Appendix 2: Aetiological Themes within included studies
Aetiological Number of Studies Aetiological Sub Study reference(s) Diagnostic Confounders Ratio of Developing Summary of Overarching within over- Theme Classification controlled for schizophrenia with Findings Theme arching theme system used: proposed variable.
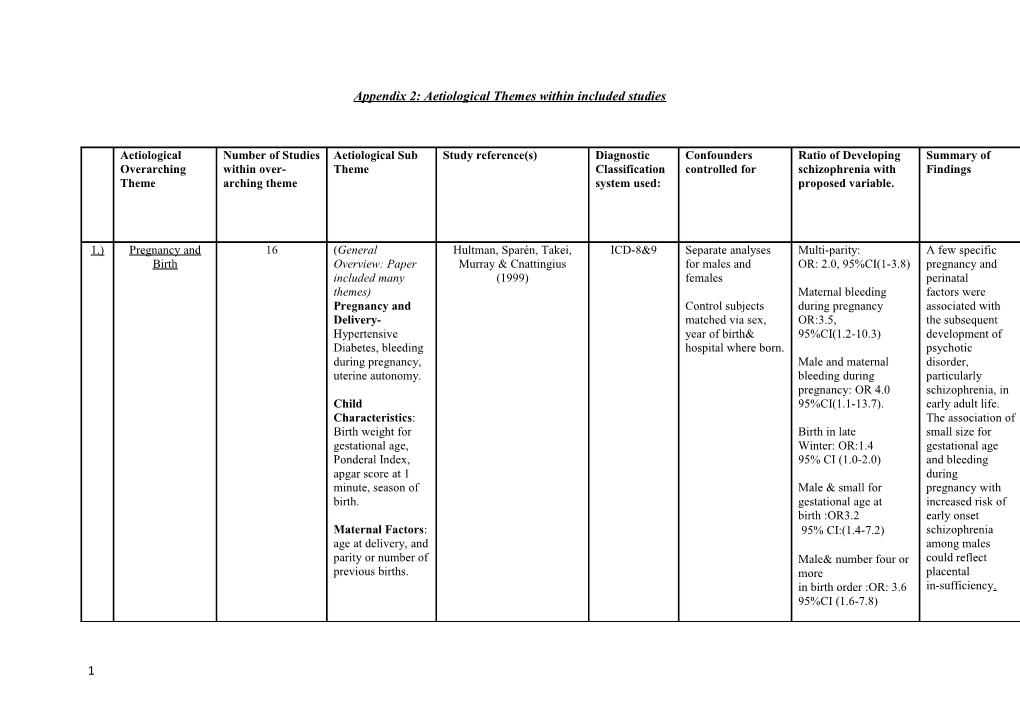
1.) Pregnancy and 16 (General Hultman, Sparén, Takei, ICD-8&9 Separate analyses Multi-parity: A few specific Birth Overview: Paper Murray & Cnattingius for males and OR: 2.0, 95%CI(1-3.8) pregnancy and included many (1999) females perinatal themes) Maternal bleeding factors were Pregnancy and Control subjects during pregnancy associated with Delivery- matched via sex, OR:3.5, the subsequent Hypertensive year of birth& 95%CI(1.2-10.3) development of Diabetes, bleeding hospital where born. psychotic during pregnancy, Male and maternal disorder, uterine autonomy. bleeding during particularly pregnancy: OR 4.0 schizophrenia, in Child 95%CI(1.1-13.7). early adult life. Characteristics: The association of Birth weight for Birth in late small size for gestational age, Winter: OR:1.4 gestational age Ponderal Index, 95% CI (1.0-2.0) and bleeding apgar score at 1 during minute, season of Male & small for pregnancy with birth. gestational age at increased risk of birth :OR3.2 early onset Maternal Factors: 95% CI:(1.4-7.2) schizophrenia age at delivery, and among males parity or number of Male& number four or could reflect previous births. more placental in birth order :OR: 3.6 in-sufficiency. 95%CI (1.6-7.8)
1 2.) Foetal Growth and Abel, Wicks, Susser, ICD 9&10 Sex, Year of Birth, 500-1499g: OR:1.66 An association Development Dalman, Pedersen, Bo Maternal 95%CI: (1.14-2.42) between birth Mortensen & Webb (2010) Psychiatric weight and adult Admission, and 1500-1999g:OR:1.94 mental disorder Social Class 95% CI(1.53-2.47) was found, but (General measure with for any psychiatric 2000-2499g: OR:1.44 no indication the diagnosis) 95%CI (1.24-1.67) effect was specific to a birth weight No adjustment for Schizophrenia overall less Obstetric risk small for than 2500 g or to Complications. gestational age( Schizophrenia. 2 SDs less than the Low birth weight normal birth weight may represent a for a particular mechanism for a gestational age) general OR: 1.34 psychiatric 95% CI (1.14-1.58) vulnerability rather than one And/or specific to Schizophrenia. Low for gestational Equally low birth age(<37 weeks) OR: weight may be a 1.34, 95% CI (1.14- marker of risk for 1.58) another variable. 3.) Dalman, Allebeck, ICD 8&9 Being male, birth C-Section: OR: 2.1 An association Cullberg, Grunewald & hospital category 95% CI (0.8-5.6) between Obstetric Koster(1999) (specialised vs main complications and hospital), psychotic Agar score at 5 min of Schizophrenia was illness in mother, 0-6 : OR: 1.5 found with mothers marital 95% CI (0.6-3.6) preeclampsia (an status & mothers indicator of foetal age. Preeclampsia:OR: 2.1 malnutrition) 95% CI (1.1-4.1) This was shown to be the strongest Ponderal Index<20 2.5 individual risk (0.8-8.3) factor for later development of
2 Gestational age<33 Schizophrenia weeks :2.5 within the study. (0.9-7.2) 4.) Gunnell, Rasmussen, ICD 9&10 Controlled for age, (Hazard Ratios): Evidence was Fouskakis, Tynelius, birth weight, birth found to suggest &Harrison(2003) length, gestational Males of low birth birth weight was age, head weight(<2.5kg) associated with circumference, HR: 7.03 Schizophrenia but season of birth, 95% CI : (1.59- 31.10) not other non- urbanicity of affective residence at birth, psychoses.. age of mother, Males of high birth Higher risks Apgar score weight(>4kg): HR: existed for males at1minute, 3.37 who remained Maternal parity, 95%CI:(1.68-6.74) small as adults. Caesarean section The associations birth, congenital with birth weight malformation, indicate that fetal uterine exposures, atony/prolonged including possible labour and parental effects of education. gestational diabetes were concluded to be important in the aetiology of Schizophrenia by the authors. The role of childhood exposures, as indexed by adult height and body mass index, were concluded to be less strong. 5.) Gunnell, Harrison, Whitley, Sex, year of birth, Birth weight Some evidence Lewis, Tynelius& gestational age (Only a weak was provided by
3 Rasmussen(2005) birth-weight, birth association found the study to Length, Low birth weight (per suggest that Caesarean delivery, kg increase in birth patterns uterine atony, weight) HR: 0.90 of risk, in relation mothers parity, 95% CI (0.78 to 1.03) to foetal growth, paternal age, Apgar differ depending score at 5 Babies weighing 2.5 kg on post-natal (above/below) compared to 3.5–4.0 growth patterns. place of birth (three kg: HR: 1.29 Within the study categories: rural, 95%CI(0.85 to 1.96). the increased risk suburban, urban) associated with season of Per 10 cm increase in low body mass birth, family history birth length: index was of psychosis, HR: 0.53, restricted to long childhood 95%CI (0.31 to 0.89 ) babies who socioeconomic became light position (three (fully adults. measures derived adjusted model) from the However, the Swedish population exposures and housing census underlying these 1990: highest associations and annual income of the either parent, biological highest mechanisms socioeconomic mediating them, index of either require further parent clarification and highest educational level of either parent.
