Menon Palat Krishna
A. SPECIFIC AIMS
Aspirin as a therapeutic drug has been in use for over hundred years. Its use as an anti-platelet drug was recognized in the early 70s. For secondary prophylaxis of vascular disease, it is the most useful and cost-effective drug. Large number of clinical trials using aspirin has concluded that at any given vascular risk, low to medium dose of aspirin (80-160mg), is as effective as any other drug of choice. However, in recent years, there are several studies, in which aspirin resistance in patients with various vascular diseases have been demonstrated. Furthermore, some studies have suggested worst outcome in aspirin non-responders. The definition of “aspirin resistant” individuals is those whose platelet cyclooxygenase (COX-1) are not inhibitable by aspirin. Thienopyridines (clopidogrel) has also become increasingly important in the management of patients with ischemic vascular disease. Combination of aspirin and clopidogrel has become a standard of care for ASC (acute coronary syndromes) and MIs (ST- elevated myocardial infractions). However according to published reports substantial number of patients do not respond to therapy in spite of regular intake of aspirin and/or clopidogrel. Failure of aspirin and/or clopidogrel to produce inhibition of platelet function can be due to inherited or acquired factors. In the proposed study we will look at the genetic mutations and polymorphisms associated with human platelets, obtained from normal control donors and compare with those of patients found to be non-responders to the action of aspirin and clopidogrel. Overall the study proposal is focused at detecting differences in genetic make up or polymorphism and corroboration with gene expression profiles. Further studies on differentially expressed microarray profile will help to identify novel platelet proteins and genes that may regulate normal and abnormal physiology of platelet function.
Specific Objectives
1. To determine prevalence of aspirin resistance in healthy population using whole blood platelet aggregation. 2. To determine prevalence of clopidogrel resistance in healthy population by whole blood aggregometry studies. 3. To determine the prevalence of aspirin and/or clopidogrel resistance in patient (Diabetics and post MI) population. 4. To study urinary metabolites of thromboxane in order to confirm that the patients are truly aspirin resistant and ADP response of platelets to confirm clopidogrel resistance. 5. To determine the drug resistance polymorphism pattern to understand the genetic mechanism of aspirin and/or clopidogrel resistance. 6. To develop gene expression profile using designed oligo chips for genes responsible for platelet activation and function, probing with platelet RNA isolated from aspirin and/or clopidogrel resistance and non resistance sub groups.
B. BACKGROUND AND SIGNIFICANCE
Role of platelets in the pathogenesis of atherosclerosis, thrombosis and stroke is well documented (1). Therefore, there is a great need for developing specific and effective drugs for modulating platelet function. A thorough understanding of the signaling mechanisms involved in the regulation of platelet function will facilitate the development of better anti-platelet drugs. Agonists interact with the platelet at specific receptor sites on the plasma membrane and initiate a series of signaling events capable of modulating shape change, adhesion, aggregation, secretion of granule contents and expression of activation markers on the
PHS 398/2590(Rev. 09/04) Page - 38 - Menon Palat Krishna
membrane (2-10). Platelet aggregates are formed when the GPIIb/IIIa receptors get activated and bind fibrinogen and recruit other platelets to form clumps. This phenomenon plays a significant role in the formation of effective haemostatic plug as well as growth of thrombus. Weak agonists such as epinephrine, ADP require the production of pro-aggregatory prostaglandin endoperoxides and thromboxane to cause platelet aggregation and secretion. Aspirin is a specific inhibitor of cyclooxygenase and prevents the formation of pro-aggregatory PG endoperoxides.
Data from large number of clinical studies have demonstrated that at any given risk, irrespective of the disease state, aspirin at low to medium concentration is as effective as any other drug (2-5). Although ability of a plant bark (bark of willow, Salix alba) product to reduce fever was discovered two hundred years ago, the mechanism of action of aspirin remained elusive till late 1900 (6). Nobel laureate Sir John R. Vane and his associates at the Royal College of Surgeons, in London, in 1971 proposed the first satisfactory mechanism as to how aspirin works (7, 8). Within a short period of time extensive work was done by various groups to elucidate the mechanism of action of aspirin like compounds (8-20). At the same period, another Nobel Laureate Dr. Bengt Samuelsson of the Karolinska Institute, Stockholm, Sweden, discovered that the prostaglandin synthase produces transient bioactive prostanoids like PGG 2 /PGH2 and thromboxane A2 from the substrate arachidonic acid (10). These findings revolutionized the research in platelet physiology and pharmacology (2-21).
Platelet Physiology:
Blood platelets interact with a variety of soluble agonists such as epinephrine (EPI), adenosine diphosphate (ADP), thrombin and thromboxane (TXA2), many cell matrix components, including collagen, laminin, fibronectin, and vonWillebrand factor and biomaterials used for construction of invasive medical devices (21-29).
GP IIa/IIIa
PHS 398/2590(Rev. 09/04) Page - 39 - Menon Palat Krishna
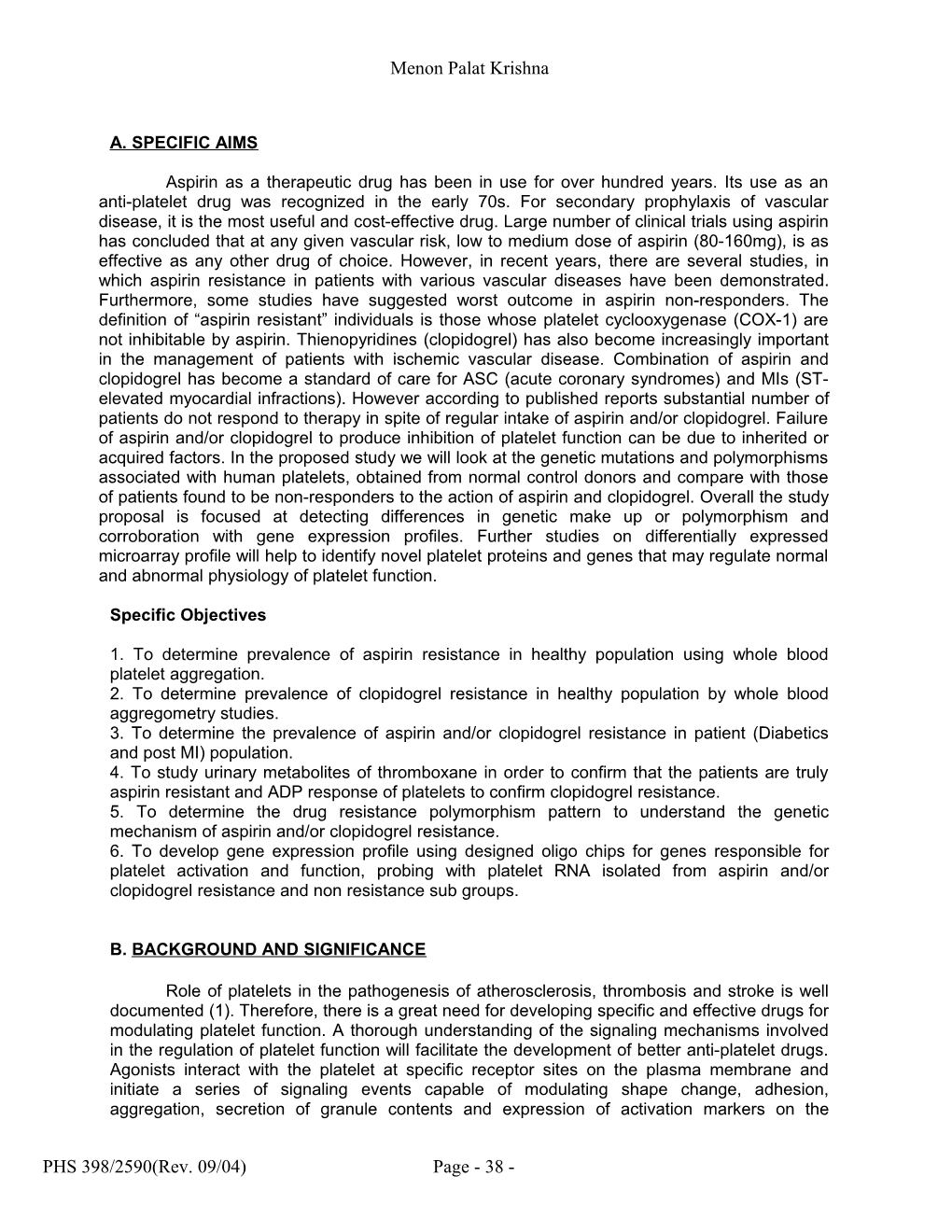
(Platelet aggregation scheme: Numerous agonists activate the platelet, and induce cyto- skeletal changes. The activated platelet changes from a smooth discoid form to an amorphous shape. Dense granules and alpha granules contained in platelet are released, leading to further activation and recruitment of local circulating platelets. Platelet plug formation occurs by platelet to platelet cross linking with fibrinogen bound to glycoprotein IIb-IIIa on the platelet surface.)
