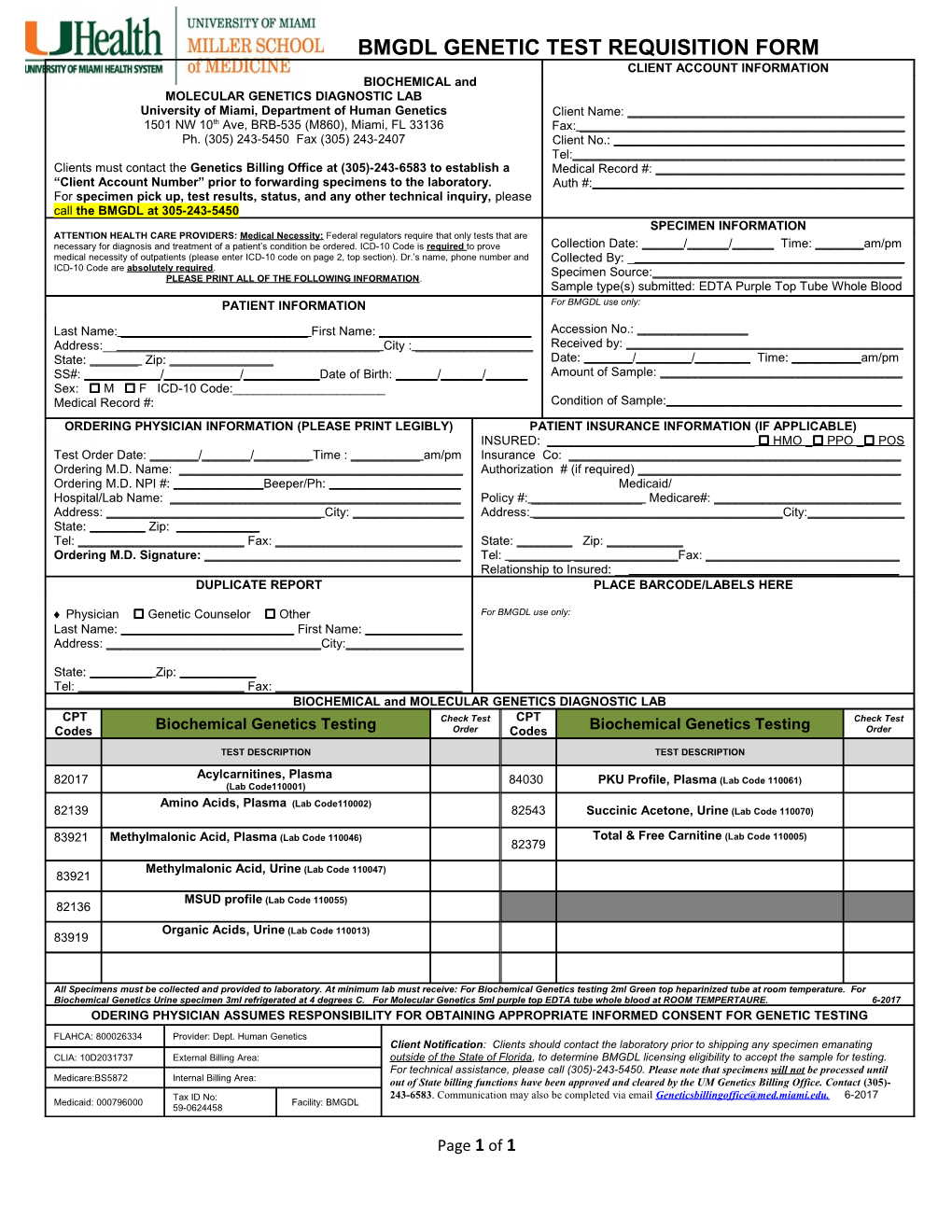
BMGDL GENETIC TEST REQUISITION FORM CLIENT ACCOUNT INFORMATION BIOCHEMICAL and MOLECULAR GENETICS DIAGNOSTIC LAB University of Miami, Department of Human Genetics Client Name: ______1501 NW 10th Ave, BRB-535 (M860), Miami, FL 33136 Fax: ______Ph. (305) 243-5450 Fax (305) 243-2407 Client No.: ______Tel:______Clients must contact the Genetics Billing Office at (305)-243-6583 to establish a Medical Record #: ______“Client Account Number” prior to forwarding specimens to the laboratory. Auth #:______For specimen pick up, test results, status, and any other technical inquiry, please call the BMGDL at 305-243-5450 SPECIMEN INFORMATION ATTENTION HEALTH CARE PROVIDERS: Medical Necessity: Federal regulators require that only tests that are necessary for diagnosis and treatment of a patient’s condition be ordered. ICD-10 Code is required to prove Collection Date: ______/______/______Time: ______am/pm medical necessity of outpatients (please enter ICD-10 code on page 2, top section). Dr.’s name, phone number and Collected By: ______ICD-10 Code are absolutely required. Specimen Source:______PLEASE PRINT ALL OF THE FOLLOWING INFORMATION. Sample type(s) submitted: EDTA Purple Top Tube Whole Blood PATIENT INFORMATION For BMGDL use only:
Last Name: ______First Name: ______Accession No.: ______Address:______City : ______Received by: ______State: ______Zip: ______Date: ______/______/______Time: ______am/pm SS#: ______/______/______Date of Birth: ______/______/______Amount of Sample: ______Sex: M F ICD-10 Code:______Medical Record #: Condition of Sample:______ORDERING PHYSICIAN INFORMATION (PLEASE PRINT LEGIBLY) PATIENT INSURANCE INFORMATION (IF APPLICABLE) GIBLY) INSURED: ______ HMO _ PPO _ POS Test Order Date: ______/______/______Time : ______am/pm Insurance Co: ______Ordering M.D. Name: ______Authorization # (if required) ______Ordering M.D. NPI #: ______Beeper/Ph: ______Medicaid/ Hospital/Lab Name: ______Policy #: ______Medicare#: ______Address: ______City: ______Address: ______City:______State: ______Zip: ______Tel: ______Fax: ______State: ______Zip: ______Ordering M.D. Signature: ______Tel: ______Fax: ______Relationship to Insured: ______DUPLICATE REPORT PLACE BARCODE/LABELS HERE
