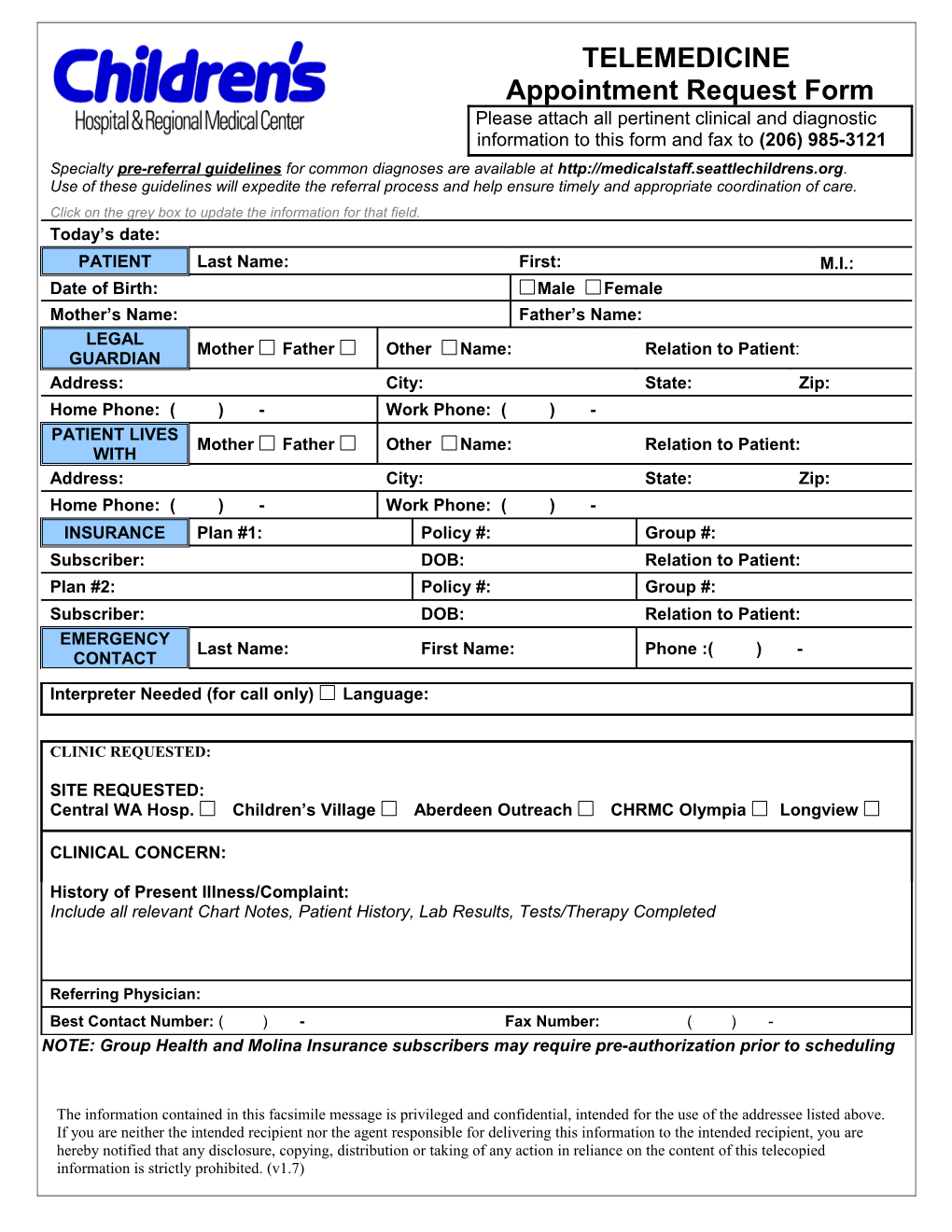
TELEMEDICINE Appointment Request Form Please attach all pertinent clinical and diagnostic information to this form and fax to (206) 985-3121 Specialty pre-referral guidelines for common diagnoses are available at http://medicalstaff.seattlechildrens.org. Use of these guidelines will expedite the referral process and help ensure timely and appropriate coordination of care. Click on the grey box to update the information for that field. Today’s date: PATIENT Last Name: First: M.I.: Date of Birth: Male Female Mother’s Name: Father’s Name: LEGAL Mother Father Other Name: Relation to Patient: GUARDIAN Address: City: State: Zip: Home Phone: ( ) - Work Phone: ( ) - PATIENT LIVES Mother Father Other Name: Relation to Patient: WITH Address: City: State: Zip: Home Phone: ( ) - Work Phone: ( ) - INSURANCE Plan #1: Policy #: Group #: Subscriber: DOB: Relation to Patient: Plan #2: Policy #: Group #: Subscriber: DOB: Relation to Patient: EMERGENCY Last Name: First Name: Phone :( ) - CONTACT
Interpreter Needed (for call only) Language:
CLINIC REQUESTED:
SITE REQUESTED: Central WA Hosp. Children’s Village Aberdeen Outreach CHRMC Olympia Longview
CLINICAL CONCERN:
History of Present Illness/Complaint: Include all relevant Chart Notes, Patient History, Lab Results, Tests/Therapy Completed
Referring Physician: Best Contact Number: ( ) - Fax Number: ( ) - NOTE: Group Health and Molina Insurance subscribers may require pre-authorization prior to scheduling
The information contained in this facsimile message is privileged and confidential, intended for the use of the addressee listed above. If you are neither the intended recipient nor the agent responsible for delivering this information to the intended recipient, you are hereby notified that any disclosure, copying, distribution or taking of any action in reliance on the content of this telecopied information is strictly prohibited. (v1.7)