These interactions stimulate specific receptors and glycoprotein-rich domains (integrin and non-integrin receptors) on the plasma membrane and lead to the activation of intracellular effector enzymes. Agonist–mediated activation of platelets stimulates Phospholipase C (PLC) and it then triggers the hydrolysis of Phosphatidyl inositol 4, 5-bisphosphate, the formation of second messengers such as 1, 2-diacyl glycerol and inositol 1, 4, 5 trisphosphate. Diacylglycerol activates protein kinase and inositol trisphosphate facilitates the mobilization of free calcium from the storage sites. The majority of regulatory events appear to require free calcium. Ionized calcium is the primary bioregulator, and a variety of biochemical mechanisms modulate the availability of free calcium (27). Elevation of cytosolic calcium stimulates Phospholipase A2 and liberates arachidonic acid (AA). Free AA is transformed to a novel metabolite thromboxane, a potent platelet agonist. This is the major metabolite of AA metabolism and plays an important role in platelet recruitment, granule mobilization, secretion of granule contents, and expression of activated GPIIb/IIIa (ά11b β3) receptors (22-30). Up regulation of activation signaling pathways, will increase the risk for clinical complications associated with thromboembolic episodes.
Aspirin Pharmacology
Arachidonic Acid Metabolism:
Arachidonic acid is a 20 carbon polyunsaturated fatty acid (20:4w6) found in membrane phospholipids. Cell activation stimulates Phospholipase A2, which facilitates the release of this fatty acid from phospholipids. AA is converted to prostaglandin (PG) endoperoxides (PGG2/PGH2) by cyclooxygenase (Prostaglandin G/H synthase; COX1)). Cyclooxygenase exists in 2 iso-forms, COX-1 and COX-2. COX1 is present in nearly all cells, while COX-2 is normally absent from cells but may be produced in response to inflammatory stimuli. These transient metabolites are converted by thromboxane synthetase to thromboxane A2, which is the major metabolite of this pathway in platelets (10). Whereas, in vascular tissues, the endoperoxides generated by COX1 are transformed by prostacyclin synthetase to prostacyclin (PGI2). Thromboxane is a potent platelet agonist and a vasoconstrictor. Prostacyclin is an anti- platelet compound and exerts vasodilatory effects on vascular tissues. Thus from a single substrate (AA), two pharmacologically opposing vasoactive prostanoids are generated by platelets and vascular tissues (3). Aspirin selectively acetylates the hydroxyl groups of a single serine residue (position 529) in the prostaglandin G/H synthase and causes irreversible inhibition of the activity of this enzyme (12, 13). Inhibition of PG synthase results in the decreased conversion of AA to PG endoperoxides, PGG2/PGH2. Molecular mechanisms involved in aspirin-mediated inhibition of prostaglandin G/H synthase are well documented (4- 16). Aspirin works by inhibiting the prostaglandin-producing enzyme cyclooxygenase, which converts arachidonic acid into prostaglandins. The anti-platelet action is through irreversible inhibition of platelet cyclooxygenases (COX-1) at serine residue 529.
PHS 398/2590(Rev. 09/04) Page - 40 - Menon Palat Krishna
A Ser c
(Aspirin mechanism of action, COX: cyclooxygenase, ASA: acetylsalicylic acid, PGG2: prostaglandin G2, PGH2: prostaglandin H2, PGI2: prostacyclin, TXA2: thromboxane A2. 31)
Conversion of arachidonic acid to the various eicosanoids, such as leukotrienes, prostaglandins, thromboxane A2 (TXA2) and prostacyclin, or prostaglandin I2 (PGI2) is catalyzed by COX-1. Thromboxane A2 is a potent vasoconstrictor and platelet agonist found in the α- granules of the platelet, which are released during platelet activation. The platelet prostaglandin thromboxane A2 increases expression of fibrinogen receptors on platelet membranes, facilitating fibrin cross-links between platelets to form a platelet plug. Thromboxane A2 also acts synergistically with other products released by activated platelets such as adenosine diphosphate, fibrinogen, and factor V to further augment platelet aggregation. Once acetylated by aspirin, COX-1 is permanently deactivated and, as enucleate cells, platelets cannot replace the defective enzyme. This effectively halts platelet TXA2 production for the entire 10-day life span of the platelet. In contrast, inhibited COX-1 in vascular endothelial cells is replaced with functional enzymes, and the synthesis of prostacyclin continues. In addition, PGI2 is produced by the enzymatic activity of COX-2, which is 50-100 times less affected by binding with aspirin than COX-1. Therefore, aspirin imparts a platelet inhibitory effect not only by reducing the amount of available TXA2 agonist, but also by increasing the amount of PGI2 relative to TXA2. Additional mechanisms have also been proposed for some of aspirin's clinical effects in cardiovascular disease, including inhibition of platelet aggregation by neutrophils, effects on the endothelium, and antioxidant effects.
Aspirin Resistance
In spite of the wonderful effect of the drug aspirin for a wide range of diseases, the non responders to the drugs are also a major concerned factor. Unfortunately there is no clear definition for aspirin resistance, however conflicting reports and clinical relevance of the term descried various phenomenon. This includes reduce platelet aggregation as measured by in vitro/ in vivo assays, inhibit platelet thromboxane formation, failure of the drug to prevent ischemic events despite regular intake of the doses, incidence of recurrent vascular and persistence of platelet formation etc. Methods used for monitoring aspirin resistance in these studies are non-specific platelet function tests. Differences in the definition of aspirin
PHS 398/2590(Rev. 09/04) Page - 41 - Menon Palat Krishna
resistance, variations in the methods used to detect “non-responders”, inter-individual variations in the response of platelets to the action of different agonists, and lack of data from large clinical trials have hampered the advancement of knowledge in this area. There is very little information available for mechanisms underlying this observed resistance to the action of aspirin. Moreover the failure rate for aspirin respond is approximately 5-60%. Although much is known about the role of aspirin on platelets, the mechanism by which patients are resistance to the drug is not clearly understood (32). There are several extrinsic factors like smoking, higher lipid levels, conditions associated with increased platelet turnover, play a role in influencing anti-platelet effects of aspirin. However few patients may require higher dose which may mot be practical due to gastrointestinal side effects. Certain drugs like non steroidal anti inflammatory drugs (NSAIDs) may play a secondary role in aspirin resistance, which compete interaction to COX1 as both act on COX1. Attempt has been made to describe aspirin resistance by various proposed intrinsic mechanism. Besides platelets, the nucleated cells has also implicated in aspirin resistance mechanism. Those cells reach in TXA2 and have capacity to resynthesis the enzymes. Beside COX-1 mediated generation, those cells can make TXA2 via COX-2. Even erythrocytes have been shown to be prothrombotic and enhance platelet reactivity. All these cell interaction is not consistently blocked by aspirin and may provide alternative pathway for thrombus formation (33). Possible mechanism for aspirin resistance can be summarized as below (34):
Bioavailability Non-compliance Under dosing Poor absorption (enteric coated aspirin) Interference: NSAID co-administration
Platelet function Incomplete suppression of thromboxane A2 generation Accelerated platelet turnover, with introduction into bloodstream Of newly formed, drug unaffected platelets Stress-induced COX-2 expression in platelet Increased platelet sensitivity to ADP and collagen
Single nucleotide polymorphisms Receptors: GPIIb-IIIa, collagen receptor, thromboxane receptor etc. Enzymes: COX-1, COX-2, thromboxane A2 synthase etc.
Platelet interactions with other blood cells Endothelial cells and monocytes provide PGH2 to platelet (by passing COX-1) Synthesis of their own thromboxane A2
Other factors Smoking, hypercholesterolemia, exercise, stress etc
Rather then resistance is it? Aspirin response variability? Platelet response variability? Treatment failure (because arterial thrombosis is multifactorial)?