6.) Nilsson, Stålberg, ICD 8&9 Maternal age, Low birthweight (less Within the study, Lichtenstein, Cnattingius, maternal than or equal to 1999 individuals with a Olausson &Hultman(2005) complications grams): OR: 1.67 birthweight of less during pregnancy, 95% CI(0.88-3.14 ) than 2300 grams birth year, sex of faced an almost the child, birth order 2000-2299 grams:OR: doubled risk of
4 (first- or second 1.79, 95% CI (1.07- developing born) ,birthplace (at 3.01) schizophrenia home or compared to at hospital; data not Small head individuals with a shown). circumference (less higher than or equal to 31.5 birthweight. cm) :OR: 1.61 Children with a 95% CI (1.03-2.51) small head circumference Born Pre-term (<36 (31.5 cm or less) weeks) had a 60% higher risk of developing OR: 1.68 95%CI schizophrenia (1.05–2.69) compared to children with a larger head circumference. Finally, compared to children born at term (37 gestational weeks or more), children born preterm (36 weeks or less) had a 70% increased risk of developing Schizophrenia. 7.) Nosarti,Reichenberg, ICD 8, 9 &10 Sex, maternal age, Compared with The vulnerability Murray, parity term births (37-41 for hospitalization Cnattingius, Lambe, Yin, and level of formal weeks) with MacCabe, full-time education a range of Rifkin & Hultman(2012) after compulsory Born at 32 to 36 psychiatric school in the weeks’ diagnoses Swedish gestation : (including educational system. HR: 1.6 95% CI:(1.1- Schizophrenia) 2.3) was shown to
5 increase with Less than 32 weeks’ younger gestation: gestational age. HR:2.5 CI (1.0-6.0) Similar associations were not observed for non-optimal foetal growth and low Apgar score within this study. 8.) Dalman, Thomas, David, ICD 8&9 Maternal history of Pre-eclampsia; birth Signs of asphyxia Gentz, Lewis&Allebeck psychosis, maternal weight; gestation; are independently (2001) age; parity; socio- delay in gaining weight associated with economic group; after birth, child Schizophrenia. attendance at remained in hospital antenatal care; other after birth all measured Other factors obstetric but emerged with showed complications confidence intervals <1 significance but measured. after adjustment for this disappeared confounders and other after confounders obstetric and other obstetric complications. complications were taken into Signs of asphyxia at account. birth :OR: 4.4 95% CI:(1.9 to 10.3) 9.) Pregnancy Stålberg Haglund Axelsson ICD 9&10 Maternal age at (Incidence Rate No evidence was &Delivery Cnattingius& birth, parity, Ratios) found for clear Hultman(2007) mother’s Exposed to ultrasound: associations hospitalization at a Males: between pre-natal psychiatric IRR(crude):1.58 ultrasound Clinic and subjects’ 95%CI:(0.99 –2.51); exposure and attained age during Females schizophrenia or follow up. IRR(crude):1.26 other psychoses. 95%CI(0.62–2.55). Other factors relating to 27 of those exposed to place of birth
6 ultrasound developed might have Schizophrenia influenced the results particularly 499 of those not hospital/location exposed to ultrasound of birth with developed higher IRR shown Schizophrenia. for Malmo hospital along IRR’s in Malmo vs with male sex, other hospitals high maternal age, Male’s: 1.55 95%CI preterm births, (0.97–2.46) and mother’s Female’s: 1.26 psychiatric 95%CI(0.62–2.55) care.
10. Thomas, Dalman, David, ICD 8&9 Controls were Labour>12 hours The study did not ) Gentz, Lewis& Allebeck matched on age, Male’s: find any large or (2001) gender, hospital of 0.75 consistent effect birth and parish of (0.47-1.21) of gender, age at birth Female’s:1.23 diagnosis or (0.62-2.41) maternal history of psychosis on Abnormal presentation the risk of Males: 1.00 schizophrenia (0.44-2.29) associated with Female’s: 1.20 individual (0.44-3.3) complications.
Instrumental Delivery Male’s: 0.90 (0.53-1.53) Female’s: 1.43 (0.63- 3.2)
Cord around neck at birth: Male’s: 1.08 (0.81-1.46)
7 For further non- significant variables see paper. 11. Class, Abel, Khashan, ICD 8,9&10 Adjusted for Adjusted OR: 6-0 No association ) Rickert, Dalman, Larsson, offspring sex, birth months preconception was found for Hultman, Långström, order, birthweight, 1.32 (0.88–1.97) schizophrenia but Lichtenstein and gestational associations were D‘Onofrio(2014) age, maternal and Across Pregnancy found for other paternal age, stress: OR: 0.78 CI: psychiatric highest education, (0.49–1.24) morbidities nationality, criminality, severe psychopathology and completed suicide. 12. Gunawardana, Davey ICD 9&10 Gender, calendar Inter-pregnancy Those born with ) Smith, Zammit, Whitley, year, interval prior to shorter Gunnell,Lewis parental age, conception inter-pregnancy &Rasmussen(2011) parental intervals(where socioeconomic 13–24 months(vs <6 maternal folate status, place of months) stores are being birth, HR:3.29 replenished) had a obstetric 95% CI(2.00–5.41) higher risk of complications schizophrenia. (Caesarean section 7-12 months (vs <6 or uterine atony), months) However findings birthweight, length HR: 1.96 may be largely of gestation, history 95%CI (1.27– 3.05) explained by of psychosis in women who parents conceive or siblings, family following a short size, and birth inter-pregnancy order. First-borns interval were excluded differing on a from analyses of number of pre-birth inter- characteristics that pregnancy interval could
8 and last-borns from subsequently analyses of post- influence risk of birth schizophrenia, inter-pregnancy (compared with interval. women with longer intervals.) Adjustment for confounders attenuated the associations we observed by approximately 30%. 13. Karlsson, Blomström, ICD 9&10 Comparison Non-affective High levels of ) Wicks, Yang, Yolken subjects matched on psychoses(including anti-gliadin IgG in &Dalman, (2012) sex, Schizophrenia) the maternal date of birth, birth circulation were hospital, and High levels (above the associated municipality. 90th percentile) of IgG with an elevated Controlled for anti-gliadin antibodies risk for the Maternal OR:1.7 development age, immigrant of non-affective status, or mode of 95%CI (1.1–2.8) psychosis in delivery, gestational offspring. age at birth, ponderal index, and However, further birth weight. research is needed to identify the mechanisms underlying this association and in order to develop preventive strategies.
