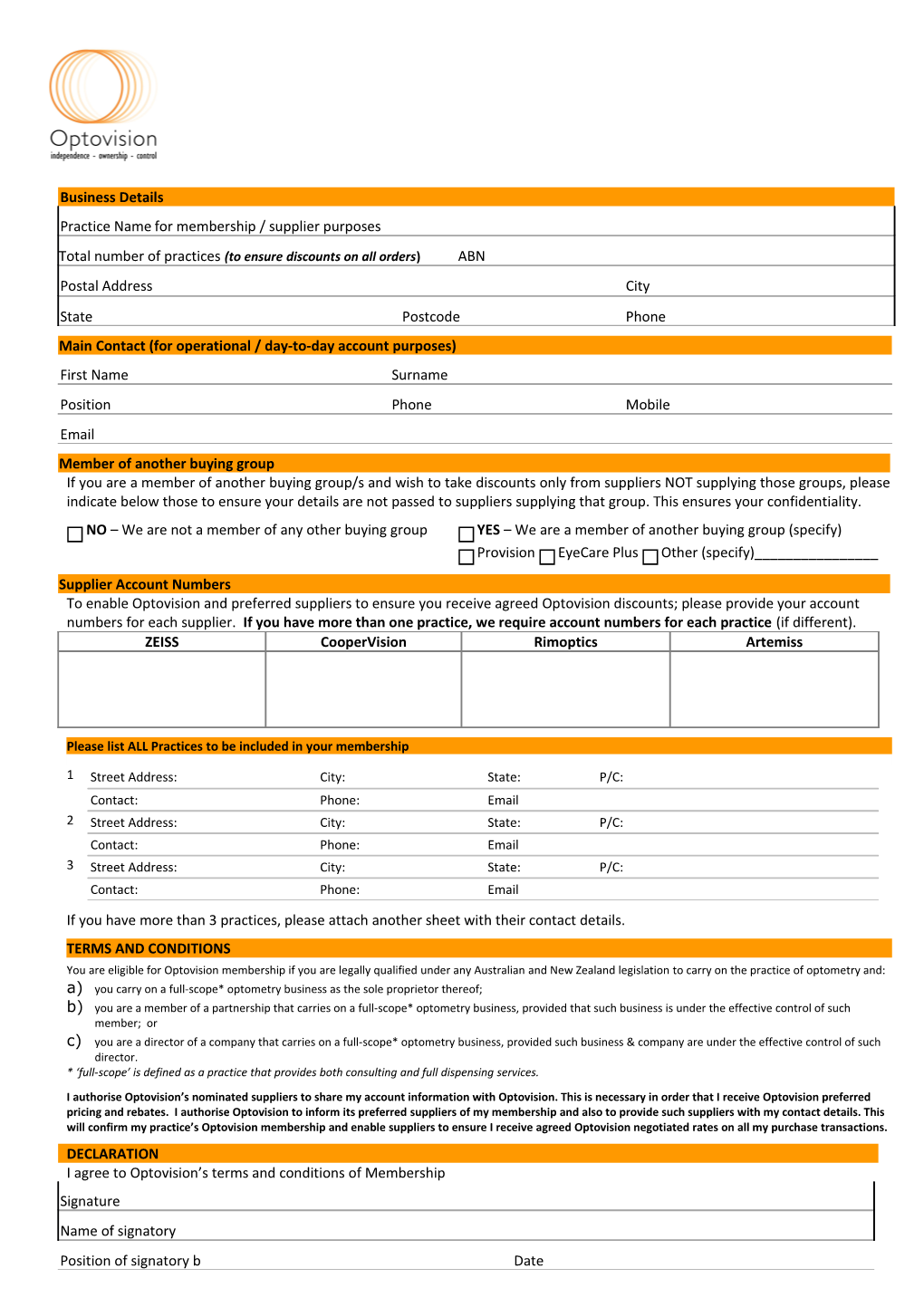
Business Details
Practice Name for membership / supplier purposes
Total number of practices (to ensure discounts on all orders) ABN Postal Address City State Postcode Phone Main Contact (for operational / day-to-day account purposes) First Name Surname Position Phone Mobile Email Member of another buying group If you are a member of another buying group/s and wish to take discounts only from suppliers NOT supplying those groups, please indicate below those to ensure your details are not passed to suppliers supplying that group. This ensures your confidentiality. NO – We are not a member of any other buying group YES – We are a member of another buying group (specify) Provision EyeCare Plus Other (specify)______
Supplier Account Numbers To enable Optovision and preferred suppliers to ensure you receive agreed Optovision discounts; please provide your account numbers for each supplier. If you have more than one practice, we require account numbers for each practice (if different). ZEISS CooperVision Rimoptics Artemiss
Please list ALL Practices to be included in your membership
1 Street Address: City: State: P/C: Contact: Phone: Email 2 Street Address: City: State: P/C: Contact: Phone: Email 3 Street Address: City: State: P/C: Contact: Phone: Email
If you have more than 3 practices, please attach another sheet with their contact details. TERMS AND CONDITIONS You are eligible for Optovision membership if you are legally qualified under any Australian and New Zealand legislation to carry on the practice of optometry and: a) you carry on a full-scope* optometry business as the sole proprietor thereof; b) you are a member of a partnership that carries on a full-scope* optometry business, provided that such business is under the effective control of such member; or c) you are a director of a company that carries on a full-scope* optometry business, provided such business & company are under the effective control of such director. * ‘full-scope’ is defined as a practice that provides both consulting and full dispensing services. I authorise Optovision’s nominated suppliers to share my account information with Optovision. This is necessary in order that I receive Optovision preferred pricing and rebates. I authorise Optovision to inform its preferred suppliers of my membership and also to provide such suppliers with my contact details. This will confirm my practice’s Optovision membership and enable suppliers to ensure I receive agreed Optovision negotiated rates on all my purchase transactions. DECLARATION I agree to Optovision’s terms and conditions of Membership Signature Name of signatory Position of signatory b Date Please forward this signed form to: Email [email protected]