The role of genetic variation in drug response has become increasingly evident over the past decade. So genetic variation may play a significant role in the manifestation of aspirin
PHS 398/2590(Rev. 09/04) Page - 42 - Menon Palat Krishna
resistance in different patients. Research is currently focusing on identifying specific genes associated with disease and variants of genes or alleles that affect response to drug therapy. Several genetic sequences have been identified that predispose patients to increased platelet aggregation. These inherited genes have been associated with ischemic vascular events. Aspirin resistance associated with genetic polymorphisms is likely to be multi-factorial and is possibly amplified in the presence of other hemostatic genetic variations such as polymorphisms of blood coagulation and fibrinolytic factors. Aspirin effectively blocks the TXA2 pathway via COX1 and polymorphism or mutations of COX-1 gene which is relatively resistance to the action of aspirin may provide a molecular basis for aspirin resistance. It has been shown that polymorphism of serine position 529 could significantly block COX-1 activity to near undetectable label and polymorphism on the carboxyl terminal segment at position 600 of the leucine residue of COX-1 could diminish the COX-1 activity up to 86 % (35). However if the COX-1 gene is dysfunctional, TXA2 may be produced by mechanism other then COX-1 possibly rendering patients with this polymorphism aspirin resistance. Genetic differences in glycoprotein IIb/IIIa receptor complex may also be responsible for varying effect of aspirin in different patients. The glycoprotein IIb/IIIa receptor is the final common pathway for platelet aggregation. Several polymorphisms on GP IIb/IIIa receptor have been identified in the general population. A frequent polymorphism leu33 to proline defines P1A1 and P1A2 alleles and which may associate with increased binding of fibrinogen to the platelet GP IIb/IIIa receptor (36). Recent studies show that a single nucleotide polymorphism (SNP) in the gene PLA2 encoding the GP IIb/IIIa receptor is a risk for acute coronary syndromes (37, 38, 39). However neither exact mechanism of aspirin resistance and PLA2 polymorphism is clear nor to what extent actions of aspirin influenced by glycoprotein IIb/IIIa polymorphism contribute to the clinical efficacy of the drug and to resistance to its actions is known (40,41). Another important integrin Gp Ia/IIa collagen receptor normally expressed on the platelet surface in low density and wide inter-subject variations. Collagen is physiologically important activating agent of platelet aggregation and increased density of platelet Gp Ia/IIa receptor could represent a potential thrombogenic risk factors contributing to aspirin resistance. Polymorphism within Gp Ia/IIa at position 807T (873A), results in altered response to collagen. Genetic variation or polymorphisms can determine if an individual will experience an altered clinical effect. However, data demonstrating the link between platelet polymorphism and anti-platelet drug therapy are limited. Prospective studies for the presence of various polymorphisms of larger and more diverse populations of patients need to be conducted. Factor XIII (FXIII) has a vital role in the coagulation process. Its transglutaminase activity, FXIII cross links fibrin monomers and thus clots enhanced mechanical strength and become more resistance to fibrinolysis (42). Recently a common polymorphism affecting the A-side chain of the FXIII (Val34Leu) has been identified to associate with thrombotic disorder. Surprisingly the less frequent allele (Leu34) doesn’t increase the risk of thrombosis, but described as being protective factor against myocardial infraction (43). Apart from above described polymorphism, aspirin resistance is significantly associated with genetic variation in the platelet surface adenosine 5-diphosphate receptor gene P2Y1 (44). The association of the polymorphism in ADP receptor gene is nearly three fold, thus increases the risk of aspirin resistance. ADP-stimulated platelet activation and aggregation is mediated by P2Y1 and P2Y12 receptors. Inhibitions of either receptor leads to significant decreases in shear-induced platelet aggregation by downstream events from the platelet glycoprotein –Ib1X- von Willebrand factor interaction (45, 46). Research has shown functional changes in the P2Y1 receptor may play a significant role in altering the function of ADP signaling and lead to prothrombotic changes and a decrease responsiveness to aspirin and other agents including P2Y12 inhibitors such as ticlopidine and clopidogrel. Clinically these changes may lead to phenotypic resistance to these anti-thrombotics.
PHS 398/2590(Rev. 09/04) Page - 43 - Menon Palat Krishna
Overall all identified genetic factors and polymorphism for platelet mechanism can be summarized as polymorphism of Cyclooxygenase-1 (COX-1) Gene COX1 (C50T), over expression of COX-2 mRNA on platelets and endothelial Cells COX-2 (G75C), fibrinogen receptor platelet glycoprotein (GP) IIb/IIIa (Pro33Leu), polymorphism of 807 C/T (873 G/A) Gene, platelet collagen receptor GP Ia/IIa (C807T) and FXIII (Val34Leu) etc. (47). Studies have been reported COX1 polymorphism, COX2 polymorphism, GP IIIa PIA Polymorphism, FXIII polymorphism and Platelet collagen receptor GP Ia/IIa (C807T) to understand the aspects of drug resistance. In the present research proposal attempts has been made to understand and in depth study of all the descried polymorphism by various approaches including common PCR and RFLP and microarray.
Aspects of Gene Expression in Platelet
Platelets are derived from megakaryoctes bone marrow cells, retain megakaryocyte-derived mRNA. They are enucleate and lack nuclear DNA but retain cytoplasmic mRNA and maintain functionally intact protein translation. Also in absence of mRNA organelles like, rough endoplasmic reticulum and polyribosome retain the ability for protein synthesis. It is demonstrated that 89 % of transcripts of platelet are mitochondrial (mt) which are enriched in 16S and 12S ribosomal RNAs presumably related to persistent mt-transcription is the absence of nuclear derived transcripts (48). Also recent findings shows platelet unexpectedly processes a functional spliceosome, a complex that processes pre m-RNAs in nuclei of other cell types. Primarily platelets also contain essential splisosome factors including small nuclear RNAs, splicing proteins, and endogenous pre mRNAs. In response to integrin engagement and surface receptor activation platelets precisely excise introns yielding mature messages that is translated to protein. Thus functional spliceosomal components are distributed to platelets during thrombopoiesis and that splicing can proceed in response to outside-in signals in an environment that is devoid of direct nuclear regulation and transcription (49). Thus apart from genetic alternation in platelet physiology, determination of platelet mRNA profiles in aspirin resistance group may establish a biological signature validating the clinical syndrome of aspirin resistance, which simultaneously can provide genetic markers of aspirin non-responsiveness. Also identification of differentially expressed transcripts may identify alternative targets for platelet inhibition unrelated to thromoboxane A2 pathway.
Clopidogrel Pharmacology and Clopidogrel Resistance
Clopidogrel is a prodrug which needs to be metabolized in the liver to active metabolites, which irreversibly interact platelet ADP receptor P2Y12 on the platelet surface. By blocking this receptor, clopidogrel interferes with platelet activation, degranulation and by inhibiting the modification of the glycoprotein IIb/IIIa receptor-aggregation. Polymorphism in P2Y12 is a risk for ischemic cerebrovascular events in patients with peripheral disease (50)
PHS 398/2590(Rev. 09/04) Page - 44 - Menon Palat Krishna
(Platelet Activity is affected by multiple factors, 51) Needless to say, the aforementioned general pitfalls of platelet aggregation applies not only to studies on aspirin resistance, but also to those of clopidogrel resistance. The possible mechanism for clopidogrel resistance could be extrinsic mechanisms; inappropriate dosing or under dosing, drug-drug interactions, including a possible interaction between clopidogrel and atharvostatin. (52, 53, 54). This is also reported that there is a positive correlation of clopidogrel response with CYP3A4 activity suggesting that an important mechanism may be variable conversion to the active metabolites (55). Other potential extrinsic mechanism could include variable conversion of the prodrug or clearance of the active metabolites. Intrinsic mechanisms could include P2Y12 receptor variability, increase in number of receptors, increased release of ADP or up-regulation of other platelet activation pathways. Few evidence shows inter-individual variability in platelet inhibitions by clopidogrel correlated well with the metabolic activity of the hepatic cytochorome 450, which activates the prodrug to its active metabolites. (56). Whether polymorphisms of the clopidogrel target P2Y12 and CYP3As plays additional roles in modulating the individual response is yet to discover.
In summary, the studies presented in this background section clearly document.
1. Aspirin and/or clopidogrel resistance is clearly an issue in diabetics and cardiovascular patient population. According to published reports non responders to aspirin or clopidogrel are at higher risk for acute coronary and cerebrovascular events.
2. Genetic polymorphism is one of the major contributors for aspirin resistance and/or clopidogrel resistance.
3. Environmental effect and gene expression profile along with polymorphism pattern in platelet couldn’t be neglected as a contributor for drug resistance.
PHS 398/2590(Rev. 09/04) Page - 45 - Menon Palat Krishna
C. PRELIMINARY STUDY
Studies from our laboratory for the first time demonstrated that one could induce drug- mediated resistance in platelets to the action of aspirin (58). In this study, the subjects were given a short acting inhibitor of COX-1, Ibuprofen. This was followed by administration of a full strength (325mg) aspirin. Ibuprofen-mediated inhibition of COX-1 enzyme lasts for a short time, whereas, aspirin induced inhibition is irreversible. Ibuprofen treated platelets recovered their sensitivity to the action of AA by 24 hrs. Whereas, aspirin treated platelets failed to respond to the action of AA even after 24 hrs. In those subjects who had ingested aspirin after taking Ibuprofen first, aspirin failed to inhibit irreversibly the COX-1; suggesting Ibuprofen molecules effectively prevented the acetylation of COX-1enzyme by aspirin. One of the earliest work describing “non-responders” and “responders” evaluated the effect of low dose aspirin and a thromboxane synthetase inhibitor dazoxiben (UK3724B) in healthy subjects (57). These studies demonstrated that low dose aspirin and ingestion of two dazoxiben tablets prevented the release of granules from platelets in response to AA in some individuals (responders) and not in others (non-responders). These subtle differences in response of platelets to various drugs as well as differences in response to various agonists may be critical when considering the outcome of acute vascular events. For instance, collagen seems to exert its effect by multiple mechanisms. In a study, using aspirin, monoclonal antibodies to IIb/IIIa receptor and fibrinogen, it was demonstrated that there exists at least three mechanisms by which collagen activates platelets; 1) GPIIb/IIIa associated activation, 2) prostaglandin dependent pathway, 3) alternate pathway responsible for 20-30 % platelet aggregation.
Several recent studies have demonstrated drug resistance in patients with a variety of vascular diseases (60-100). This subject currently is a very hot topic and has made national headlines. Andrew Pollack published an article in July of 2004 in New York Times, on this subject titled, “For Some, Aspirin May Not Help Hearts” (59). According to this article, 5-40% of aspirin users are “non-responders” or “resistant” to the drug. In the same article, he cites the opinion of Dr. Daniel I. Simon, the associate director of interventional cardiology at Brigham and Women’s Hospital, Boston, which reads as follows: “They are taking it for stroke and heart attack prevention and it’s not going to work”. He also reports the opinion of Dr. Michael J. Domanski; head of clinical trials unit at the NIH, in his opinion, the non-responders may represent a huge number of patients. According to Dr. Deepak L. Bhatt, director of interventional cardiology Cleveland Clinic, aspirin resistance is associated with worst outcome. Professor Eric Topol, Chairman, Cardiovascular Medicine Cleveland Clinic, USA states, “Aspirin resistance carries high risk, with over 20 million Americans taking aspirin to prevent heart attacks or strokes, it is important that further work to be done to confirm our findings and develop a rapid detection method. He also assures that for individuals with aspirin resistance, there are excellent alternatives”.
