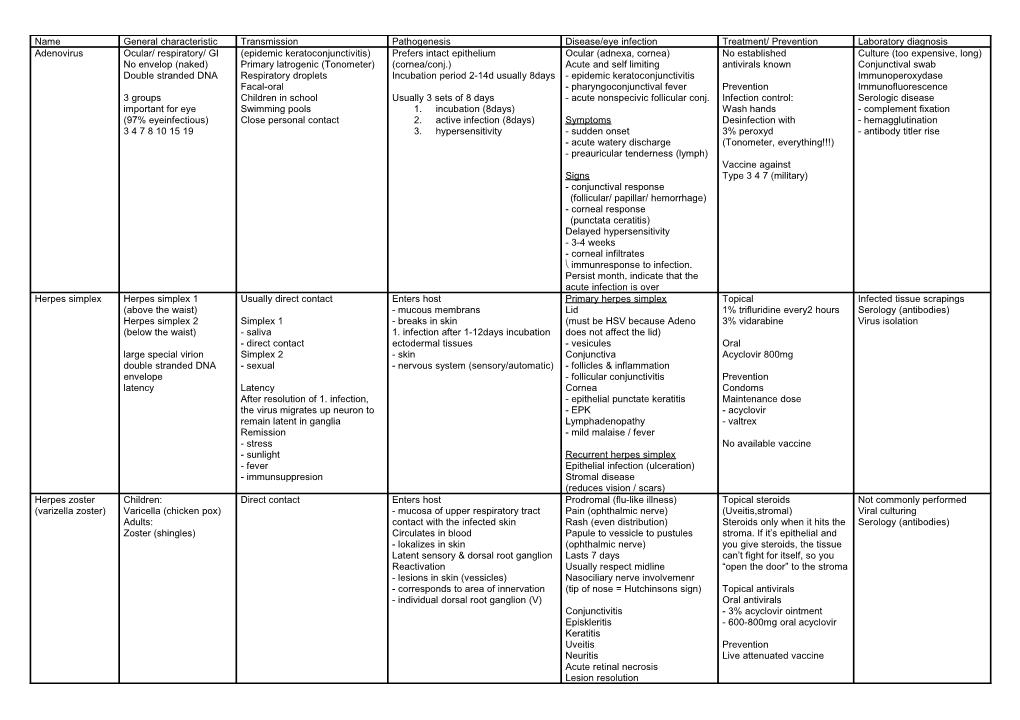
Name General characteristic Transmission Pathogenesis Disease/eye infection Treatment/ Prevention Laboratory diagnosis Adenovirus Ocular/ respiratory/ GI (epidemic keratoconjunctivitis) Prefers intact epithelium Ocular (adnexa, cornea) No established Culture (too expensive, long) No envelop (naked) Primary latrogenic (Tonometer) (cornea/conj.) Acute and self limiting antivirals known Conjunctival swab Double stranded DNA Respiratory droplets Incubation period 2-14d usually 8days - epidemic keratoconjunctivitis Immunoperoxydase Facal-oral - pharyngoconjunctival fever Prevention Immunofluorescence 3 groups Children in school Usually 3 sets of 8 days - acute nonspecivic follicular conj. Infection control: Serologic disease important for eye Swimming pools 1. incubation (8days) Wash hands - complement fixation (97% eyeinfectious) Close personal contact 2. active infection (8days) Symptoms Desinfection with - hemagglutination 3 4 7 8 10 15 19 3. hypersensitivity - sudden onset 3% peroxyd - antibody titler rise - acute watery discharge (Tonometer, everything!!!) - preauricular tenderness (lymph) Vaccine against Signs Type 3 4 7 (military) - conjunctival response (follicular/ papillar/ hemorrhage) - corneal response (punctata ceratitis) Delayed hypersensitivity - 3-4 weeks - corneal infiltrates immunresponse to infection. Persist month, indicate that the acute infection is over Herpes simplex Herpes simplex 1 Usually direct contact Enters host Primary herpes simplex Topical Infected tissue scrapings (above the waist) - mucous membrans Lid 1% trifluridine every2 hours Serology (antibodies) Herpes simplex 2 Simplex 1 - breaks in skin (must be HSV because Adeno 3% vidarabine Virus isolation (below the waist) - saliva 1. infection after 1-12days incubation does not affect the lid) - direct contact ectodermal tissues - vesicules Oral large special virion Simplex 2 - skin Conjunctiva Acyclovir 800mg double stranded DNA - sexual - nervous system (sensory/automatic) - follicles & inflammation envelope - follicular conjunctivitis Prevention latency Latency Cornea Condoms After resolution of 1. infection, - epithelial punctate keratitis Maintenance dose the virus migrates up neuron to - EPK - acyclovir remain latent in ganglia Lymphadenopathy - valtrex Remission - mild malaise / fever - stress No available vaccine - sunlight Recurrent herpes simplex - fever Epithelial infection (ulceration) - immunsuppresion Stromal disease (reduces vision / scars) Herpes zoster Children: Direct contact Enters host Prodromal (flu-like illness) Topical steroids Not commonly performed (varizella zoster) Varicella (chicken pox) - mucosa of upper respiratory tract Pain (ophthalmic nerve) (Uveitis,stromal) Viral culturing Adults: contact