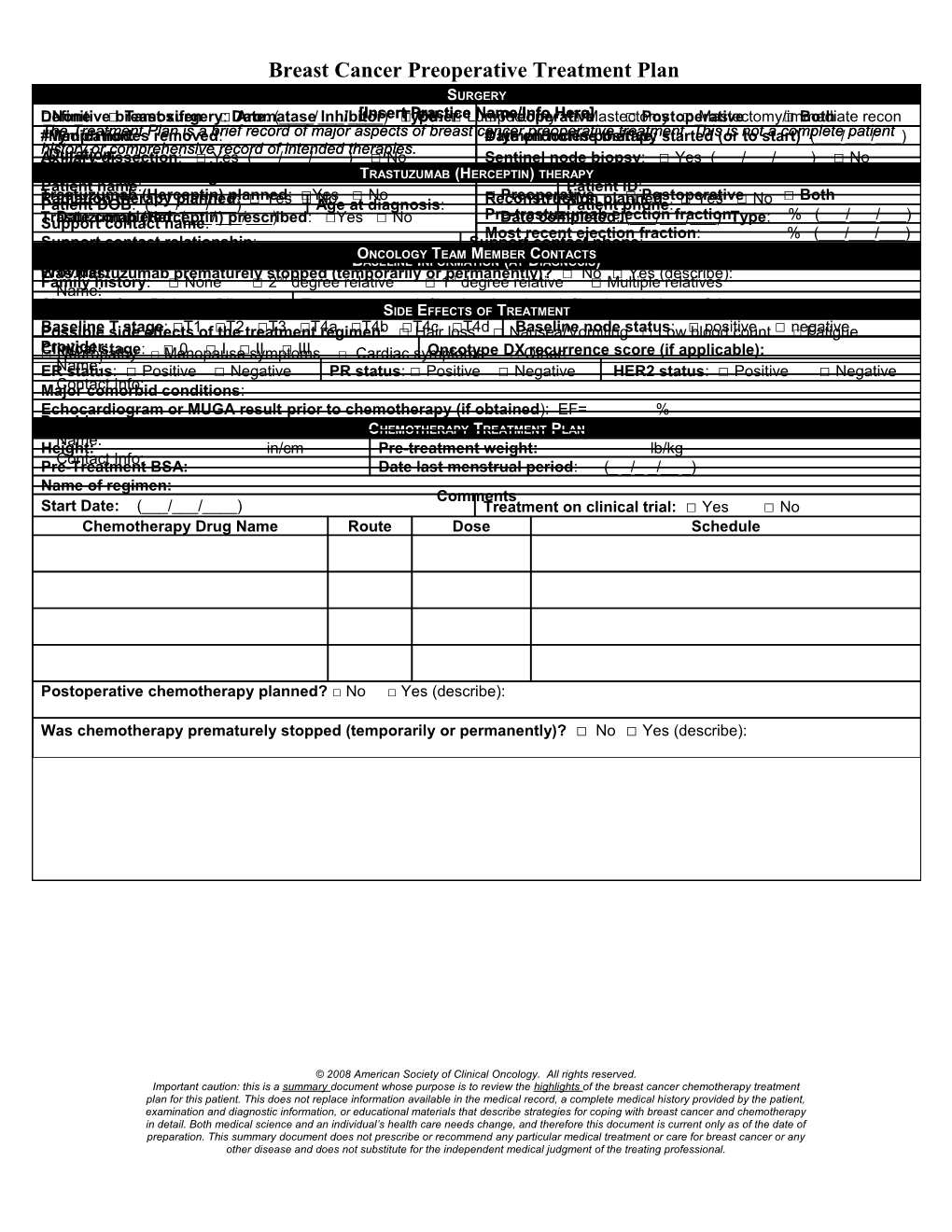
Breast Cancer Preoperative Treatment Plan ENDOCRINESURGERY THERAPY □DefinitiveNone □ breast Tamoxifen surgery □: DateAromatase: (____/___/____) Inhibitor[Insert □Type Practice Other: □ Lumpectomy Name/Info□ Preoperative Here] □ Mastectomy □ Postoperative □ Mastectomy/immediate □ Both recon #The Medication: lymph Treatment nodes Plan removed is a brief: record of major aspects of breast cancerDate# lymph endocrine preoperative notes positive therapy treatment.: started This (or is notto start) a complete (___/___/___) patient history or comprehensive record of intended therapies. Axillary Duration: dissection: □ Yes (___/___/____) □ No Sentinel node biopsy: □ Yes (___/___/____) □ No Medical oncology provider name: Notable surgical findings/comments: T RASTUZUMAB (HERCEPTIN) THERAPY Patient name: Patient ID: Trastuzumab (Herceptin) planned: □Yes □ No □ Preoperative □ Postoperative □ Both RadiationPatient DOB therapy: (___/___/___) planned: □ Yes □ AgeNo at diagnosis: ReconstructionPatient planned phone: : □ Yes □ No Pre-trastuzumab ejection fraction: % (___/___/___) Trastuzumab Support Date completed contact (Herceptin) name: (___/___/___): prescribed : □Yes □ No Date completed: (___/___/___) Type: Most recent ejection fraction: % (___/___/___) Support contact relationship: Support contact phone: Planned or completed dates of trastuzumabO therapyNCOLOGY: T EAM Start M EMBERdate (___/___/___) CONTACTS End date (___/___/___) BASELINE INFORMATION (AT DIAGNOSIS) WasProvider: trastuzumab prematurely stopped (temporarily or permanently)? □ No □ Yes (describe): Family history: □ None □ 2nd degree relative □ 1st degree relative □ Multiple relatives Name: Site Contact: □ Left Info: □ Right □ Bilateral Tumor typeS: IDE □ InfiltratingEFFECTS OF ductal TREATMENT □ Infiltrating lobular □ Other: PossibleBaseline sideT stage effects: □T1 of □theT2 treatment □T3 □T4a regimen □T4b: □□ T4cHair loss□T4d □ Nausea Baseline/Vomiting node status □ Low: □blood positive count □ negative□ Fatigue □Provider:Clinical Neuropathy stage : □ □Menopause 0 □ I □ symptoms II □ III □ Cardiac symptomsOncotype DX □ Other: recurrence score (if applicable): ER Name: status: □ Positive □ Negative PR status: □ Positive □ Negative HER2 status: □ Positive □ Negative Major Contact comorbid Info: conditions: Echocardiogram or MUGA result prior to chemotherapy (if obtained): EF= % Provider: CHEMOTHERAPY TREATMENT PLAN Name: Height: in/cm Pre-treatment weight: lb/kg Contact Info: Pre-Treatment BSA: Date last menstrual period: (_ _/_ _/__ _) Name of regimen: Comments Start Date: (___/___/____) Treatment on clinical trial: □ Yes □ No Chemotherapy Drug Name Route Dose Schedule
Postoperative chemotherapy planned? □ No □ Yes (describe):
Was chemotherapy prematurely stopped (temporarily or permanently)? □ No □ Yes (describe):
© 2008 American Society of Clinical Oncology. All rights reserved. Important caution: this is a summary document whose purpose is to review the highlights of the breast cancer chemotherapy treatment plan for this patient. This does not replace information available in the medical record, a complete medical history provided by the patient, examination and diagnostic information, or educational materials that describe strategies for coping with breast cancer and chemotherapy in detail. Both medical science and an individual’s health care needs change, and therefore this document is current only as of the date of preparation. This summary document does not prescribe or recommend any particular medical treatment or care for breast cancer or any other disease and does not substitute for the independent medical judgment of the treating professional.