The first and foremost need at this time is to standardize a definition of aspirin resistance. The mechanism of action of aspirin is very well documented (7-13). The drug acetylates the platelet COX1 enzyme and irreversibly inhibits its ability to convert AA to PG endoperoxides (12, 13). In the absence of COX1 enzyme activity, platelets do not respond to AA stimulation with aggregation. Weak agonists such as ADP, Epinephrine depend on the formation of PG endoperoxides to initiate secondary wave of aggregation and promote release of platelet granule contents (3). Therefore, weak agonists fail to induce platelet aggregation and release granules from aspirin-treated platelets. Failure of AA, ADP and Epinephrine to
PHS 398/2590(Rev. 09/04) Page - 46 - Menon Palat Krishna
cause aggregation of platelets more or less establishes drug-induced platelet dysfunction. If platelets obtained from individuals who have ingested a full strength aspirin, respond with aggregation to the action AA, ADP and EPI, and release their granule contents, then one can safely conclude that these platelets are resistant to aspirin action. Further proof for aspirin resistance of platelets can be provided by studying AA metabolism by such platelets, monitoring serum TXB2 levels, or urinary levels of TXB2 or its metabolite, 11-dehydro-TXB2. Methods are available to monitor all these parameters. According to Cattaneo, “aspirin resistant” should be considered as description for those individuals whom aspirin fails to inhibit thromboxane A2 production, irrespective of the results of unspecific tests of platelet function (92).
In spite of the fact that several attempts have been made to explain the mechanisms involved in aspirin resistance, there exists no clear explanation. Studies should be initiated immediately to explore the mechanism by which an individual develops resistance to these drugs. Since platelets lack DNA, it is highly unlikely that these cells re-synthesize COX1 enzyme. Since many of these patients are on long-term aspirin therapy the effect of aspirin on megakaryocytes should be further explored. Platelets are formed from megakaryocytes and these cells do have DNA, hence studies are warranted to explore the effect of aspirin on bone marrow megakaryocytes. Majority of patients with vascular disease also will be taking many other drugs. As such, some amount of drug-drug interaction cannot be ruled out. Whatever may be the mechanism by which individuals with vascular disease develop resistance to aspirin, a better understanding of the molecular mechanisms involved will facilitate the development of appropriate therapeutic regimen.
In view of these observations, we have initiated a multi centered screening to determine prevalence of aspirin and clopidogrel resistance in normal healthy individual, well characterized diabetic (type-2) subjects and post MI-patients. The screening of high risk individuals will be conducted at Manipal Hospitals, Sri Jayadeva Institute of Cardiology, Mahavir Jain Hospital, Bangalore; MAKH, CRC, Manipal and at PSG Medical College and Hospitals, Coimbatore.
We hope that by the time we get NIH funding we will have some preliminary data on prevalence of drug resistance in normal subjects and patients suffering from diabetes and vascular diseases.
D. RESEARCH DESIGN AND METHODS
Pharmacogenomics and expression study comparison in Aspirin and/or Clopidogrel resistance: Human Studies. The overall goals of this proposal are to enhance our understanding of the detail mechanisms involved in aspirin and/or clopidogrel resistance in majority of patient population. We postulate not only polymorphism but alter gene expression involvement in those found resistant to the action of aspirin. Aspirin and/or clopidogrel responder or nor responder observed in individuals will:
a) be distinguished and sub grouped by their response to aspirin and clopidogrel, which will be measured by platelet aggregometry assay.
PHS 398/2590(Rev. 09/04) Page - 47 - Menon Palat Krishna
b) be confirmed of the respective drug resistance by studying metabolites. e.g urinary metabolites 11-dihydrothromboxane B2(TXB2) for aspirin resistance.
c) be studied for polymorphism for various genes involved in aspirin metabolic pathway as well as clopidogrel drug metabolic pathway.
d) be studied for gene expression profile between responder and non responders of aspirin and/or clopidogrel using designed oligo chips.
The current proposed study will identify causes for aspirin and/or clopidogrel resistance and it will open new era for correlation between polymorphism and gene expression pattern in those drug resistance population.
Study Feasibility:
The proposed multi center study will primarily utilize the blood obtained from the participating healthy volunteers and patient population (diabetics and post MI) under aspirin and/or clopidogrel treatment at multidisciplinary study centers (SJIC, Bangalore, Bhagawan Mahavir Heart Center Bangalore, CRC Manipal and Cardiology Division, PSG College, Coimbatore). All subjects participating in the study will sign an approved consent form. Screening for aspirin and/or clopidogrel resistance will be conducted at all the above mentioned centers. Patient population will be accessible from various collaborated hospital for study purposes. After preliminary screening for drug resistance, urinary metabolites and clopidogrel metabolites from the screened patients will be studied at Manipal Acunova, Clinical research center, Manipal. Once true aspirin and/or clopidogrel resistance population are screened, polymorphisms and gene expression study will be conducted at Manipal Acunova, Bangalore. Overall work and work progress will be supervised by Dr. Gundu H. Rao, Professor, Lillehei Heart Institute, University of Minnesota.
Description of Aspirin resistance and clopidogrel resistance patients and control subjects: Since aspirin and clopidogrel metabolism and drug physiology is not common in many settings, to improve uniformity in the study population, only patients under aspirin or clopidogrel therapy with knowledge of the patient history and drug effects, date of initial exposure will be included in the study. Patients (ages 21-60) will be included in this study. Detail inclusion criteria and exclusion criteria are given in section “E”. Healthy Volunteers (control population) participating in the study will be on no medications. All control subjects who are age (within 2 years), gender matched to each aspirin or clopidogrel resistant patients will be recruited from the medical center for sample (blood) collection at surrounding community by Dr. Manjunath, Dr. Ramesh, Dr. Keshava, Dr. S. Vidyasagar and Dr Bhuvaneswarn. Measurements obtained from healthy volunteers would provide the control base-line values.
The impact of aspirin and clopidogrel, resistance to the drug will be examined using the following study groups: i) Patients under aspirin treatments (n = 3000, each center will screen 1000). ii) Patients under clopidogrel treatment (n = 3000, each center will screen 1000). iii) Screened patients for aspirin non responder (n = 150). iv) Screen patients for clopidogrel non responder (n = 150).
PHS 398/2590(Rev. 09/04) Page - 48 - Menon Palat Krishna
v) Screen patients for both aspirin and clopidogrel non responder (n = 150) vi) Age/sex matched healthy volunteers (n = 500).
A total of 3000 patients will be evaluated in this study over a period of 1 year. The proposed size of the patient population in first two group (n = 3000) has 90% power to detect either or both aspirin and clopidogrel resistance. Importantly, due to the large patient population under aspirin and /or clopidogrel treatment accessible to all the study centers screening of 3000 patients over the study period and 500 healthy volunteers is not going to be a limiting factor. YEAR 0 1 2 Specific Aim 1 ------ Specific Aim 2 ------ Specific Aim 3 ------ Specific Aim 4 ------ Specific Aim 5 ------
Specific Aim 1: To determine prevalence of aspirin resistance in healthy population by platelet aggregation.
Hypothesis: Published reports indicate that aspirin resistance is a phenomenon observed mostly in patient population. However, we have included healthy population in this study to determine the prevalence of drug resistance in normal populations.
Experimental Design Healthy volunteers will be given aspirin 325 mg per day. Presence or absence of aspirin resistance will be determined by ex-vivo method. Blood for these studies will be obtained from normal adult volunteers with informed consent. Blood will be collected by venipuncture from healthy donors and patients after informed consent in accordance with the committee on Human Subjects Protection. The blood samples will be mixed immediately with Citrate-Citric acid, PH 6.5 (93mM sodium citrate, 70mM citric acid, and 140mM dextrose) in a ratio of nine parts blood to one part of anticoagulant. Platelet aggregation studies will be carried out on a Chronolog (Chronolog Corporation, Havertown, PA) whole blood aggregometer. Platelet aggregability will also be checked with ADP, collagen, epinephrine, restocetin, and PAF. Platelets will be stimulated by arachidonic acid (AA) as agonist to determine the specificity of aspirin resistance. Drug resistance will be defined as lack of inhibitory effect of the drugs on the target enzyme. If individuals taking aspirin respond with aggregation to the action of AA, then those individuals are considered non-responders. Those found to be resistant to the action of aspirin will be further evaluated for specificity by measuring metabolites of thromboxane.
Anticipated results and problems Subjects not meeting following criteria’s will be excluded. Patients on other antiplatelet drugs, other drugs containing aspirin therapy and on anti coagulants. Patients who are allergic/intolerant to aspirin and/or clopidogrel
PHS 398/2590(Rev. 09/04) Page - 49 - Menon Palat Krishna
Patients in whom aspirin and/or clopidogrel is contraindicated Patients with history of bleeding disorders, thrombocytopenia, liver or renal diseases.