No association was additionally
9 found between Caesarean section and non-affective psychoses(includi ng schizophrenia) within the study. 14. Season of Birth Fouskakis, Gunnell ICD 9&10 Age, sex, birth Birth in winter Months: A moderate ) Rasmussen, weight, birth length, HR: 1.23, increased risk of Tynelius,,Sipos&Harrison, gestational age, age CI: (0.96, 1.59). schizophrenia was 2004) of mother, Apgar shown amongst score at 1 min, winter births, maternal parity, but this did not Caesarean section reach and place of conventional residence of mother levels of statistical & maternal significance. education. There was also no association shown with non-affective psychoses. Finally, there was no evidence that these associations were confounded by measures of foetal growth or maternal socioeconomic position. 15. Hultman, Sparén, Takei, As previously ) Murray,& Cnattingius discussed (1999) 16. Svensson ,Rogvin, Hultman, ICD 8,9&10 Not discussed Recurrence Risk Ratio Season of birth ) Reichborn, Winter Birth (Jan- only factor not to Kjennerud,Sandin,&Moger April) modify the effect (2013) RR: 1.00 of familiarity for 95% CI: (0.97–1.03) Schizophrenia
10 within the study (Other variables included: paternal age, age of onset, immigrant status of parents). 1.) Parental Age 9 Dalman and Allebeck ICD 10 Each of the subjects Father aged 45+ Having a father (2002) with schizophrenia OR: 2.8 aged 45 years or was matched with 95% CI (1.3-6.3) older was two subjects from associated with a the parish register Father aged 35-44 doubled risk for who 1) were born OR: 1.5 95%CI (0.9- schizophrenia immediately after 2.6) Compared to the the subject with offspring of schizophrenia, 2) Mothers 40+ fathers aged 20– were matched for OR: 0.6 95% CI (0.2– 24 years. sex and hospital of 1.7), After adjustment birth, and 3) resided for maternal age, in Stockholm at the Mothers <20 years the risk estimates time the cases were OR: 1.2 95% CI (0.7– for fathers was selected. 2.2). increased. Adjusted for possible No association confounders was shown for including: maternal greater maternal age (<20, 20–24, age. 25–39, ≥40 years), parity (1, 2 or 3, ≥4), marital status (married, unmarried, or divorced), socioeconomic index, maternal psychotic illness, and any of the following obstetric complications:
11 preeclampsia, gestational age <33 weeks, small for gestational age, signs of asphyxia (complications expected to yield an Apgar score less than 7 at 1, 5, or 10 minutes), and hyperbilirubinemia (>15 mg/dl). 2.) Ekeus, Olausson &Hjern ICD 9&10 Age, sex, Offspring of older Considerable risks (2005) cephalhaematoma, parents (mother>34 for multiple fetal distress, pre- years) had the highest psychiatric eclampsia, low risk for hospitalisation disorders Apgar score, small for schizophrenia (including for gestational age (RR:1.9 (95% CI 1– schizophrenia), in (SGA), 3.4) those with parents premature rupture of increasing age, of membranes or Paternal age(35-39): remained after breech delivery. RR1.9 95%CI(1 . 3– adjustments 2.7) for social and obstetric factors. 3.) Ek, Wicks,Magnusson, ICD 8,9,10 Adoptees gender (Aged 30-34 used as This study shows &Dalman(2012) (female v. male) reference) that advancing and place of birth adoptive paternal (Sweden v. other Adoptive paternal age: age did not country), advanced Over 40+ increase adopted adoptive maternal OR:1.0 children’s risk of age (≥35 years old 95%CI (0.6–1.6) developing v. <35 years old), schizophrenia or adoptive paternal non-affective socioeconomic psychosis group, residence suggesting any (urban v. non- previous urban), and association shown adoptive parents in- with advancing
12 patient treatment for paternal age in psychiatric disorder familial studies is (yes v. no). likely to have a stronger genetic aetiology.Further studies are needed to confirm this finding. 4.) Delayed Ek, Wicks, Svensson, Idring ICD 8,9,10 Urbanicity, Advancing paternal The association Fatherhood(as & Dalman (2014) advancing maternal age (controlling for between against advancing age, non affective delayed fatherhood) advancing paternal age) psychotic disorder HR : 0.93, 95% paternal age and in mother,father or CI (0.72–1.21) increased risk of sibling, parental schizophrenia in unemployment (comparing 45+ years offspring old fathers to those disappeared after 25–29) controlling for delayed Delayed fatherhood fatherhood(comparison to 25-29 year olds) The association Fathers 35–39 between paternal HR :1.37, age and 95% CI( 1.18–1.58) schizophrenia is not due to paternal Fathers 40–44 years age per se, but old rather HR : 1.81, 95% CI to an unknown (1.44–2.28) factor associated with both delayed fatherhood and schizophrenia.
5.) Frans ,McGrath , Sandin, ICD 8,9,10 Age of spouse, birth Maternal grandfather Offspring of older Lichtenstein Reichenberg year and sex of Aged >55(reference fathers at greater Långström & proband. 20-24 years) risk of Hultman(2011) OR: 2.79 95% CI schizophrenia was (1.71-4.56) confirmed.
13 Aged 50-54 First study to find OR: 1.76 association with 95%CI(1.21-1.58) grandparent age(but maternal Fathers 55+ greatest side only). Having increase in risk OR: a maternal 1.95 grandfather over 95% CI (1.58 to 2.4) age 55 led to an increased risk in Increased risk for offspring; fathers 35+ for ease of however further space please see clarification with paper. regards to the mechanisms behind this is needed. 6.) Sipos, Rasmussen, Harrison, ICD 9&10 Family history, sex, Each 10 year increase The paper gives Tynelius, Lewis, Leon& birth weight, Apgar in paternal age evidence for the Gunnell(2004) scores, and age of HR: 1.47 association onset. Parental 95% CI between increased death. (1.23 to 1.76) paternal age and psychosis to be Association between relatively specific paternal age and to schizophrenia schizophrenia in those with no family history Associations were of the disorder stronger in those For each 10 year with no family increase in paternal age history of the HR: 1.60, 95%CI (1.32 disorder and to 1.92) those with normal apgar scores. With a family history HR:0.91 95%CI (0.44 to 1.89) 7.) Svensson, Lichtenstetin, ICD 8,9&10 Age at onset of Recurrence Risk ratio What may appear Sandin O¨Berg, proband, paternal Siblings of later onset to be a strong
14 Sullivan & Hultman (2012) age, immigrant cases genetic aetiology status of mother RR: 7.2 to Schizophrenia father and sibling 95% CI (6.7–7.9) is infact reduced and season of birth by higher age of Siblings of early onset onset, advancing cases paternal age and RR:10.8 immigrant status. 95% CI (9.4–12.2).
Offspring to fathers above 40 years RR: 6.3 95% CI (5.3–7.3)
Offspring of younger fathers RR:8.6 95% CI (8.0–9.3).
Offspring to parents (maternal immigrants) RR:4.8 95% CI (4.0–5.7)
Paternal immigrants RR: 5.7 95% CI (4.6–6.9) (reference: offspring to parents born in Sweden.) 8.) Svensson ,Rogvin, Hultman, ICD 8,9&10 Not discussed Paternal Age>40 For individuals Reichborn, without familial Kjennerud,Sandin& IRR: 1.36 schizophrenia, a Moger(2013) 95% CI: (1.30–1.43) protective effect was seen across most ages of diagnosis for females, low
15 paternal age, born in rural areas, and being born in later cohorts.
For individuals with familial schizophrenia, a protective effect is found for females diagnosed between ages 18 and 30 years, corresponding values were 18-25 years for low paternal age.
