Instructions for Completing the SF 424M Revised April, 2011
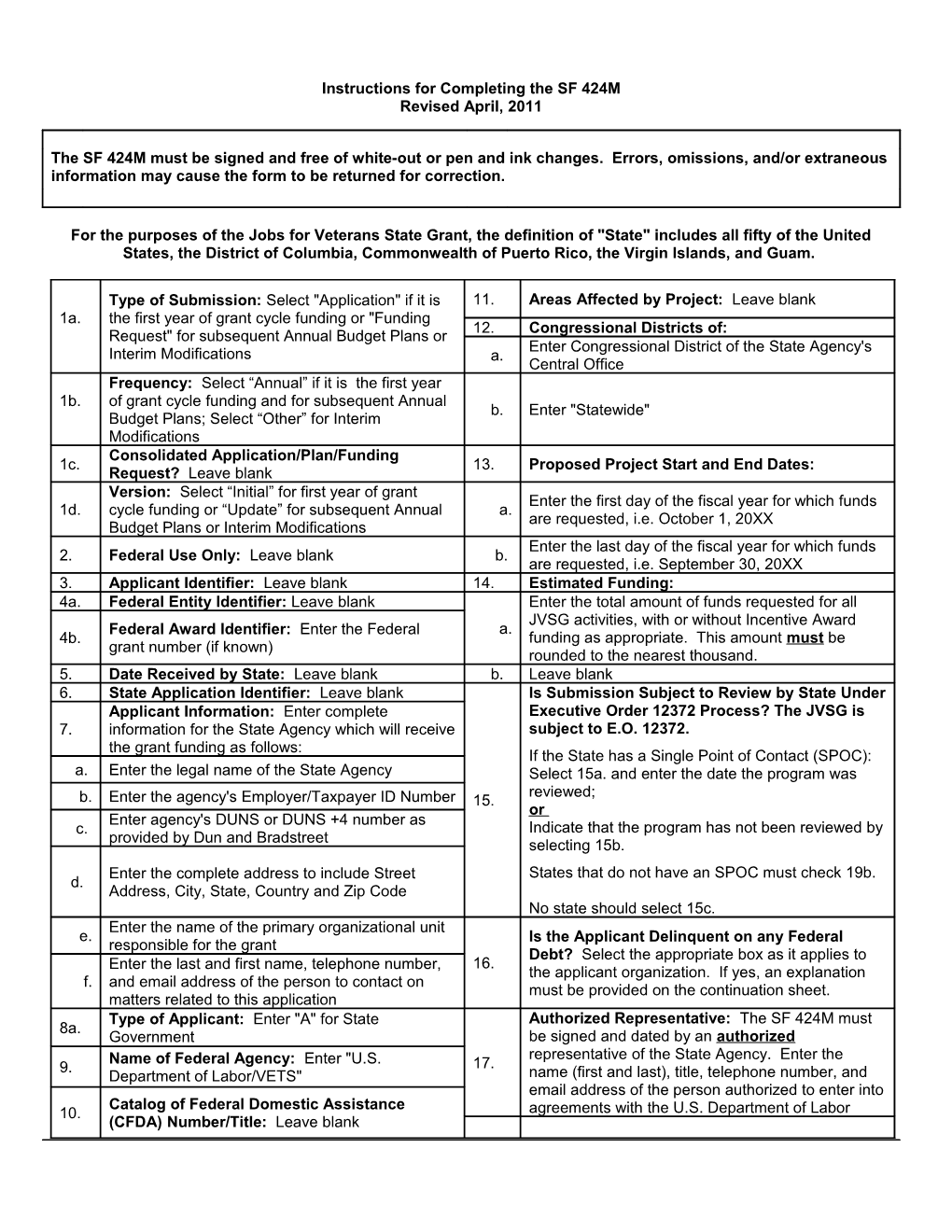
The SF 424M must be signed and free of white-out or pen and ink changes. Errors, omissions, and/or extraneous information may cause the form to be returned for correction.
For the purposes of the Jobs for Veterans State Grant, the definition of "State" includes all fifty of the United States, the District of Columbia, Commonwealth of Puerto Rico, the Virgin Islands, and Guam.
Type of Submission: Select "Application" if it is 11. Areas Affected by Project: Leave blank 1a. the first year of grant cycle funding or "Funding 12. Congressional Districts of: Request" for subsequent Annual Budget Plans or Enter Congressional District of the State Agency's Interim Modifications a. Central Office Frequency: Select “Annual” if it is the first year 1b. of grant cycle funding and for subsequent Annual b. Enter "Statewide" Budget Plans; Select “Other” for Interim Modifications Consolidated Application/Plan/Funding 1c. 13. Proposed Project Start and End Dates: Request? Leave blank Version: Select “Initial” for first year of grant Enter the first day of the fiscal year for which funds 1d. cycle funding or “Update” for subsequent Annual a. are requested, i.e. October 1, 20XX Budget Plans or Interim Modifications Enter the last day of the fiscal year for which funds 2. Federal Use Only: Leave blank b. are requested, i.e. September 30, 20XX 3. Applicant Identifier: Leave blank 14. Estimated Funding: 4a. Federal Entity Identifier: Leave blank Enter the total amount of funds requested for all JVSG activities, with or without Incentive Award Federal Award Identifier: Enter the Federal a. 4b. funding as appropriate. This amount must be grant number (if known) rounded to the nearest thousand. 5. Date Received by State: Leave blank b. Leave blank 6. State Application Identifier: Leave blank Is Submission Subject to Review by State Under Applicant Information: Enter complete Executive Order 12372 Process? The JVSG is 7. information for the State Agency which will receive subject to E.O. 12372. the grant funding as follows: If the State has a Single Point of Contact (SPOC): a. Enter the legal name of the State Agency Select 15a. and enter the date the program was reviewed; b. Enter the agency's Employer/Taxpayer ID Number 15. or Enter agency's DUNS or DUNS +4 number as c. Indicate that the program has not been reviewed by provided by Dun and Bradstreet selecting 15b. Enter the complete address to include Street States that do not have an SPOC must check 19b. d. Address, City, State, Country and Zip Code No state should select 15c. Enter the name of the primary organizational unit e. Is the Applicant Delinquent on any Federal responsible for the grant Debt? Select the appropriate box as it applies to Enter the last and first name, telephone number, 16. the applicant organization. If yes, an explanation f. and email address of the person to contact on must be provided on the continuation sheet. matters related to this application Type of Applicant: Enter "A" for State Authorized Representative: The SF 424M must 8a. Government be signed and dated by an authorized Name of Federal Agency: Enter "U.S. representative of the State Agency. Enter the 9. 17. Department of Labor/VETS" name (first and last), title, telephone number, and email address of the person authorized to enter into Catalog of Federal Domestic Assistance 10. agreements with the U.S. Department of Labor (CFDA) Number/Title: Leave blank