Specific Aim 2: To determine prevalence of clopidogrel resistance in healthy population by aggregometry studies.
Hypothesis: Aspirin, is the most cost effective, which is used of 1st line anti-platelet cardiovascular diseases. However it blocks only one pathway (TXA2) of platelet activation. Blood platelets interact with a variety of soluble agonists such as epinephrine (EPI), adenosine diphosphate (ADP), thrombin and thromboxane (TXA2); many cell matrix components, including collagen, laminin, fibronectin, and vonWillebrand factor and biomaterials used for construction of invasive medical devices Clopidogrel works as anti-platelet agent by blocking ADP receptor. In recent years increasing number of patients use clopidogrel for secondary prevention of cardiovascular events. Therefore resistance to clopidogrel is also of major concern. Before initiating studies on the concept and mechanism for clopidogrel resistance in patient population, it is highly important to check whether the healthy population develops resistance to clopidogrel.
Experimental Design
Blood for these studies will be obtained from normal adult volunteers with informed consent. Blood will be collected by venipuncture from healthy donors and patients (75 mg of clopidogrel has taken previous day) after informed consent in accordance with the committee on Human Subjects Protection. The blood samples will be mixed immediately with Citrate-Citric acid, PH 6.5 (93mM sodium citrate, 70mM citric acid, and 140mM dextrose) in a ratio of nine parts blood to one part of anticoagulant. Platelet aggregation studies will be carried out on a Chronolog (Chronolog Corporation, Havertown, PA) whole blood aggregometer. Drug resistance will be defined as lack of inhibitory effect of the drugs on the target receptor. If individuals taking clopidogrel respond with aggregation, then those individuals are considered non-responders.
Specific Aim 3: To determine the prevalence of aspirin and/or clopidogrel resistance in patients (Diabetics and post MI).
Hypothesis: Prevalence of drug resistance in patient population and the mechanism for drug resistance. Concept of drug resistance is major concern for both aspirin and clopidogrel. Various factor like bioavailability, platelet function, single nucleotide polymorphisms, platelet interactions with other blood cells and many more, could potentially contribute for those drug resistances. Therefore, it is essential to find out the prevalence of true drug resistance before starting studies on mechanism behind drug resistance.
Experimental Design
3000 diabetics and post MI patients who are receiving different doses of aspirin at 3 different study centers will be subjected to aggregation test. Patients will be given 325 mg of aspirin and after 30 minutes blood will be collected for aggregation study to check aspirin resistance. However 75 mg of clopidogrel will be given previous day and blood sample will be collected next day to check clopidogrel resistance by aggregation study. Blood for these studies will be obtained from patients with informed consent. Blood sample will be collected, processed and studied for drug resistance as described earlier in Specific aim 1. Drug resistance will be
PHS 398/2590(Rev. 09/04) Page - 50 - Menon Palat Krishna
defined as lack of inhibitory effect of the drugs on the target enzyme or target receptor. If individuals taking clopidogrel respond with aggregation, then those individuals will be considered non-responders.
Specific Aim 4: To study metabolites products (Urinary metabolites: 11- dehydrothromboxane B2) in order to confirm the patients are truly aspirin resistance and to study clopidogrel metabolites for confirmation of clopidogrel resistance.
Hypothesis: One of the possible explanations for the limited efficacy of aspirin may be the ability of platelets
to generate thromboxane A2 despite usual therapeutic doses of aspirin (101). The mechanism could be incomplete suppression of thromboxane generation with the usual dose of aspirin. We hypothesize that platelet aggregometry study may not be able to give a clear picture of true aspirin resistance. As aspirin works by stopping the production of thromboxane (TXA2), the
extent of inhibition of thromboxane A2 generation can be determined by measuring urinary
levels of 11-dehydro thromboxane B2, a stable metabolite of thromboxane A2.
Experimental Design Monitoring Metabolite of Thromboxane: Quantitative analysis of thromboxane production is useful as an index of pathological states and medical therapeutic effects. Quantitative methods require high sensitivity and selectivity because of the low concentration, short half-life time of the compounds. Urinary thromboxane also will be monitored using commercially available ELISA using manufacture’s instructions. Measurement of 11 dehdro-TXB2, major metabolites of TXB2, in plasma, is one of the approaches to the assessment of thromboxane formation in the circulation. Liquid chromatography/mass spectrometry (LC/MS) is a simple and rapid determination method. LC/MS is sufficiently applicable to determination of TXA2. Advanced determination method for 11-dehydro TXB2, a stable urinary metabolite of TXA2, using liquid chromatography/tandem mass spectrometry (LC/MS-MS) will be used as alternative method. In this study proposal urinary metabolites (TXA2) will be analyzed after preliminary screening for aspirin resistance at CRC, Manipal.
Specific Aim 5: To study gene polymorphism pattern in aspirin and clopidogrel responders and non responders.
Hypothesis: The role of genetic variation in drug response has become increasingly evident over the past decade. Genetic determinants for multifactorial diseases are poorly understood. Genetic variation may play a significant role in mediating aspirin resistance in different patients.
Experimental Design Polymorphism for various responsible genes will be studied according to methods described in literatures. Polymorphism of Cyclooxygenase-1 (COX-1) Gene COX1 (C50T) Over expression of COX-2 mRNA on Platelets and Endothelial Cells COX-2 (G75C) Fibrinogen receptor platelet glycoprotein (GP) IIb/IIIa (Pro33Leu) Polymorphism of 807 C/T (873 G/A) Gene Platelet collagen receptor GP Ia/IIa (C807T) Gene polymorphism of FXIII (Val34Leu) Gene polymorphism P2Y12 H1/H2 Attempts has been made to understand and conducting in depth study of all the above descried polymorphism by conventional PCR and RFLP and microarray.
PHS 398/2590(Rev. 09/04) Page - 51 - Menon Palat Krishna
PCR and RFLP Determination of the Cox-1 C50T and Cox-2 G-765C genotypes will be performed by polymerase chain reaction–allelic restriction assays with Fau-I (Fermentas, Pascual and Furió) and single-stranded conformational polymorphism, respectively, using specific primers COX1 polymorphism (102) Cox-1F: 5'GGTGCCCGGTGGGGAATTTTC3' Cox-1B: 5'GAGGGGAAAGGAGGGGGTTG 3' Restriction enzyme Fau-I COX2 polymorphism Cox-2F: 5'CCGCTTCCTTTGTCCATCAG3' Cox-2B: 5'GGCTGTATATCTGCTCTATATGC3' Restriction enzyme Fau-I GP IIIa PIA Polymorphism (103) FP: 5’ GCTCCAATGTACGGGGTAAAC 3’ and RP: 5’ GGGGACTGACTTGAGTGACCT 3’ Restriction enzyme Msp1 FXIII polymorphism(104) PCR of the FXIII exon 2 genes will be performed using 5’ GACCTTGTAAAGTCAAAAATGT 3’ 5’ TGGTGCCCCGGGGCGTCAACCTHCAAG 3’ (67-238 bp) The mutated reverse primer identifies the 214G/T (Val34Lec) polymorphism by restriction enzyme BsaHI. Platelet collagen receptor GP Ia/IIa (C807T) (will be standardized) Polymorphism for P2Y12 and CYP3 (will be standardized)
Specific Aim 5: To develop possible altered gene expression profile using designed oligo chips (30- 40 genes responsible for platelet activation as mentioned below and CYP450 gene family) probing with platelet RNA isolated from both aspirin and/or clopidogrel resistance and non resistance sub groups.
Hypothesis: Response to drug depends on multi factors. Non responsiveness to aspirin and clopidogrel can be results of various factors including genetic, environment, altered gene expression, individual response and many unknown factors. Major finding in molecular aspects of aspirin resistance are gene polymorphism. However we postulate altered gene expression for platelet physiology and aspirin metabolism as one of the major reason for developing non responsiveness to aspirin.
Experimental Design Attempt has been made to include maximum numbers of genes involve in platelet physiology, genes involved in drug metabolism. Candidate genes described below will be included in the custom made oligo chips.
