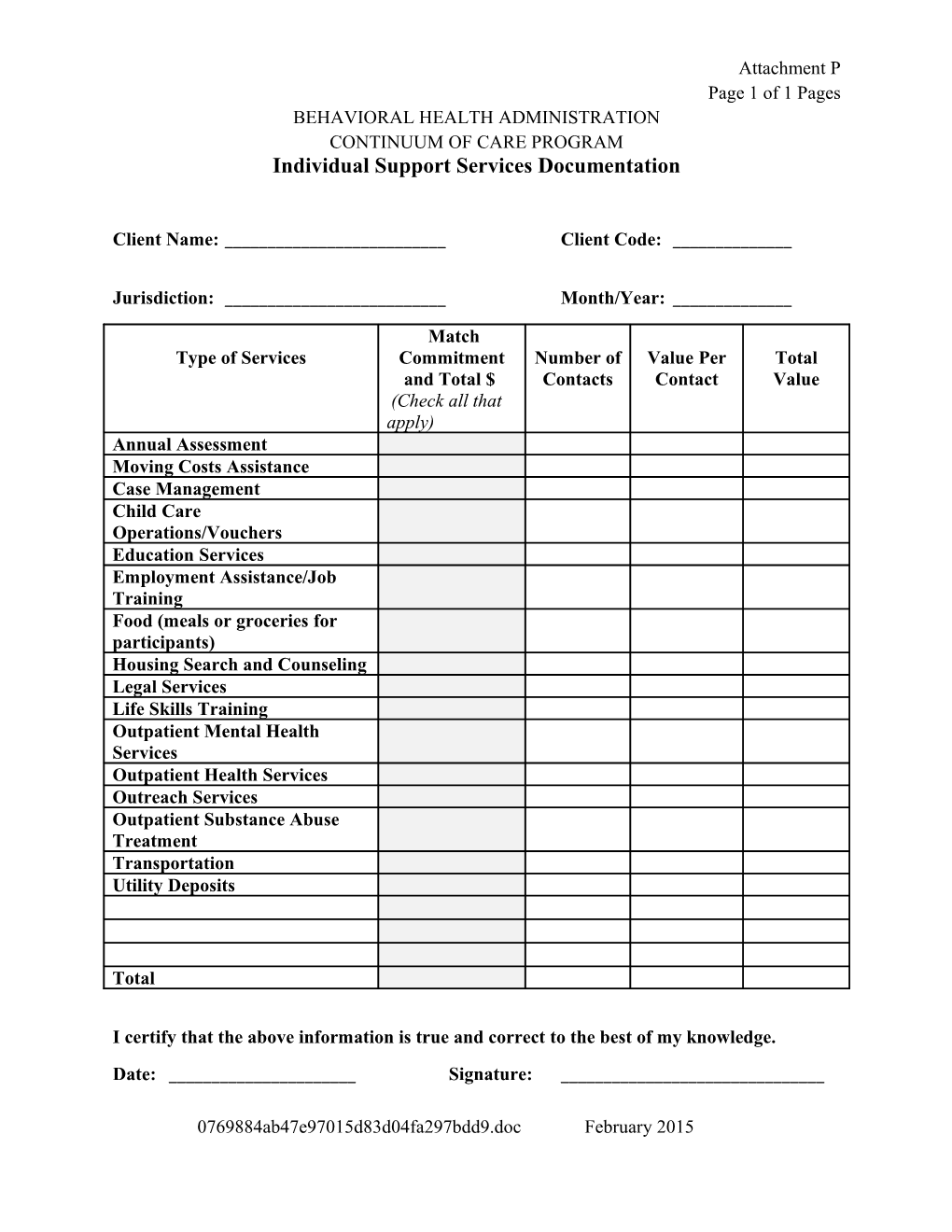
Attachment P Page 1 of 1 Pages BEHAVIORAL HEALTH ADMINISTRATION CONTINUUM OF CARE PROGRAM Individual Support Services Documentation
Client Name: ______Client Code: ______
Jurisdiction: ______Month/Year: ______
Match Type of Services Commitment Number of Value Per Total and Total $ Contacts Contact Value (Check all that apply) Annual Assessment Moving Costs Assistance Case Management Child Care Operations/Vouchers Education Services Employment Assistance/Job Training Food (meals or groceries for participants) Housing Search and Counseling Legal Services Life Skills Training Outpatient Mental Health Services Outpatient Health Services Outreach Services Outpatient Substance Abuse Treatment Transportation Utility Deposits
Total
I certify that the above information is true and correct to the best of my knowledge.
Date: ______Signature: ______
0769884ab47e97015d83d04fa297bdd9.doc February 2015