There was no statistically significant effect of paternal age on the proportion of susceptible. 9.) Zammit, Allebeck, Dalman, DSM III Personality Evidence was Lundberg, Hemmingson, variables concerned 10-year increase in provided for Owen & Lewis(2003) with paternal advancing interpersonal age paternal age to be relationships, IQ OR: 1.3 an independent score, place 95% CI(1.0-1.5) risk factor for of upbringing, (Adjusted model) schizophrenia. cannabis use and Adjusting for maternal social age. integration in subjects made little difference to this association,
16 consistent with the hypothesis that advancing paternal age may increase liability to schizophrenia owing to accumulating germ cell mutations. 1.) Social Adversity 10 In Childhood Wicks, Hjern, ICD-8&9 IQ,urbanicity, Households where A number of Gunnell,Lewis & Dalman disturbed behaviour receiving benefits social factors (2005) OR: 1.7 related to the 95% CI (1.5-2.0) parental socioeconomic Single Parent situation were Household; associated with an OR:1.5 increased risk of 95% CI (1.4-1.6) schizophrenia . Measured and Unemployed: OR:1.4 found sig renting 95% CI: (1.2-1.5) apartments, unemployment, For further variables single-parent see paper. households, and households receiving social welfare benefits. May be difficult to generalise to the UK population as migration rules are a lot stricter in Sweden. 2.) Wicks, Hjern & Dalman , ICD 8,9&10 Each analysis was (If without genetic The results 2010 adjusted for sex, liability for psychosis) indicate that
17 age, and the other Adoptees reared in children reared in two exposures. families with parental families with a unemployment disadvantaged HR: 2.0, socioeconomic 95% CI (1.0–4.2) position have an increased risk Single-parent for psychosis. household There was HR:1.2 also some support for an interaction 95% CI (0.6–2.6) effect, suggesting that Living social in apartments disadvantage HR:1.3 increases this risk 95% CI(1.0–1.8) more in children ...... with Genetic liability for genetic liability psychosis alone for psychosis. (without exposure to a less advantaged socioeconomic position in childhood) HR: 4.7, 95% CI (3.1–7.2) ...... Both genetic liability and a disadvantaged socioeconomic situation in childhood
Parental unemployment: HR: 15.0 95%CI (5.4–42.3)
Single parent households:
18 HR:10.3 95%CI: (4.4 - 23.8)
Apartment HR:5.7 95% CI (3.6 -9.0)
3.) In adulthood Hjern, Wicks &Dalman, ICD 9&10 Sex, age, residency, (Risk Ratio) A higher risk of (2004) single adult Low Socioeconomic schizophrenia and households, status(SES) as IV : psychoses was unemployment, 1st Generation found in two white collar SES immigrants generations of and social welfare. (Highest Finnish immigrants Immigrants other of diverse ethnicities see paper) ethnicity. RR: 1.6 95% CI (1 . 3–2.0) As the effect reduced 2nd Generation considerably after (Highest Finnish controlling for Immigrants other socio-economic ethnicities see paper) status the results RR: 2.0 indicate that social 95% CI(1 . 6–2.4) adversity contributes somewhat to the SES as a confounder higher risk. entered into model: (Model which adjusted for SES reduced RR)
RR: 2.1>0.4 non European adults
RR: 2.5 >1.3 youth (Confidence Intervals not listed)
4.) Westman, Johansson& ICD 9&10 Age, income and Immigrants to Sweden The authors found
19 Sundquist (2006) (DSM IV also marital status. from: that several groups noted to be Stratified by gender. of foreign-born used within (Risk of psychotic men and women Swedish disorders exhibited hospitals general)Finland: increased risks of within the Female:HR:1.69 a first hospital study) 95% CI(1.52-1.88) admission (during Male: HR:1.24 the study period) 95%CI(1.10-1.40) due to psychotic disorders. Southern Europe: However the Female: HR:1.65 increased risk of 95%CI (1.37-1.99) psychotic disorders Other non-European decreased to some countries: extent after Female: HR:1.47 adjustment for 95% CI(1.25-1.72) demographic and Male:HR:1.3- socioeconomic 95%CI (1.12-1.50) factors suggesting that social Poland adversity plays a Female: HR:1.32 role in the 95%CI:(1.04-1.67) aetiology of Male:1.55 Schizophrenia, 95%CI (1.14-2.11) with the immigrant Eastern Europe: population at Female: HR:1.32 least. 95%CI: (1.09-1.59)
Low Income(bottom 25% of study population): Female:HR:9.06 95%CI:(8.16-10.06) Male HR: 15.80
20 95%CI(13.50-18.42)
Average Income(Middle 50% of the study population) Female: HR:3.49 95%CI(3.14-3.87) Male: HR: 2.86 95%CI (13.50-18.42)
5.) Some overlap: Zammit, Lewis, Rasbash , Psychiatric Sex, family history (Within Interaction The association Individual and Dalman, Gustafsson Admission of psychosis, being model: effect of L1 between Neighbourhood &Allebeck(2010) 1973 & ICD8- foreign born, variable) urbanicity and adversity 10 moving from the Individual levels of psychosis area, parental deprivation: was concluded by education, parental the authors to be a socioeconomic OR:1.34 reflection of position/unemploy 95% CI:( 1.11-1.63) increased social ment, receipt of fragmentation welfare benefits, Within Interaction present within family income, model: effect of L2 cities. However single parent variable) within the study family, school School level of the majority of grade. deprivation: variation was OR: 1.1 down to individual 95%CI:( 1.00-1.21) level and not neighbourhood level factors. Cross-level interactions between individual- and school-level markers of ethnicity, social fragmentation, and deprivation on risk
21 of developing any psychotic disorder were observed. 6.) Neighbourhood Urbanicity Harrison, Fouskakis, ICD 9&10 Controlling for age, Urbanicity defined as: Urbanization of Level Factors Rasmussen, Tynelius, birth weight, birth Main citiesand birthplace is Sipos& Gunnell (2003) length, gestational subhurbs associated with age, season of birth, increased risk of age of mother, Schizophrenia non-affective APGAR score at 1 HR:1.31 psychosis but this min, maternal 95% CI (0.89-1.93) is not confined to parity, schizophrenia Caesarean section, Other non-affective only The authors sex and maternal psychoses concluded the education. HR:1.57 magnitude of the 95% CI (1.13-2.18). association in Sweden is lower than that reported in other studies. Causal factors underlying this association appear to operate independently of risks associated with obstetric complications and parental educational status(proxy for child SES) as controlling for these variables did not hinder the significance levels within the study. 7.) Population Density Sariaslan, Larsson, ICD 9&10 All statistical Population density Excess risks of D’Onofrio, Långström, models adjusted (population size/km2: schizophrenia, in
22 Fazel, and for sex, birth year at age 15) within the densely populated Lichtenstein(2014) (categorized into 5- general population: and year intervals), and OR = 1.10 socioeconomically birth order 95% CI: (1.09-1.11). deprived Swedish (categorized as first, neighbourhoods second, third, and Within families: appear to fourth OR:1.02 result primarily or more). 95%CI: (0.97- 1.08) from unobserved familial selection Neighbourhood factors, within the deprivation as a study. continuous measure: Previous studies OR:1.43 CI:(1.38; may have 1.49) overemphasized the aetiological importance of these environmental factors. Neighbourhood level effects only account for 2-3% of variance.
8.) Svensson ,Rogvin, Hultman, ICD 8,9&10 Not discussed for Born in an Urban Area Place of birth risk Reichborn-Kjennerud, this section of the (Urbanicity was factor in its own Sandin, & Moger(2013) paper. defined by Swedish right, though census data. Before particularly 1982, subjects born in increased when in communities with less interaction with than 1000 inhabitants familial risk. were considered as (within a frailty rural. For cohorts model approach after 1982, we used the in the second national register from portion of the Statistics Sweden paper: Not SAMS (Small Area discussed here as Market Statistic) log’s were
23 classification data) reported not IRR.)
IRR: 1.24 95% CI:(1.18–1.29)
9.) (Factors in Van der Ven. Dalman, ICD 8&9 Not listed. Looked History of Urban A history of urban migrants)(Not Wicks, Allebeck, at enough variables upbringing upbringing is discussed within Magnusson, van Os, in main analyses to OR:2.3 significantly more our own paper for & Selten (2014) see confounders. 95% CI 1.4–3.7) common in ease of space) migrant groups and may explain the increased risk of schizophrenia previously reported within this group. 10. Zammit, Lewis, Rasbash, Psychiatric Sex, family history Social fragmentation The association ) Dalman, Gustafsson Admission of psychosis, being at school level : between &.Allebeck (2010) 1973 & ICD8- foreign born, (proportion of children urbanicity and 10 moving from the who migrated psychosis area, parental into Sweden, moved appears to be a education, parental into a different reflection of socioeconomic municipality between increased social position/unemploy ages8 and 16 years, or fragmentation ment, receipt of were raised in single- present within welfare benefits, parent households; cities. However family income, median,0.23; 90% the majority of single parent family range, 0.08-0.46), variation was andschool grade. down to individual OR: 1.09 level and not 95% CI: (1.01-1.18) neighbourhood level factors. Social Deprivation at school level (proportion of children with parents unemployed,
24 parents receiving welfare benefits, or parents in lowest 10% of income; median,0.15; 90% range, 0.05 0.30)
OR: 1.16 95% CI(1.10- 1.22) 1.) Population 6 Lichtenstein, Bjork, ICD 8,9&10 Control pairs Recurrence Risk The lifetime Genetics Hultman, Scolnick, Sklar matched to case Schizophrenia in both prevalence of the &Sullivan pairs by gender and parents: narrow definition (2006) year of birth. RR: 89 of schizophrenia 95% CI:( 11.8–672) was 0.407%; it was estimated that Uncles/Aunts RR:3.04 one in every 79 95% CI:(2.39-3.87) extended Swedish families had been First Cousin impacted by RR: 2.29 schizophrenia. 95% CI: (1.71-3.07) The proportion of affected families with multiple affected members was 3.81%.