COX1 NM_000962 prostaglandin-endoperoxide synthase 1 (prostaglandin G/H synthase and cyclooxygenase) (PTGS1) M59979 Human prostaglandin endoperoxide synthase mRNA, complete cds, mRNA ACCESSION M59979 NP_000953 PRI 03- prostaglandin-endoperoxide synthase 1 isoform 1 precursor
PHS 398/2590(Rev. 09/04) Page - 52 - Menon Palat Krishna
COX2 NM_000963 prostaglandin-endoperoxide synthase 2 (prostaglandin G/H synthase and cyclooxygenase) (PTGS2), mRNA AY462100.1 Homo sapiens cyclooxygenase 2 (COX2) mRNA, complete cds M90100.1 Homo sapiens cyclooxygenase-2 (Cox-2) mRNA, complete cds AY151286.1 complete cds Homo sapiens cyclooxygenase 2b mRNA, complete cds; alternatively spliced L15326.1 Human endoperoxide synthase type II mRNA, complete cds
Glycoprotein Hs.272216 GP6: Glycoprotein VI (platelet) Homo sapiens, 41 sequence(s) Hs.411312 TGA2B: Integrin, alpha 2b (platelet glycoprotein IIb of IIb/IIIa complex, antigen CD41B) Homo sapiens, 41 sequence(s) Hs.517410I GP1BB: Glycoprotein Ib (platelet), beta polypeptide Homo sapiens, 97 sequence(s) Hs.218040 ITGB3: Integrin, beta 3 (platelet glycoprotein IIIa, antigen CD61) Homo sapiens, 146 sequence(s) Mm.248662GP9: Glycoprotein IX (platelet), Homo sapiens, 15 sequence(s) Hs.73734 GP5: Glycoprotein V (platelet), Homo sapiens, 7 sequence(s) Hs.1472 GP1BA: Glycoprotein Ib (platelet), alpha polypeptide Homo sapiens, 11 sequence(s) Str.28675 ranscribed locus, moderately similar to NP_000203.2 integrin beta chain, beta 3 precursor; platelet glycoprotein IIIa precursor [Homo sapiens] Hs.120949 CD36: CD36 antigen (collagen type I receptor, thrombospondin receptor) Homo sapiens, 539 sequence(s)
Glycogen Receptor Hs.120949 CD36: CD36 antigen (collagen type I receptor, thrombospondin receptor) Homo sapiens, 539 sequence(s) Cfa.14070 Transcribed locus, strongly similar to XP_546326.1 PREDICTED: similar to Integrin alpha-2 precursor (Platelet membrane glycoprotein Ia) (GPIa) (Collagen receptor) (VLA-2 alpha chain) (CD49b) [Canis familiaris] Canis familiaris, 2 sequence(s) Hs.30868 RTN4R: Reticulon 4 receptor, Homo sapiens, 125 sequence(s)
Thromboxane pathway Hs.520757 BXAS1: Thromboxane A synthase 1 (platelet, cytochrome P450, family 5, subfamily A) Homo sapiens, 212 sequence(s) Hs.442530 TBXA2R: Thromboxane A2 receptor Homo sapiens, 26 sequence(s) Cfa.21720 Transcribed locus, strongly similar to XP_539887.1 PREDICTED: similar to thromboxane-A synthase (EC 5.3.99.5) - human [Canis familiaris] Hs.552136 Transcribed locus, weakly similar to NP_963998.1 thromboxane A2 receptor isoform 2 [Homo sapiens] NM_001060 Homo sapiens thromboxane A2 receptor (TBXA2R), transcript variant 2, mRNA |NM_201636Homo sapiens thromboxane A2 receptor (TBXA2R), transcript variant 1, mRNA
PAR PKC Phospholipase 2A
PHS 398/2590(Rev. 09/04) Page - 53 - Menon Palat Krishna
Hs.554780 PLA2G7: Phospholipase A2, group VII (platelet-activating factor acetylhydrolase, plasma) Homo sapiens, Hs.466804 PLA2G2A: Phospholipase A2, group IIA (platelets, synovial fluid) Homo sapiens, BC038452 Homo sapiens phospholipase A2, group VII (platelet-activating factor acetylhydrolase, plasma), mRNA (cDNA clone MGC:46165 IMAGE:5216829), complete cds
Collagen Hs.553794 MGC34774: Platelet receptor for type III collagen, 47 kDa Homo sapiens, 82 sequence(s) Hs.120949 CD36: CD36 antigen (collagen type I receptor, thrombospondin receptor) Hs.172844 Non-integrin platelet receptor for type I collagen NM_000212 Homo sapiens integrin, beta 3 (platelet glycoprotein IIIa, antigen CD61) (ITGB3), mRNA
ADP AJ320495.1 Homo sapiens mRNA for platelet ADP-receptor (P2Y12 gene) AF313449.1 Homo sapiens P2Y12 platelet ADP receptor mRNA, complete cds AY275466.1 Homo sapiens platelet-activating factor receptor (PTAFR) mRNA, complete cds
Collagen Receptor AY339211 Homo sapiens non-integrin platelet receptor for type I collagen mRNA, complete cds NM_000072Homo sapiens CD36 antigen (collagen type I receptor, thrombospondin receptor) (CD36), transcript variant 3, mRNA NM_001001548 Homo sapiens CD36 antigen (collagen type I receptor, thrombospondin receptor) (CD36), transcript variant 1, mRNA AY339211 Homo sapiens non-integrin platelet receptor for type I collagen mRNA, complete cds M59911 Human integrin alpha-3 chain mRNA, complete cds X17033 Human mRNA for integrin alpha-2 subunit NM_000552 Homo sapiens von Willebrand factor (VWF), mRNA NM_002211 Homo sapiens integrin, beta 1 (fibronectin receptor, beta polypeptide, antigen CD29 includes MDF2, MSK12) (ITGB1), transcript variant 1A, mRNA (transcript variant 1B and 1C also available) NM_000088 Homo sapiens collagen, type I, alpha 1 (COL1A1), mRNA
Thromosis/ Fibrinolysis/ Platlet Fuctions Hs.75599 SERPINC1: Serine (or cysteine) proteinase inhibitor, clade C (antithrombin), member 1 Homo sapiens, 171 sequence(s) Hs.335513 F13A1: Coagulation factor XIII, A1 polypeptide Homo sapiens, 334 sequence(s) Hs.351593 FGA: Fibrinogen alpha chain Hs.300774 FGB: Fibrinogen beta chain Hs.546255 FGG: Fibrinogen gamma chain Hs.529161Alpha-1-B glycoprotein Hs.516578 TFPI: Tissue factor pathway inhibitor (lipoprotein-associated coagulation inhibitor) Hs.38449 SERPINE2: Serine (or cysteine) proteinase inhibitor, clade E (nexin, plasminogen activator inhibitor type 1), member 2 Hs.491582 PLAT: Plasminogen activator, tissue Hs.218040 ITGB3: Integrin, beta 3 (platelet glycoprotein IIIa, antigen CD61) Hs.224698 PROC: Protein C (inactivator of coagulation factors Va and VIIIa) Hs.64016 PROS1: Protein S (alpha)
PHS 398/2590(Rev. 09/04) Page - 54 - Menon Palat Krishna
Hs.36989 F7: Coagulation factor VII (serum prothrombin conversion accelerator) Hs.554780 PLA2G7: Phospholipase A2, group VII (platelet-activating factor acetylhydrolase, plasma) Hs.302085 PTGIS: Prostaglandin I2 (prostacyclin) synthase Hs.82353 PROCR: Protein C receptor, endothelial (EPCR) Hs.510334 SERPINA5: Serine (or cysteine) proteinase inhibitor, clade A (alpha-1 antiproteinase, antitrypsin), member 5 Hs.510334 SERPINA5: Serine (or cysteine) proteinase inhibitor, clade A (alpha-1 antiproteinase, antitrypsin), member 5 Hs.546538 CRB2: Crumbs homolog 2 (Drosophila)
CYP 450 Another very important gene family to consider in the proposed studies is Cytochrome P450, the drug metabolizing enzymes, which metaboilize cholesterol, steroids and other important lipids such as prostacyclins and thromboxane A2. Prostacyclins and thromboxane A2 are metabolites of arachidonic acid. Studies show mutations in cytochrome P450 genes or deficiencies of these drug metabolizing enzymes are responsible for several human diseases. P450 enzymes play a major role in drug metabolism as well as drug interactions. However, it will be interesting to study the expression of cyp450 family and their role in aspirin resistance to determine if non-responders to aspirin develop resistance because of gene mutations or impaired functions or high turnover of hydrolyzing enzymes.
The proposed study is focusing on factors such as genetic and gene expression variabilities responsible for aspirin and/or clopidogrel resistance. However other mechanism such as transcellular metabolism, inducible COX-2 in platelets, inducible COX-2 transporting arachidonic acid metabolites to platelets etc can be considered as alternative resistance mechanism.
E: Human Subject Research:
Aspirin is the most useful and cost-effective drug for secondary prophylaxis of vascular disease. Large number of clinical trials using aspirin has concluded that for any given vascular risk, low to medium dose of aspirin (80-160mg), is as effective as any other drug of choice. Next to aspirin clopidogrel is the choice of drug for vascular diseases. However, in recent years, there are several studies, in which aspirin resistance and clopidogrel resistance in patients with various vascular diseases have been demonstrated specially in patient population. We will conduct the study in both healthy and patient population to understand the underlying mechanism behind observed drug resistance in patient population. We have applied for the study approval to IRB (institutional review board) for each study centers and ICMR (Indian council of medical research). We have got approval for 2 study centers and expect to get the approval from ICMR by the time founding comes for the study.
Patients (ages 21-60) irrespective to genders, will be included in this study if they meet the following Inclusion criteria: 1. Healthy volunteers for control subjects without any record of diabetes and post MI. 2. Diabetic and/or post MI patients who are under aspirin for secondary prophylaxis.
PHS 398/2590(Rev. 09/04) Page - 55 - Menon Palat Krishna
Exclusion criteria: 1. Patients on other anti-platelet drugs, other drugs containing aspirin and or anti coagulants. 2. Patients who are allergic/intolerant to aspirin and/or clopidogrel 3. Patients in whom aspirin and/or clopidogrel is contraindicated 4. Patients with history of bleeding disorders, thrombocytopenia, liver or renal diseases.
