if she marries a normal person who is a carrier for tyrosinemia? If K is AA, then all children will be normal (50% will be AA and 50% will be Aa) If K is Aa, then Aa x Aa gives a probability of 3 normal children per 1 diseased child or 75% normal.
Medical genetics - group work 2 Page 5 5. What is the likelihood of female K having a normal child if she marries her cousin M? Cousin M could be either AA or Aa just like K could be AA or Aa. With combinations: AA x AA} all normal children will result AA x Aa} all normal children will result Aa x AA} all normal children will result Aa x Aa} 75% normal
Medical genetics - group work 2 Page 6 Hereditary tyrosinemia is usually quite rare, affecting only 1 in 100,000 newborns. The situation in the French Canadians in Chicoutimi, Quebec, is dramatically different; 1 birth in 685 can be expected to produce a child with the disorder.
6. From the answers below, what is the most likely reason for the large number of tyrosinemia cases in Chicoutimi. Explain the reason for your answer. (A) A high mutation rate. (B) A selective advantage for tyrosinemia in this part of Quebec. (C) Founder effect. (D) Nutritional patterns in the people; large quantities of tyrosine in the diet. (E) Pleiotropy where the allele for tyrosinemia has beneficial effects as well as harmful effects. Reason for your choice: There is no reason to expect a high mutation rate (answer A) or selective advantage (answer B) for tyrosinemia in Quebec. Since it is a genetic disease, answer D is unlikely. Answer E is conceivable but why should it show up only in Chicoutimi? (C) is the most likely answer since it is reasonable to predict Chicoutimi is a small community. (In fact, the Canadian geneticist Dr. Claude Leberge found the Chicoutimi region was settled by a few dozen families who migrated north from Quebec's Charleuoix County. Most people living there are descendants of the original settlers. The tyrosinemia victims can be traced back to one couple, Louis and Marie Gagne, who emigrated from France. It seems likely that either Louis or Marie had the gene for tyrosinemia and passed it to some of their nine children, and innumerable grandchildren, at least two of whom moved to Charleuoix. Their progeny later moved to Chicoutimi. The significant inbreeding produced a high proportion of people who carried the tyrosinemia gene. This is a classic example of the founder effect.)
7. The Hardy-Weinberg equation allows us to make some calculations about the local population. (A) What is the frequency of "aa" individuals? Remember p+q=1 Therefore p2+2pq+q2=1 In the local population, given 1/685 children have the disease and are aa, this means q2 = .00146
(B) What is the frequency of the "a" allele in the local gene pool? q=.0382
Medical genetics - group work 2 Page 7 (C) What is the frequency of the "A" allele in the local gene pool? Since p + q = 1 and q = .0382, then 1 - .0382 = p = 0.9618
(D) What is the frequency of heterozygous individuals in the local gene pool?
2 pq = .073 or 1 person in 14 are Aa individuals. The frequency of aa (homozygous recessive) q2 = .00146 The frequency of AA (homozygous dominants) p2 = 0.925
(E) Assuming random breeding, what are the chances that two carriers will marry in Chicoutimi? .073 x .073 = .0053 or 1 marriage in 190 will involve two carriers
Medical genetics - group work 2 Page 8 Two really hard questions 3. RFLP analysis
Pre-natal diagnosis is attempted for an autosomal recessive condition in a family with one previously affected child (II.2), who died as a consequence of the disease when 2 years old. Individuals II.1, II.3 and II.4 are known to be unaffected. Individual II.5 is the current pregnancy for which the disease status is not yet known. At a marker locus (closely linked to the disorder) there is a polymorphic RFLP with alleles of sizes 7, 9 or 12 kb (referred to as RFLP-7, RFLP-9 and RFLP-12). DNA hybridisation (Southern blot) data are obtained from available family members. What is the diagnosis for the current pregnancy (II.5) ?
I 1 2
II ? 1 2 3 4 5 I.2 II.1 II.3 II.4 II.5
12 kb 9 kb
7 kb
NOTES and HINTS Remember that both the mother and the father must be carriers of the recessive disease allele. Begin by working out which RFLP alleles the father has at the linked marker locus. Then determine, for each parent, which of their two RFLP alleles cosegregates with their respective disease alleles - check your predictions by comparing the expected condition of each child (based upon your answer) with the actual condition recorded.
Medical genetics - group work 2 Page 9 RFLP analysis - Explanation
The children have combinations of RFLP-12, RFLP-9 and RFLP-7 (from their parents). The mother does not have RFLP-7, so this must come from the father. The band corresponding to RFLP-9 in child II.1 is double the intensity of the others, indicating that she has received an RFLP-9 from her father. To simplify discussions later we will use the following notation: Mother has mRFLP-12 and mRFLP-9 (where m indicates maternal). Father has pRFLP-9 and pRFLP-7 (where p indicates paternal).
Because both the mother and father must be carriers of a recessive disease allele, many students will assume that RFLP-9 is the one that cosegregates with the disease allele. This is WRONG - the clearest demonstration that this is wrong involves child II.1. She has two copies of RFLP-9, one from her mother (mRFLP-9) and one from her father (pRFLP-9). If both of these cosegregate with the disease allele then II.1 would be affected by the disease (although the disease is recessive, she would be homozygous for the diseased) but she is unaffected.