Recurrence risk estimates for all relative types were similar to those reported in smaller and older studies.
2.) Li, Sundquist, Hemminki& ICD 9&10 Individual variables Both parents had The higher Sundquist(2009) entered into analysis schizophrenia(But only familial risks in rather than 2 cases each so singleton siblings controlled for co- generalisability of and variates. findings: twins compared
25 with spouses Men (SIR:46.19, 95% provide strong CI 4.35–169.87) genetic epidemiological Women (SIR:19.57, evidence for the 95% CI 1.84–71.97) overall heritable effects Familial SIRs for with regard to psychotic disorders in psychotic siblings by age at disorders diagnosis including schizophrenia. (Both genders )Aged <20 years SIR: 15.90 95% CI (5.78-39.39)
Aged 20-29 SIR: 8.65 95%CI(5.10-14.57)
For further ages see paper.
Less than 5 years age difference between siblings: SIR:5.23 95% CI (3.40-8.02 ) Greater than 5 years difference 5.69 95%CI (3.72-8.68)
For other twin(sibling had schizophrenia): SIR:7.34 95% CI (4.79–11.23)
26 Husband (wife was hospitalized for psychotic disorders) SIR: 3.17 95% CI (2.82–3.55)
Wife (Husband was hospitalized for psychotic disorders) SIR : 3.29 95% CI (2.93–3.69)
3.) Lichtenstein, Yip, Björk, ICD 8,9&10 Not listed or no Relative risk The study Pawitan, Cannon, Sullivan& confounders Full siblings: provided evidence Hultman (2009) controlled [RR] 16.4 of a substantial for(familial design 95% CI (15.1–17.7) genetic partially controls for association this) Maternal Half-siblings Between RR: 3·6, schizophrenia and 95% CI (2·3–5·5) bipolar disorder. Additionally Paternal half siblings adopted children RR: 2·7 whose biological 95% CI (1·9–3·8) parents had Schizophrenia had Full-siblings a significantly RR: 9·0, CI:(8·5– increased 11·6); risk for bipolar disorder Shared environmental suggesting an effects RR:4·5 underlying shared 95 %,CI: aetiology. ( 4·4%–7·4%) When relatives of Having a relative with probands with
27 bipolar disorder (even bipolar if reared in a different disorder were environment), RR:7·9 analysed, 95% CI:(7·1–8·8). increased risks for schizophrenia existed for all relationships, including adopted children to biological parents with bipolar disorder. Non-shared environmental effects contributed to comorbidity by around 30% suggesting both an environmental and genetic aetiology is involved in the development of schizophrenia.
4.) Svensson ,Rogvin, Hultman, ICD 8,9&10 Not discussed Familial schizophrenia Increased risk for Reichborn (Defined as sibling schizophrenia was Kjennerud,Sandin, with the disease) shown for those Moger(2013) with previous IRR: 8.16 cases within the 95% CI: (7.62–8.74) family. This was found to be particularly true in the male gender and if other risk factors were present. However this
28 study only discussed risk within the context of having a sibling with the disease not a parent or child. 5.) Svensson, Lichtenstein, ICD 8,9&10 Age at onset of Older paternal age Familial risk was Sandin, O’Berg, proband, paternal (>40 years) found to have a Sullivan&Hultman (2012) age, immigrant greater effect in status of mother (RR:6.3 younger fathers. father and sibling; 95% CI (5.3–7.3) Within this study, season of birth the authors Younger paternal age reported familial RR:8.6 risk decreased 95% CI (8.0–9.3) when higher age of onset, advancing paternal age and immigrant status were controlled for. 6.) Zammit, Lewis, Rasbash, Psychiatric Sex, Family history Familial Within the study Dalman, Gustafsson& Admission of psychosis, being Schizophrenia: the authors Allebeck, (2010) 1973 & ICD8- foreign born, OR: 3.59, concluded the 10 moving from the 95% CI: (2.80-4.59) majority of the area, parental association shown education, parental between urban socioeconomic areas and position/unemploy psychosis was ment, receipt of explained by welfare benefits, individual level family income, variables such as single parent Family history of family, school the disorder. grade. 1.) Non-psychiatric 8 Coeliac Disease Ludvigsson, Osby, Ekbom& ICD,7,8,9&10 Controlled for Coeliac Disease Individuals with co-morbidity Montgomery(2007) existing diabetes schizophrenia: Coeliac Disease
29 and socio-economic HR:1.43 may be at index. Stratified 95% CI (0.77-2.67) increased risk of population by age non-affective of diagnosis of Non-affective psychosis but not coeliac disease, psychosis(that didnt schizophrenia.Ho gender and calender include wever numbers of period. schizophrenia):/ schizophrenia HR:/1.61 cases within the 95% CI (/1.19-2.20) study were low so an association can not yet be ruled out. The authors suggest the association with non affective psychosis may be mediated through nutritional factors in early life or other exposures influencing neurological development; further research is needed to explore such mechanisms. 2.) Darrier Disease Cederlo, Bergen, ICD 8,9&10 Birth year, sex, and (Risk Ratio) An increased risk Langstrom, Larsson , county of Individuals with was found for Boman, Craddock residence(within Darrier disease later , Ostberg , Lundstrom Sweden) Schizophrenia: Schizophrenia in Sjolander, Nordlind & RR: 2.3 individuals with Landen Lichtenstein (2014). 95% CI (1.1–5.2) Darrier Disease. However the Bipolar: increase was RR:4.3(95% CI: 2.6– greater for bipolar 7.3) suggesting any association may
30 Relatives of those with reflect a general Darrier Disease: psychiatric RR: 0.8 vulnerability 95% CI: (0.4–1.8). rather than a direct temporal link. The authors suggest this underlying vulnerability is likely to be genetic but further research is needed. 3.) Head Injury Harrison, Whitley, ICD9&10 Year of birth, After head injury The authors Rasmussen, Lewis, Dalman highest parental exposure: conclude that it is &Gunnell, 2006), income, highest unlikely that head parental education, Non-schizophrenic, injury causes highest parental non-affective schizophrenia. occupation, area of psychoses: A small but birth, family history OR 1.37 significant risk of of psychosis, apgar 95 %CI (1.14–1.66) non-schizophrenic score at 5 min, psychotic gestational age, Schizophrenia disorders and head paternal age, OR:1.10 injury was birthweight, birth 95% CI (0.82 to 1.47) shown ;this was length. not associated with early age of injury or family history of psychosis. The authors stated that further research is needed to clarify the potential roles of social and biological intermediary factors. 4.) Height & BMI Zammit, Rasmussen, ICD 7,8&9 Both height and