H. Literature cited:
1. Sherry S, Scriabine A. Platelets and Thrombosis. University Press, USA 1999. P.309 2. Suldow C, Baigent C. Randomized Trials of Antiplatelet Therapy. Handbook of Platelet Physiology and Pharmacology. Rao GHR, (ed) Kluwer Academic Publishers, USA1999, p526-549. 3. Rao GHR, Rao AT. Pharmacology of Platelet Inhibitory Drugs. Ind. J. Physiol.19994, 38:69-84. 4. Rao GHR, Rao ASC, White JG. Aspirin in Ischemic Heart Disease-an overview. Ind. Heart J.1993, 45: 73-79. 5. Rao GHR. Aspirin and Coronary Artery Disease: Coronary Artery Disease in South Asians: Epidemiology, Risk Factors and Prevention. Rao GHR, Kakkar VV(eds), Jaypee Medical Publishers, India, 2001, p263-278. 6. Weisman G. Aspirin. Sci Am.1991, 264: 84-91. 7. Vane JR. Inhibition of prostaglandin synthesis as a mechanism of action of aspirin-like drugs. Nature 1971, 231: 232-235. 8. Vane JR, Flower RJ, Botting RM. History of aspirin and its mechanism of action. Stroke 1990, 21: IV-12. 9. Ferreira SH, Vane JR. Newer aspects of the mode of action of non-steroidal anti-inflammatory drugs. Ann. Rev. Pharmacol. 1974, 14: 57-73. 10. Hamberg M, Svensson J, Samuelsson B: Thromboxanes: A new group of biologically active compounds derived from prostaglandin endoperoxides. Proc. Natl. Acad Sci. 1975, 72: 2994-2998. 11. Marcus AJ. Aspirin as an anti-thrombotic medication. N. Engl. J. Med. 1983, 309: 1515-1517 12. Roth JG, Caverley DC. Aspirin, Platelets and Thrombosis: Theory and Practice. Blood 1994, 83: 885-898. 13. Roth JG: Stanford N, Majerus PW. Acetylation of prostaglandin synthetase by aspirin. Proc. Natl. Acad. Sci. 1975, 72: 3073-3076. 14. Meade EA, Smith WL, Dewitt DL: Differential inhibition of prostaglandin endoperoxide syhthase (cyclooxygenase) isoenzymes by aspirin and other non-steroidal anti-inflammatory drugs. J. Biol. Chem. 1993, 268: 6610-6614. 15. Burch JW, Stanford N, Majerus PW. Inhibition of platelets prostaglandin synthetase by oral aspirin. J. Clin. Invest 1978: 61: 314-319. 16. Reilly IA, FitzGerald GA. Aspirin in Cardiovascular Disease. Drugs 1988, 35: 154-176. 17. Wilson KM, Siebert DM, Duncan EM. et al. Effect of aspirin infusions on platelet function in humans. Clin. Sci. 1990, 79: 37-42. 18. McLeod LJ, Roberts MS, Cossum PA. et al. The effects of different doses of some acetyl salicylic acid formulations on platelet function and bleeding times in healthy subjects. J. Haematol. 1986, 36: 379-384. 19. Masptti G, Galanti G, Pogessi L. Differential inhibition of prostacyclin production and platelet aggregation by aspirin. Lancet 1972, 2:11213-1216. 20. Steering Committee of the Physicians Health Study Research Group. Preliminary Report: Findings from the aspirin component of the ongoing physicians’ health study. N. Engl. J. Med. 1988, 318: 262-264. 21. Steering Committee of the Physicians Health Study Research Group. Final Report. N. Engl. J. Med. 1989, 321: 129-135. 22. Hallam TJ, Sanchez A, Rink TJ. Stimulus response coupling in Platelets. Biochem J. 1984, 218:819-827. 23. Zucker MB Nachmias VT. Platelet Activation. Arteriosclerosis. 1985, 5:2-18. 24. Edridge MJ. The molecular basis of communication within the cells. Sci. Am 1985, 253:142-152. 25. Holmsen H. Platelet metabolism and activation. Semin Hematol. 1985, 22:219-240.
PHS 398/2590(Rev. 09/04) Page - 56 - Menon Palat Krishna
26. Seiss W. Molecular mechanism of platelet activation. Physiol. Rev.1990, 70:115-164. 27. Rao, GHR. Physiology of blood platelet activation. Ind J Physiol Pharmacol. 1993, 37:263-275. 28. Rao, GHR. Signal transduction, second messengers and platelet function. J Lab Clin Med. 1993, 121:18-21. 29. Rao, GHR. Signal transduction, second messengers and platelet pharmacology. Pharmacol. 1994,13:39-44. 30. Packham MA. Role of platelets in thrombosis and hemostasis. Can J Physiol. Pharmacol. 1993, 72:278-284. 31. Martin, C et al. (2005): Aspirin Resistance: An evolution of current evidence and measurement methods.Pharmacotherapy. 25 (7):942-953 32. Singh S., Kothari SS. And Bhal VK.: Aspirin Resistance: Myth or Reality?. 2003, Vol 55, No. 3, 1-7 33. Valles J et al., (1998): Erythrocyte promotion of platelet reactivity decreases the effectiveness of aspirin as an antithrombotic therapeutic modality: the effect of low dose aspirin is less then optimal in patients with vascular disease due to prothrombotic effects of erythocytes on platelet reactivity. Circulations, 97:350-355. 34. Michelson AD et al.,(2005). Aspirin resistance: Position paper of the working group on aspirin resistance. J Thromb Haemost. Jun; 3(6):1309-11. 35. Cambria-Kiely J. A. and Gandhi P.J (2002): Aspirin resistance and genetic polymorphisms 36. Kuniki, TJ, Newman, PH. (1992): The molecular biology of human platelet proteins. Blood. 80:1396-1404. 37. Nuden, AT.(1997): Platelet glycoprotein IIIa polymorphism and coronary thrombosis. Lancet, 350:1189-1191. 38. Michalson et al (2000): Polymorphisms display different sensitivities to agaonists. Circulatiob,101: 1013-8. 39. Andrioli et al (2000): Defective platelet response to ariachidonic acid thromboxin A2 in subjects with PI (A2) polymorphism of beta (3) subunit (glycoprotein IIIa). Br J Haaematol, 110:911-8. 40. Gum P. A., Marchant K., Poggio E. D., Gurm H., Welsh P. A, Brooks L., Sapp S. K., Topol E. J. (2001) Profile and prevalence of aspirin resistance in patients with cardiovascular disease. The American Journal of cardiology, Vol 88, 230-235 41. Mckee SA, Sane DC and Deliargyris EN (2002): Aspirin resistance in cardiovascular disease: a review of prevalence, mechanism and clinical significance. Thromb Haemost., 88:711-715. 42. Carrol J., Gonzalez-Conejero, Iniesta J. A., Rivera J., Martinex C. and Vicente V (2000) The FXIII Val34Leu polymorphism in venous and arterial thromboembolism. Hematologica 85: 293-297 43. Kholor et al. Rao GHR, Radha E Johnson GJ. et al. Enteric coated aspirin, platelet cyclooxygenase activity and platelet function. Prost. Leukot. Med. 1984, 13: 3-12. 44. Jefferson B.K et al., Am J Cardiol. 2005 Mar 15; 95(6):805-8: Aspirin resistance and a single gene 45. Storey et al. (2001): Effects of P2Y (1) and P2Y (12) receptor antagonists on platelet aggregation induced by different agonists in human whole blood. Platelets 2001:12:443. 46. Leon C. et al (2003): Differential involvement of the P2Y1 and P2Y12 receptorsin platelet procoagulent activity. Arterioscler Thromb Vasc Biol. 23:1941-1947. 47. Tang Z. and Tracy R.P. 2001, Candidate genes and confirmed genetic polymorphisms associated with cardiovascular diseases: a tabular assessment. Journal of Thrombosis and Thrombolysis, Volume 11, Nov 1, pg 49-81. 48. Bahou, F. W. and Gnatenko, D. V. (2004): Platelet Transcriptome: The application of microarray analysis to platelets. Vol 30, Nov 4, 473-487 49. Denis M M et al. (2005): Escaping the nuclear confines: signal- dependent pre-mRNA splicing in anucleate platelets. Cell, Vol. 122, 379-391 50. Ziegler S et al. (2005): Association of a functional polymorphism in the clopidogrel target receptor gene, P2Y12, and the risk for Ichemic cerebrovascular events in patients with pheripheral artery diseaseStrok: 2005:36:1394. 51. Mayers R. (2005): The variability of platelet response to aspirin and clopidogrel: revisiting the CAPRIE, CURE, CREDO and MATCH trials. 18:331-336 52. Wiviotte S., and Antman M. (2004): Clopidogrel resistance, A new chapter in a fast moving story. June 29: 3064-3067. 53. Saw j et al (2003): Lack of adverse clopidogrel atrovastain clinical interaction from secondary analysis of a randamised, placebo-controlled clopidogrel trial. Circulation, 108:921-924. 54. Law WC et al (2003): Atrovastatin reduces the ability of clopidogrel to inhibit aggregation: a new drug-drug interaction. Circulation. 2003:107:32-37.