Physician Genetic Counselor Other For BMGDL use only: Last Name: ______First Name: ______Address: ______City:______
State: ______Zip: ______Tel: ______Fax: ______BIOCHEMICAL and MOLECULAR GENETICS DIAGNOSTIC LAB CPT Check Test CPT Check Test Codes Biochemical Genetics Testing Order Codes Biochemical Genetics Testing Order
TEST DESCRIPTION TEST DESCRIPTION
Acylcarnitines, Plasma 82017 84030 PKU Profile, Plasma (Lab Code 110061) (Lab Code110001) Amino Acids, Plasma (Lab Code110002) 82139 82543 Succinic Acetone, Urine (Lab Code 110070)
83921 Methylmalonic Acid, Plasma (Lab Code 110046) Total & Free Carnitine (Lab Code 110005) 82379
Methylmalonic Acid, Urine (Lab Code 110047) 83921
MSUD profile (Lab Code 110055) 82136
Organic Acids, Urine (Lab Code 110013) 83919
All Specimens must be collected and provided to laboratory. At minimum lab must receive: For Biochemical Genetics testing 2ml Green top heparinized tube at room temperature. For Biochemical Genetics Urine specimen 3ml refrigerated at 4 degrees C. For Molecular Genetics 5ml purple top EDTA tube whole blood at ROOM TEMPERTAURE. 6-2017 ODERING PHYSICIAN ASSUMES RESPONSIBILITY FOR OBTAINING APPROPRIATE INFORMED CONSENT FOR GENETIC TESTING
FLAHCA: 800026334 Provider: Dept. Human Genetics Client Notification: Clients should contact the laboratory prior to shipping any specimen emanating CLIA: 10D2031737 External Billing Area: outside of the State of Florida, to determine BMGDL licensing eligibility to accept the sample for testing. For technical assistance, please call (305)-243-5450. Please note that specimens will not be processed until Medicare:BS5872 Internal Billing Area: out of State billing functions have been approved and cleared by the UM Genetics Billing Office. Contact (305)- Tax ID No: 243-6583. Communication may also be completed via email [email protected]. 6-2017 Medicaid: 000796000 Facility: BMGDL 59-0624458
Page 1 of 1 BMGDL GENETIC TEST REQUISITION FORM
Page 2 of 1