31 Farahmand , Gunnell , BMI in early Lewis Tynelius &Brobert adulthood are (2007) strongly and inversely associated with risk of schizophrenia. Genetic and nutritional mechanisms are argued to be the causation behind this, by the authors. 5.) Multiple Johansson, Lundholm, ICD 8,9&10 Matched by birth Diagnosis of MS 2 The risk of Sclerosis(MS) Hillert, Masterman, year and sex. years prior to onset of developing Lichtenstein, Landén & Schizophrenia schizophrenia was Hultman, 2014) lower following HR: 0.71 MS.The 95% CI: (0.51–1.00) association between having a Risk of Schizophrenia sibling with a in siblings of patients psychiatric with MS: disorder and HR: 0.88 developing MS 95%CI(0.71-1.09) was also not significant. Previous research where an association has been shown may be specific to an affective subtype of psychosis rather than schizophrenia specifically. 6.) Rheumatic Sundquist, Li, Hemminki,& ICD 8,9&10 Age in 5 year (Standardised Neither men nor Conditions Sundquist, (2008) groups, geographic Incidence ratio.) women had an
32 regions divided into Women: Ankylosing increased risk of large cities with a Spondylitis Schizophrenia population of over SIR: 3.30 following 200,000. 95% CI:(0.62-9.76) rheumatic conditions, Systemic Lupus however Erythematosus associations were SIR:1.35 shown for other 95% CI: (0.25-3.98) Psychiatric disorders. Rheumatoid The results for Arthritis:SIR:0.72 schizophrenia may 95% CI(0.19-1.87) be due to the small numbers of cases Men: Ankylosing of schizophrenia Spondylitis within the study. SIR: 0.33 95% CI: (0.00-1.87)
Systemic Lupus Erythematosus SIR 2.13 95% CI (0.00-12.20)
Rheumatoid Arthritis SIR: 0.72 95% CI (0.19-1.87) 7.) Sensory(and David, Malmberg ICD-8 Not discussed but Hearing Impairment: Left handedness neurological) ,Lewis,Brandt, Allebeck, male only sample so OR: 1.81 (presumably deficits e.g hearing (1995) gender controlled 95% CI (1.2-2.7) A normal variant impairment. for. of cerebral No increase in subjects asymmetry) and found with epilepsy. epilepsy do not confer a risk for No increase for those schizophrenia. with left handedness. Hearing impairment however was
33 shown to increase individuals risk by 80% and may represent a potentially avoidable aetiological factor
8.) Fors, Abel, Wicks, ICD-10& Parental Psychiatric Hearing Impairment at Both hearing and Magnusson &Dalman, Inpatient contact, parental age 4: speech (2013). admissions in occupation, Low OR: 6 impairment in hospital since birth weight, 95% CI (1.6-23.2) childhood linked 1987. premature birth. to increased risk Speech impairment at of early onset age 4 schizophrenia. OR:2.6 The study shows 95% CI:(1.4-4.9) that hearing impairment is likely to be important in more than just elderly populations for psychosis development.
1.) Substance Misuse 9 Alcohol Andréasson & Allebeck, ICD 8 Social background >250g alcohol usage a Although a dose (1991). factors e.g. previous week (comparatively response contact with the to 1-100g). relationship police. OR: 1.8 between alcohol 95 %CI: 1.5-2.1 and Schizophrenia was found within Abstainers also had a the study, as significantly increased abstainers also had risk of being an increased risk hospitalised for further research is Schizophrenia (OR: 1.6 needed to clarify
34 95% CI:1.1-2.5). the findings and whether any underlying moderators can explain the results. 2.) Non Psychotic Lewis, David, Malmberg ICD-8& DSM Other symptoms, Alcohol abuse Nearly 40% of Psychiatric and Allebeck (2000) III personality OR:5.5 those that develop Illness :assessed variables, IQ, drug 95% Cl (1.7-17.5) Schizophrenia had through: taking, family a previous non Somatic symptoms- income and place of Substance abuse Psychotic headache, upbringing. OR:14.0 Psychiatric difficulty sleeping, 95% Cl (7.8-25.0) diagnosis. stomach ache, However the feeling nervous, ( at age 18). authors concluded feeling that other than for down/depressed, Personality angry easily, Disorder, other troubled restless, disorders are upset when things likely to reflect a go wrong pro-dromal phase Other diagnosis: of the illness. Neurosis, Personality disorder, alcohol misuse, substance misuse. 3.) Cannabis Allebeck, Adamsson , DSM III Not listed, unless No OR listed but 69% cases Engstrom, Rydberg ,1993 same as 1989 paper. temporal length developed between diagnosis of Schizophrenia cannabis use following (substance disorder) cannabis disorder and development of diagnosis. (Rest of Schizophrenia sample developed 25%:1-2 years after before substance use, disorder diagnosis) 26%:3-5 years
35 13% 6-9 years
4% >10 years. 4.) Andreasson, Allebeck ICD-8 Hereditary presence (Relative risk) There was no &Rydebeck(1989) of schizophrenia, For >50 uses/cannabis evidence of other drug and episode’s: mental disorder alcohol use, RR: 4.1 prior to cannabis negative social 95% CI: (1.8-9.3) abuse within the background factors. study, 11-50 uses even if the role of RR 2.4, personality traits 95% CI: (0.8-7.6) could not be fully assessed. The 1-10 uses authors concluded RR: 1.2 a different pattern 95% CI:( 0.5-3.1) of mental deterioration was found among cannabis users, with a more abrupt onset of schizophrenic symptoms than nonusers. There was no major difference between users and nonusers in heredity for schizophrenia (or other psychiatric disorders). Negative social background factors were more common among cannabis abusers. Although the
36 number of cases in this study was small, the findings support the hypothesis that cannabis does play an aetiological role in schizophrenia. 5.) Andreasson, Engstrom, ICD-8 Controlled for (Undadjusted) Relative Relative risk of Allebeck& Rydebeck(1987) contact with police, Risk schizophrenia in having ran away (0 reference) cannabis users from home, fathers 1-10 uses: RR:13 was found to be 6 alcohol habits, 95%CI(0.8-2.2) school adjustment, x higher than non- socioeconomic 11-50 uses:RR: 95% users. group, smoking, CI 3.0(1.6-5.5) solvent abuse, (1-10 uses: 1.3x alcohol >50 uses: RR:6.0, risk; 11-50 uses: consumption, 95%CI (4.0-8.9) 3x, 50+ uses: 6x). psychiatric However cannabis diagnosis at After control for other may be a stressor conscription, variables(in log linear for those medication for model): nervous problems, 1-10 uses: RR: 1.5 vulnerable to and family member 95% CI (0.6-3.3) developing on medication for >10 times RR:2.3 95% schizophrenia nervous problems. CI (1.0-5.3) rather than a Additionally necessary or controlled for sufficient factor. psychiatric Of 274 diagnosis at conscription and schizophrenics whether individuals only 21 were in parents had the high divorced. consuming group and only 49 had ever tried
37 cannabis. Additionally the use of cannabis for self- medication for previous psychiatric symptoms cannot be ruled out within the study methodology.
5.) Giordano, Ohlsson, ICD 10 Controlled for General Population at The authors Sundquist, Sundquist& potential prodromal baseline: concluded that Kendler (2014) effects. Looked at OR:10.44, Cannabis abuse effects of other 95% CI: (8.99–12.11) has an appreciable drugs/likely drug causal impact on induced psychosis. Extrapolated future risk for discordant MZ pairs schizophrenia. (=controlling for However, confounding familial population-based factors) estimates of cannabis– 3 year temporal schizophrenia co- delay:OR 3.3 morbidity substantially 7 year temporal delay: overestimate their OR: 1.6 causal association.