The next thought for many will be that RFLP-9 must therefore cosegregate with the normal allele and that the 'other' RFLP in each parent (mRFLP-12 and pRFLP-7) must cosegregate with the disease allele. Again, this is WRONG - the clearest demonstration that this is wrong involves child II.3. He has mRFLP-12 and pRFLP-7. If both of these cosegregate with the disease allele then II.3 would be affected by the disease (although the disease is recessive, he would be homozygous for the disease) but he is unaffected.
It should now be obvious that the disease allele cosegregates with either the mother's RFLP-9 or the father's RFLP-9 (but not both and not neither). This is most likely due to recombination (crossing over) between the RFLP and the disease allele. The original question states that the polymorphic RFLP is closely linked to the disorder - there is no indication of how close the linkage is to the disorder. It would appear that the RFLP is not close enough to prevent recombination between the RFLP and the disease allele.
Unfortunately, the Southern blot does not reveal which RFLP-9 is from the mother and which is from the father. It therefore becomes a problem of logic involving incompatibilities.
If we propose, for example, that the maternal RFLP-9 (mRFLP-9) is linked to the disease. Then, the 'other' maternal RFLP (mRFLP-12) must be normal (because she is heterozygous for the disease) AND the father's pRFLP-9 must be normal (otherwise child II.1 would be affected), in which case, his pRFLP-7 must be linked to the disease (as the father is heterozygous for the disease). In this case: mRFLP-9 is disease mRFLP-12 is normal pRFLP-9 is normal pRFLP-7 is disease BUT this is WRONG (again !) - the clearest demonstration that this is wrong involves child II.4. She must receive the RFLP-7 from her father (pRFLP-7 which, in this example, is linked to the disease) and the RFLP- 9 must therefore be from her mother (mRFLP-9 which is also linked to the disease). In this scenario, child II.4 would therefore be affected by the disease (she would be homozygous for the disease), but she is unaffected.
Since the maternal RFLP-9 is not linked to the disease, it must be the paternal RFLP-9 that is linked to the disease. If so, then using the earlier logic and the same notation, we would have: pRFLP-9 is disease pRFLP-7 is normal mRFLP-9 is normal mRFLP-12 is disease
We can confirm this is correct by considering each child: II.1 has pRFLP-9 (disease) and mRFLP-9 (normal) - expected to be unaffected (correct). II.2 - no blot available, but presumed to be pRFLP-9 (disease) and mRFLP-12 (disease). II.3 has pRFLP-7 (normal) and mRFLP-12 (disease) - expected to be unaffected (correct). II.4 has pRFLP-7 (normal) and mRFLP-9 (normal) - expected to be unaffected (correct).
We can now (finally) determine the diagnosis of the current pregnancy (II.5). II.5 has pRFLP-9 (disease) and mRFLP-12 (disease) and will be AFFECTED.
Working out that II.5 will be affected is the easy bit - telling the parents might be harder !
Medical genetics - group work 2 Page 10 3. ABO blood groups
Use your knowledge of the ABO blood group system to explain how it is possible for a blood type O female (II-5) and a blood type A male (II-6) to produce a child with blood type AB (III-1). It might help to know that the individuals in the first line of the pedigree (I-1 and I-2) are first cousins.
I 1 2 A B
II 1 2 3 4 5 6 O B A AB O A
III 1 2 AB O
Medical genetics - group work 2 Page 11 ABO blood groups - explanation
Using the standard ABO genotype notation, the indicated outcome of this mating is not possible. In fact, it would appear that this is a case of non-maternity. That is, the male parent (II-6) could have contributed an A allele to the AB child but the O type female parent (II-5) apparently could not have contributed a B allele.
I 1 2 A B AO BO
II 1 2 3 4 5 6 O B A AB O A OO BO AO AB OO AO
III 1 2 AB O AB OO
However, it is important to realise that the O blood group is effectively 'zero' with regards to antigenic status and can be classified in a negative manner as not-A and not-B. In order for the A or B antigens to be expressed, not only must the A or B enzymes be present BUT so must the H antigen (or O antigen) since it is the precursor to both the A and B antigens. Individuals unable to make the H antigen are phenotypically blood group O, regardless of whether they express the A and/or B enzymes (if there is no substrate there can be no product).
The H antigen is produced by the addition of core sugars to the proteins and lipids on the surface of the Red Blood Cells. The enzyme responsible for this is encoded by the H gene (which is different to the genes for the A and B antigens): an individual homozygous for the H gene (HH) will produce the H antigen. an individual heterozygous for the H gene (Hh) will produce the H antigen. an individual with two defective versions of the H gene (hh) will not produce the H antigen.
It is now possible to reconsider the pedigree in terms of whether the H antigen is produced. Female II-5 must have been deficient for the H enzyme (hh) while having the ABO genotype of BO. Thus, she could transmit the B allele even though should could not express it. Her parents (I-1 and I-2) can both produce the H antigen, so must be heterozygous Hh. Her husband (II-6) can produce the H antigen, so must contain at least one functional copy of the H enzyme (he could be either HH or Hh).
I 1 2 A B AO BO Hh Hh
II 1 2 3 4 5 6 O B A AB O A ?? BO AO AB BO AO ?? H? H? H? hh H?
III 1 2 AB O AB ?? Hh ??
This is an example of the Bombay Phenotype (it was first described in Bombay, India) and is worth remembering when an irate husband questions blood group anomalies in his children.
Medical genetics - group work 2 Page 12 Medical genetics - group work 2 Page 13