with the infected skin Rash (even distribution) Steroids only when it hits the Serology (antibodies) Zoster (shingles) Circulates in blood Papule to vessicle to pustules stroma. If it’s epithelial and - lokalizes in skin (ophthalmic nerve) you give steroids, the tissue Latent sensory & dorsal root ganglion Lasts 7 days can’t fight for itself, so you Reactivation Usually respect midline “open the door” to the stroma - lesions in skin (vessicles) Nasociliary nerve involvemenr - corresponds to area of innervation (tip of nose = Hutchinsons sign) Topical antivirals - individual dorsal root ganglion (V) Oral antivirals Conjunctivitis - 3% acyclovir ointment Episkleritis - 600-800mg oral acyclovir Keratitis Uveitis Prevention Neuritis Live attenuated vaccine Acute retinal necrosis Lesion resolution Name General characteristic Transmission Pathogenesis Disease/eye infection Treatment / Prevention Laboratory diagnosis Cytomegaliovirus Ubiquitous human virus Congenital infection Primary infection Immunosuppression (severe) Gancyclovir Virus recovery - across placenta - Pregnancy/ delivery - reactivation of virus Foscarnet - mouth swabs Common & often in apparent - AIDS - Urine Infected body fluids 90-100% of adults in developped - cancer (chemotherapy) No vaccine available - Liver countries show past exposure - transplant - Adenoids Port of entry: Usually aquired in first 5 years - kidney Contact infected saliva/urine Eye disease - Peripheral blood leukocytes Cytomegalovirus retinitis Serology (antibodies) AIDS patients Ketchup & Cheese fundus EpsteinBarr virus Nothing in sctipt Poxvirus Large (light microscope) Direct contact Smallpox Double stranded DNA - Eradicated by vaccine Envelope Molluscum virus - wart like, benign epithelial tumor - confined (skin, eye margin) (Molluscum contagiosum)
Human papilloma Double stranded DNA Eye diseases None virus No envelope Tropic Papoavirus family - epithelial cells Prevention (skin, mucous membranes) Immunization of woman wart like lesions - Eyelid margin - conjunctiva
Neurologic damage - deafness - retardation
Hepatitis Hepadnavirus Direct contact Liver Prevention Double stranded DNA Infected body fluid Recombinant vaccine Envelope recommended for health care A B C infection workers
Human Lentivirus family Infected body fluid Retina Reverse transcriptase ELISA immunodefficienc Very long latency Sexual contact Blood vessels (cotton wool spots) inhibition Western blot y virus RNA virus Most infectious Opportunistic infections Protease inhibition HIV Envelope - initial viremic stage Highli active antiretroviral AIDS = acquired immune - after latency therapy deficiency syndrome Infect T4 helper Future: Uncoating inhibitors lymphocytes severe immunosuppression Prevention No vaccine Consoms Gloves
Irène Imbach