(Extrapolated Confidence Intervals not listed) 6.) Manrique-Garcia, Zammit, ICD 8, 9&10. Psychiatric Frequent cannabis Provides evidence Dalman, Hemmingsson, diagnosis at users compared with for an association Andreasson&Allebeck, conscription, IQ non-users(>50 times) : between psychotic (2012) score, disturbed OR: 3.7 outcomes and behaviour, being 95% CI:( 2.3-5.8) cannabis (more
38 brought up in a city than a threefold and being a Ever used cannabis: risk for cigarette smoker OR: 1.8 Schizophrenia). 95%CI (1.3–2.5)
7.) Manrique-Garcia,. Zammit, ICD 8,9&10 Diagnosis of (Patients with History Results of this Dalman, personality of cannabis use) long-term (34 Hemmingsson,Andreasson disorders, family 20 hospital years) follow-up and Allebeck(2014) socio-economic readmissions: OR:3.1; show that position, IQ score, 95% CI :(1.3-7.3) civil status, place of schizophrenia residence, risky use Hospital admission patients with a of alcohol and other lasting more than 2 history of drugs. years. OR: 2.4 ; 95% cannabis use had a CI: (1.1-7.4) significantly higher burden of in-patient care, with regard to hospital readmission and hospital duration, compared with those without a history of cannabis use.
8.) Van der Ven. Dalman, ICD 8&9 Not listed. Looked (Non-affective No difference was Wicks, Allebeck, at enough variables psychotic disorder) found in cannabis Magnusson, van Os and in main analyses to Cannabis use among use between Selten (2014)(Not discussed see confounders. emigrants migrant groups, within paper for ease of OR: 1.6 the study does not space and non significant 95% CI (0.8–3.1) give evidence findings) against an Emigrants(narrow) association RR :0.7 between cannabis 95% CI (0.4–1.2) and Schizophreniabut
39 Emigrants(broad) cant explain the RR: 0.8 risk in this group 95% CI (0.7–1.0) specifically. 9.) Zammit, Allebeck, ICD 8&9 Psychiatric Any use of cannabis Cannabis use was Andreasson, Lundberg& diagnosis at (controlling for other shown to be Lewis (2002) conscription, IQ drug usage) associated with an score, disturbed increased risk of behaviour, being OR 1.3, developing brought up in a city 95 % CI:(1.1 to 1.5) schizophrenia(and and cigarette not psychiatric smoker Cannabis use > 50 illness in general), times consistent OR: 6.7 95% CI:( 2.1- with a causal 21.7) relation (dose dependent). This association was not explained by use of other psychoactive drugs or personality traits relating to social integration, within the study. 1.) Migration and 5 Hjern, Wicks &Dalman ICD 9&10 Single adult (Risk Ratio) A higher risk of Ethnicity (2004) household, adults Low Socioeconomic schizophrenia and having received status(SES) as IV : all psychoses was social welfare, 1st Generation found in two parental immigrants generations of unemployment, (Highest Finnish immigrants urban Immigrants other of diverse residency, housing ethnicities see paper) ethnicity, within and socio-economic RR: 1.6 the study. This is status. 95% CI (1 . 3–2.0) likely to be caused by higher levels of 2nd Generation social adversity (Highest Finnish within migrants.
40 Immigrants other ethnicities see paper) RR: 2.0 95% CI(1 . 6–2.4)
SES as a confounder entered into model: (Model which adjusted for SES reduced RR)
RR: 2.1>0.4 non European adults
RR: 2.5 >1.3 youth (Confidence Intervals not listed)
2.) Maternal Karlsson, ICD 9&10 Comparison (Non-affective The study Immigration Blomström,Wicks, subjects matched on psychosis in offspring) investigated the Yang,Yolken& Dalman, sex, date of birth, influence levels of (2012) birth hospital, and Maternal immigration IgG directed at municipality. to Sweden dietary Authors controlled OR:2.0 Antigens. for Maternal 95% CI (1.3–3.1) Although an age, immigrant increased risk of status, or mode of non-affective delivery, gestational psychosis was age at birth, found in those ponderal index, and whose mothers birth weight had immigrated, this was not found to be associated to levels of dietary antigens.
3.) Lea˜o, Sundquist, Frank, ICD 9&10 Age and 2nd Generation Finnish: Second-generation Johansson, Johansson income(though HR:2.28 immigrants with &Sundquist (2006) partially looked at 95%CI (1.97-2.63) one
41 as an IV) parent born in One parent born in Sweden and Sweden: second-generation HR: 1.51 Finns had a higher 95%CI (1.38-/1.66) risk of being hospitalised for 2nd Generation refugee psychotic HR: 1.64 (1.34-/2.02) disorders, comparatively to Lowest Income Group: the Swedish HR: 1.55 majority 95%CI (1.41-1.72) population. Second-generation refugees had a higher risk of being hospitalised for psychotic disorders than the Swedish majority population. All results remained significant even after adjustment for socio- economic status (income and education). 4.) Westman, Johansson& DSM IV Age, income and (Psychotic disorders: Several groups of Sundquist, 2006 ICD 9&10 marital status for general) immigrants, both women. Finnish Immigrants: men and women, HR: 1.96 had risks of 95% CI(1.52-1.88) hospital admission for Southern European: Psychotic HR:1.65 disorders 95% CI( 1.37–1.99) compared to the Swedish-born Other non European reference group.
42 countries The impact of HR: 1.47 demographic and 95% CI(1.25–1.72) socioeconomic factors Poland on these risks HR: 1.32 seemed to be 95% CI (1.04–1.67) larger for men than for women. Eastern Europe For foreign-born HR: 1.32 men, several of 95% CI(1.09–1.59) the risks no longer remained Low SES: significant after HR: 9.06 adjustment for 95% CI (8.16–10.06) income and marital status. In Single(female): contrast, most of HR: 6.65 the risks for 95% CI (6.24–7.10) foreign-born women remained significant after adjustment for income and marital status. Low income and being single were associated with an increased risk of psychiatric hospital admission. Demographic factors explained more of Psychotic results. than affective- depression etc. 5.) Minority Ethnicity Zammit, Lewis, Rasbash, Psychiatric Looked at Foreign born at school The association
43 Dalman, Gustafsson Admission interaction between level: between &Allebeck (2010) 1973 & ICD8- neighbourhood OR: 1.14 urbanicity and 10 level and individual 95 % CI: (1.07-1.20) psychosis level appears to be a variables(minority In an interactional reflection of ethnicity one of model: increased social these variables) Foreign born at fragmentation individual level: OR: present within 1.32 cities. However 95% CI: (1.16-1.50) the majority of variation was Foreign born at school down to individual level: level(such as OR: 1.16 being foreign 95% CI: (1.02-1.22) born) and not neighbourhood Interaction Effect of level factors. two: OR:0.95 95% CI: (0.91-0.99) 1.) Personality 2 Pre-morbid Malmberg, Lewis, ICD-8 Family history, 40 Personality All variables Schizoid David&Allebeck(1998) parental occupation, Variables assessed. included were Personality(Howev urbanicity, parental Not all can be listed associated with an er could also be divorce. here for ease of space increased risk of categorised as only highest listed schizophrenia Social Adversity) here; please refer to (especially if a paper. number present at the same time). Unhappy at home: OR: However this 4.27 could also be a 95%CI (2.2-8.3) reflection of a pro- dromal phase. Unpopular with peers: Presence of one OR: 4.01 variable only leads 95% CI (2.5-6.4) to schizophrenia in a small number Ran away from home of cases. OR: 3.79
44 95% CI(2.5-5.9)
No steady girlfriend: OR: 3.89 95% CI (2.0-7.9)
1 variable(any): OR: 2.3 95% CI(1.1-4.9) 2 variables: OR: 4.5 95% CI(2.2-9.4) 3 variables: OR: 12.6 95% CI (6.1-26.7) 4 variables: OR: 30.7 95% CI(12.9-73.8) 2.) Premorbid Zammit, Lewis, Dalman ICD-8&9 Urbanicity, Additive model: Although Schizoid &Allebeck(2010). immigration, and Poor social adjustment individual personality paternal age (but no OR:2.40 variables may (Poorer Social adjustment for pre 95% CI:(1.92–2.99) significantly Relations & and peri-natal contribute to one’s Disturbed factors. Disturbed behaviour in risk ,multiplicative behaviour in childhood OR:2.15, models were childhood ) 95% CI:(1.69–2.74) shown to describe the joint effect of Poor social risk relationships and factors more disturbed behaviour adequately than together: additive ones do. RR: 3.7 95% CI (2.8-4.9) 1.) Psychiatric 4 ADHD Larsson, Ryde´n, Marcus ICD 8,9,10 Design itself Those without bipolar An increased risk History Langstrom, Lichtenstein& compared for but who had ADHD of Schizophrenia Lande(2013) genetic and OR: 6.7 in those with environmental 95% CI:(5.9–7.5) ADHD was found. influences(Twin First-degree
45 study). Parents: relatives of OR: 2.22 probands with 95% CI (1.99–2.47) ADHD were more likely to have Offspring: schizophrenia than OR: 1.89 relatives of 95% CI (1.13–3.15) controls The risk of Full siblings schizophrenia was OR: 1.71 similar among 95% CI (1.44–2.04) maternal and paternal half- Maternal half- siblings(who are siblings likely to share the OR: 1.11 same 95% CI : (0.78–1.58) environment) and substantially Paternal half-siblings lower than for full OR :1.06 siblings 95% CI 1.06 (0.79– 1.43)
2.) Lewis, David, Malmberg & ICD-8& DSM Adjusted for other Neurosis OR:4.6, Personality factors Allebeck (2000) III symptoms and 95% Cl (3.2-6.9) (through a diagnosis at diagnosis of conscription, Personality disorder personality personality OR:8.2 disorder) could variables, IQ, drug 95% Cl (5.4-12.3) represent an taking, place of underlying upbringing and Alcohol abuse OR:5.5, vulnerability to family economy. 95% Cl (1.7-17.5) schizophrenia. Male sample. Other diagnoses Substance abuse occurring before OR:14.0 schizophrenia may 95% Cl (7.8-25.0) reflect a prodromal phase Of those who of the illness.
