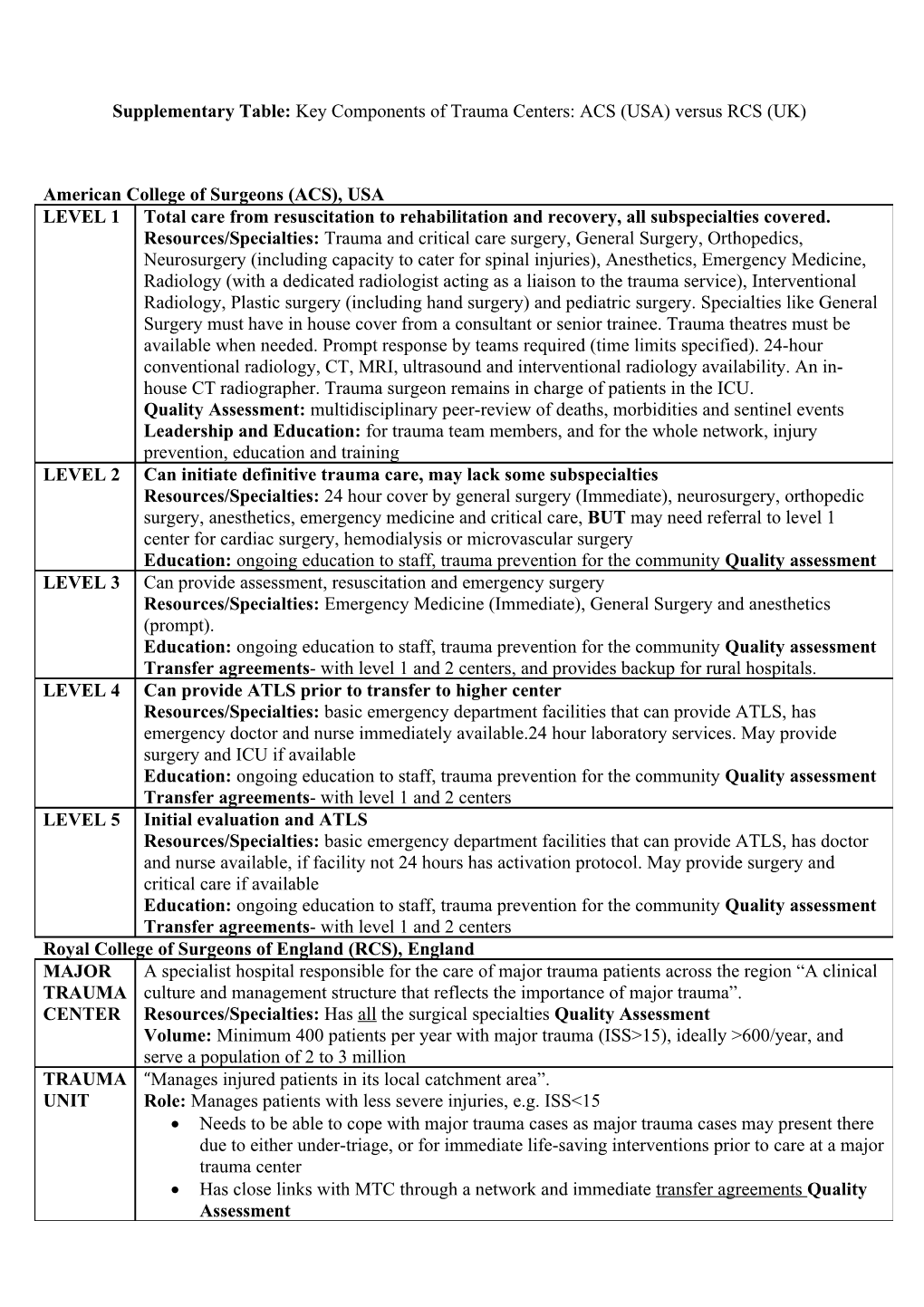
Supplementary Table: Key Components of Trauma Centers: ACS (USA) versus RCS (UK)
American College of Surgeons (ACS), USA LEVEL 1 Total care from resuscitation to rehabilitation and recovery, all subspecialties covered. Resources/Specialties: Trauma and critical care surgery, General Surgery, Orthopedics, Neurosurgery (including capacity to cater for spinal injuries), Anesthetics, Emergency Medicine, Radiology (with a dedicated radiologist acting as a liaison to the trauma service), Interventional Radiology, Plastic surgery (including hand surgery) and pediatric surgery. Specialties like General Surgery must have in house cover from a consultant or senior trainee. Trauma theatres must be available when needed. Prompt response by teams required (time limits specified). 24-hour conventional radiology, CT, MRI, ultrasound and interventional radiology availability. An in- house CT radiographer. Trauma surgeon remains in charge of patients in the ICU. Quality Assessment: multidisciplinary peer-review of deaths, morbidities and sentinel events Leadership and Education: for trauma team members, and for the whole network, injury prevention, education and training LEVEL 2 Can initiate definitive trauma care, may lack some subspecialties Resources/Specialties: 24 hour cover by general surgery (Immediate), neurosurgery, orthopedic surgery, anesthetics, emergency medicine and critical care, BUT may need referral to level 1 center for cardiac surgery, hemodialysis or microvascular surgery Education: ongoing education to staff, trauma prevention for the community Quality assessment LEVEL 3 Can provide assessment, resuscitation and emergency surgery Resources/Specialties: Emergency Medicine (Immediate), General Surgery and anesthetics (prompt). Education: ongoing education to staff, trauma prevention for the community Quality assessment Transfer agreements- with level 1 and 2 centers, and provides backup for rural hospitals. LEVEL 4 Can provide ATLS prior to transfer to higher center Resources/Specialties: basic emergency department facilities that can provide ATLS, has emergency doctor and nurse immediately available.24 hour laboratory services. May provide surgery and ICU if available Education: ongoing education to staff, trauma prevention for the community Quality assessment Transfer agreements- with level 1 and 2 centers LEVEL 5 Initial evaluation and ATLS Resources/Specialties: basic emergency department facilities that can provide ATLS, has doctor and nurse available, if facility not 24 hours has activation protocol. May provide surgery and critical care if available Education: ongoing education to staff, trauma prevention for the community Quality assessment Transfer agreements- with level 1 and 2 centers Royal College of Surgeons of England (RCS), England MAJOR A specialist hospital responsible for the care of major trauma patients across the region “A clinical TRAUMA culture and management structure that reflects the importance of major trauma”. CENTER Resources/Specialties: Has all the surgical specialties Quality Assessment Volume: Minimum 400 patients per year with major trauma (ISS>15), ideally >600/year, and serve a population of 2 to 3 million TRAUMA “Manages injured patients in its local catchment area”. UNIT Role: Manages patients with less severe injuries, e.g. ISS<15 Needs to be able to cope with major trauma cases as major trauma cases may present there due to either under-triage, or for immediate life-saving interventions prior to care at a major trauma center Has close links with MTC through a network and immediate transfer agreements Quality Assessment