PHS 398/2590(Rev. 09/04) Page - 57 - Menon Palat Krishna
55. Nguyen TA, Diodati JG, Pharand C. Resistance Clopidogrel: a review of the evidence. J. Am Coll Cardiol 2005, 45: 1157-64. 56. Law WC.et al (2004): Contribution of hepatic cytochrome p450 3A4 metabolic activity to the phenomenon of clopidogrel resistance. Circulation. 2004:109:166-171 57. Jones EW, Cockbill SR, Cowley AJ. et al. Effects of dazoxiben and low-dose aspirin on platelet behavior in man. Brit. J. Pharmacol. 1983, 15: 395-445. 58. Rao GHR, Johnson GJ, Reddy KR. Ibuprofen Protects Platelet Cyclooxygenase from Irreversible Inhibition by Aspirin. Arteriosclerosis. 1983, 3: 383-388. 59. Pollack A. For Some, Aspirin May Not Help Hearts. New York Times. 2004, July. 60. Weber AA, Przytuski B, Schanz A. et al. Towards a definition of aspirin resistance: a typological approach. Platelets. 2002, 13: 37-40. 61. Yilmaz MB, Balbay Y, Korkmaz S. Aspirin resistance. Anadolu. Kardiyol. Derg 2004, 4: 59-62. 62. Patrono C, Coller B, FitzGerald GA. et al. Platelet-Active Drugs: The Relationships Among Dose, Effectiveness, and Side Effects. CHEST 2004, 126: 234S-264S. 63. Howard PA. Aspirin resistance. Ann Pharmacother. 2002, 36: 1620-1624. 64. Hurlen M, Seijeflot I, Arnesen. The Effect of Different Regimens on Platelet Aggregation After Myocardial Infarction. Scand. Cardiovasc. J. 1998, 32: 233-237. 65. Wu KK, Hoak JC. A new method for the quantitative detection of platelet aggregation in patients with arterial insufficiency. Lancet 1974,11: 924-926. 66. Gum PA, Kottke-Marchant K, Poggio ED. et al. Profile and prevalence of aspirin resistance in patients with cardiovascular disease. Am. J. Cardiol. 2001, 88: 230-235. 67. Gum PA, Kottke-Marchant K, Welsh PA. et al. A prospective, blinded determination of the natural history of aspirin resistance among stable patients with cardiovascular disease. J. Am. Coll. Cardiol. 2003, 41: 961- 967. 68. Deliargyris E, Boudoulas H. Aspirin Resistance. Hellenic J. Cardiol. 2004, 45: 1-5. 69. Grotemeyer KH. Effects of acetylsalicyclic acid in stroke patients; evidence of non-responders in a subpopulation of treated patients. Thromb. Res. 1991, 63: 587-593. 70. Grotemeyer KH. Two-year follow-up of aspirin responder and aspirin non-responder. A pilot-study including 180 post-stroke patients. Thromb. Res. 1993, 71:397-403. 71. Mueller MR, Salat A, Stangi P. et al. Variable platelet response to low-dose ASA and the risk of limb deterioration in patients submitted to peripheral arterial angioplasty. Thromb. Haemost. 1997, 78: 1003-1007. 72. Eikelboom JW, Hirsh J, Weitz JI. et al. Aspirin-resistant thromboxane biosynthesis and the risk of myocardial infarction, stroke, or cardiovascular death in patients at high risk for cardiovascular events. Circ 2002, 105: 1650-1655. 73. Smout J, Stansby G. Aspirin resistance. Brit. J. Surgery 2002, 89: 4-5. 74. Helgason CM, Bolin KM, Hoff JA. et al. Development of aspirin resistance in persons with previous ischemic stroke. Stroke 1994, 25: 2331-2336. 75. Zimmerman N, Wenk A, Kim U. et al. Functional and biochemical evaluation of platelet aspirin resistance after coronary artery bypass surgery. Circ. 2003, 108: 542-547. 76. Sane DC, McKee SA, Malinin AI. Frequency of aspirin resistance in patients with congestive heart failure treated with antecedent aspirin. Am. J. Cardiol. 2002, 90: 893-895. 77. Muller I, Besta F, Schulz C. et al. Prevalence of Clopidogrel non-responders among patients with stable angina pectoris scheduled for elective coronary stenting. Thromb. Heamost. 2003, 89: 783-787. 78. Angiolilo DJ, Fernandez-Ortiz A, Bernardo E. et al. High Clopidogrel loading dose during coronary stenting: effect on drug response and inter-individual variability. Eur. Heart J. 2004, 25: 1903-1910. 79. Serebruany VL, Steinhubl SR, Berger PB. et al. Variability in platelet responsiveness to Clopidogrel among 544 individuals. J. Am Coll. Cardiol. 2005, 45: 246-251. 80. Dziewierz A, Dubek D, Heba G. et al. Inter-individual variability in responses to Clopidogrel with cardiac diseases. Polis Heart J. 2005, 62: 1-6. 81. Altman R, Luciardi HL Muntaner J. et al. The anti-thrombotic profile of aspirin, aspirin resistance or simply failure? Thromb. J. 2004, 2: 1-8.
PHS 398/2590(Rev. 09/04) Page - 58 - Menon Palat Krishna
82. De Gaetano G, Cerletti C. Aspirin resistance: a revival of platelet aggregation tests? J. Thromb. Haemost. 2004, 1: 2048-2061. 83. Malinin A, Spergling M, Muhlestein B. et al. Assessing aspirin responsiveness in subjects with multiple risk factors for vascular disease with a rapid platelet function analyzer. Blood Coag. Fibrinol. 2004, 1%: 295-301. 84. Sambola A. Heras M, Escolar G. et al. The PFA-100 detects sub-optimal antiplatelet responses in patients on aspirin. Platelets. 2004, 1-8. 85. Feuring M, Hasseroth K, Janson CP. et al. Inhibition of platelet aggregation after intake of acetylsalicylic acid detected by a platelet function analyzer (PFA-100). Int. J. Clin Pharmacol Ther. 1999, 37: 584-548. 86. Andersen K, Hurlen M, Arnesen H. et al. Aspirin-responsiveness as measured by a PFA-100 in patients with coronary artery disease. Thromb. Res. 2002, 108: 37-42. 87. Singh S, Kothari SS, Bahl VK. Aspirin Resistance: Myth or Reality? Ind. Heart J. 2003, 55: 1-8 88. McKee SA, Sane DC, Deliagyris. Aspirin resistance in cardiovascular disease: A review of prevalence, mechanisms, and clinical significance. Thromb. Haemost. 2002, 88: 711-715. 89. Eikelboom JW, Hankey GJ. Aspirin resistance: a new independent predictor of vascular events? J. Am. Coll.Cardiol. 2003, 41: 966-968. 90. Berger PB. Resistance to antiplatelet drugs: Is it real or relevant? Cath. And Cardiovasc Interven. 2004, 62: 43-45. 91. Shemesh CG, zehavi M, Dinur I et al. Lack of aspirin effect: aspirin resistance or resistance to taking aspirin? Am. Heart J. 2004, 147: 293-300. 92. Cattaneo M. Aspirin and Clopidogrel: efficacy, safety, and the issue of drug resistance. Arterscler. Vasc. Biol. 2004, 24: 1980-87. 93. Sztritha LK Sas K, Vecsei L. Aspirin resistance in stroke: 2004. 2005, 230:163-69. 94. Coma-Canella I, Velasco A, Castano S. Prevalence of aspirin resistance measured by PFA-100. Int. J. Cardiol. 2005, 101:71-76. 95. Kuliczkowski W, Halawa B, Korolko B. Aspirin resistance in ischemic heart disease. Kardiol Pol. 2005, 62: 14-25. 96. Schwartz KA, Schwartz DE, Ghosheh K et al. Compliance as a critical consideration in patients who appear to be resistant to aspirin after healing of myocardial infarction. Am. J. Cardiol 2005, 95: 973-75. 97. Driewierz A, Dudek D, Heba G, Inter-individual variability in response to Clopidogrel in patients with coronary artery disease. Kardiol Pol. 2005, 62: 108-118. 98. Serebruaany VL, Steinhubl SR, Berger PB. et al. Variability in platelet responsiveness to Clopidogrel among 544 individuals. J Am Coll Cardiol. 2005 45: 246-51. 99. Rao GHR. Aspirin resistance: A fact or a myth? Expt. & Clin. Cardiol. 2005, 10: 17-20. 100. Pettersen AA, Seljeflot I, Abdelnoor M et al. Unstable angina, stroke, myocardial infarction and death in aspirin non-responders. A Prospective, randomized trial. The ASCET (Aspirin non-responsiveness and Clopidogrel Endpoint Trial) design. Scand Cardiovasc. J. 2004, 38:353-56. 101. Vejar M, et al., (1990): Dissociation of platelet activation and spontaneous myocardial ischemia in unstable angina. Thromb Haemost 63(2):163-8 102. Conejero-Gonzalez R., Rivera J., Corral J., Acuna C., Guerrero J A and Vicente V (2004): Biological Assessment of Aspirin efficacy on healthy individuals. Heterogeneous response or aspirin failure? Stroke: 36:276. 103. Pamukcu B., Oflaz H., Nisanci Y (2005): The role of platelet glycoprotein IIIa polymorphism in the high prevalence of in vitro aspirin resistance in patients with intracoronary stent restenosis. American Heart Journal: 675-680 104. Carrol J., Gonzalez-Conejero, Iniesta J. A., Rivera J., Martinex C. and Vicente V (2000) The FXIII Val34Leu polymorphism in venous and arterial thromboembolism. Hematologica 85: 293-297
PHS 398/2590(Rev. 09/04) Page - 59 -