46 developed schizophrenia, 38% (95% Cl 32-45) received a diagnosis of non-psychotic psychiatric disorder at age 18. 3.) Bipolar Song, Bergen, Kuja- ICD 8,9&10 To ensure Risk Ratio The strong co- Specifically Halkola, Larsson, Landen equal follow-up Schizophrenia: occurrence with &Lichtenstein (2014) time, the control RR: 15.3 schizophrenia and was required to 95% CI:( 14.5–16.2) bipolar that was be alive, reside in shown within the Sweden, and have study suggests a no history common of BPD before the aetiology. date of the first Both may have a diagnosis of stronger common the matched genetic aetiology, proband. than environmental. The authors estimated this at: 76% heritability and 24% for non- shared environment. 4.) Zammit, Lewis, Dalman Nordic Version Urbanicity, Psychiatric History Psychiatric history &Allebeck (2010) ICD-8&9 immigration, and OR: 4.15 was significantly paternal age (but associated with didn’t adjust for pre 95 % CI(3.29–5.22) later and peri-natal schizophrenia. factors.) However, although individual variables may significantly contribute to one’s
47 risk ,multiplicative models describe the joint effect of risk factors more adequately than additive ones do.
1 IQ& Cognitive 7 Low IQ David, ,Malmberg, Brandt, ICD 8 Pro-dromal decline. IQ score <74 The effect of IQ . Performance Allebeck &Lewis (1997) Social and OR: 8.6 and later psychotic ) behavioural 95% CI: (3.1-25.4) illness was highly 1.) difficulties (such as significant for having few friends IQ itself as an psychotic disorder or intimate individual risk factor and Schizophrenia relationships), had low predictive specifically. that were identified value at 1.3% in this in the cohort; category. But low IQ had family finances, low predictive place of upbringing Other psychoses & an power predicting and psychiatric IQ of <74 only 3.1% of diagnosis at OR: 5.4 cases. conscription. 95% CI:( 2.6-11.8). Family member on Within this study psychotropic risk for medication. Schizophrenia was also attenuated in comparison to risk for other psychoses 2.) Van der Ven. Dalman, ICD 8&9 Not listed. Looked Low IQ Low IQ within Wicks, Allebeck, at enough variables OR: 0.5, migrants did not Magnusson, van Os &Selten in main analyses to 95% CI (0.3–0.9]) explain the (2014) see confounders. increased prevalence of Schizophrenia within this group(urbanicity was shown to do
48 so however). 3.) Zammit, Allebeck, David, ICD 8&9 Age of onset, Low IQ: Of the 4 Dalman, Hemmingsson, severity of illness, Schizophrenia intelligence Lundberg& Lewis (2004) bipolar, severe OR: 1.26 subtests, reduced depression. 95 %CI:(1.19-1.33) performance for Other Psychoses : OR: verbal IQ, 1.24 visuospatial 95% CI (1.15-1.33) ability, and mechanical ability were associated with increased risk of Schizophrenia that persisted after adjusting for the other subtest measures. This may represent an increased risk for all psychoses rather than schizophrenia in particular.
4.) Zammit, Lewis, Nordic Version Urbanicity, IQ score bottom 1/3 of Although Dalman&Allebeck(2010) ICD-8&9 immigration, and total cohort: individual paternal age( but OR: 2.63 variables such as didn’t adjust for pre 95% CI(2.11–3.26) low IQ may and peri-natal significantly factors.) Low scores on 3 of 4 contribute to one’s IQ measures OR:1.26 risk ,multiplicative 95% CI: (1.19-1.33). models describe the joint effect of Low IQ and poor risk social relationships: factors more RR: 4.0 adequately than
49 95% CI (3.2–5.1) additive ones do.
5.) Cognitive Gunnell, Harrison, ICD 9&10 Controlling for age, Suitability for being an Poor scores for Performance Rasmussen, Fouskakis, birth weight, birth officer test score (risk each of the five Tynelius & Harrison(2002) length, gestational 3 years following test): tests were age, head Schizophrenia: Associated with a circumference, HR:19.99 3- to14- season of birth, 95 % CI: foldincreasedrisk urbanicity of (2.66-150.23) of psychosis, residence at birth, particularly age of mother, Risk for Psychosis: schizophrenia. Apgar score HR: 2.45, CI: 1.00- Poor intellectual at1minute, 6.02) performance at18 maternal parity, years of age was Caesarean section, also shown to be congenital associated with malformation, early-onset uterine psychotic atony/prolonged disorder. labour and parental education. 6.) MacCabe , Lambe , ICD 9&10 Sex, migrant status, Poor School Poor school Cnattingius, Torrång , Björk low birth weight, performance performance , Sham , David , Murray hypoxia, parental (general) across all domains &Hultman (2008) education level, associated with socio-economic HR: 3.9, schizophrenia(and group. 95% CI (2.8–5.3) other psychoses) Repeating a year Repeating a year was also a HR: 9.2, significant 95% CI (3.4–24.7) predictor of schizophrenia. 7.) MacCabe, Wicks, Lofving, ICD-8,9 or10 Urbanicity, highest (Adjusted HR’s) Relative decline in David, Berndtsson, dependent on parental educational Verbal at 18years : verbal ability Gustafsoon, Allebeck cohort. level, and family HR 1.06 between 13&18 &Dalman (2013) history of psychosis 95% CI (0.66-1.69) associated with (to adjust not only increased risk for for genetic liability Change in verbal(13- schizophrenia. A
50 but also for the 18years): HR: 0.59 cognitive decline educational and 95% CI (0.40-0.88) was shown to social consequences more important of growing up with Spatial at 18 years: than initial score a parent having HR: 0.83 at 18. psychosis). 95% CI (0.57-1.22)
Change in spatial(13- 18 years): HR: 1.20 95% CI (0.83-1.72)
Inductive at 18 years: HR: 0.97 95% CI (0.59-1.57)
Change in inductive(13-18years): HR: 0.86 95% CI (0.59-1.26)
51