Getting to Zero
UNAIDS Joint Programme
STRATEGIC PLAN 2011-2015
First Draft—For Comment
10 September 2010 Contents
The Plan – At a glance...... 1 I The rationale for a new strategic plan...... 2 II A new Strategic Plan...... 6 III UNAIDS Strategic Directions 2011-2015...... 8 IV Core themes guiding UNAIDS action...... 19 V Delivering Results...... 22 Annex 1. UNAIDS’ ECOSOC Mandate...... 28 Annex 2. UNAIDS’ Guiding Principles...... 28 Annex 3. Core principles governing the Division of Labour...... 29
List of acronyms
ILO International Labour Organization MDGs Millennium Development Goals TB Tuberculosis UNAIDS United Nations Joint Programme on HIV/AIDS UNDP United Nations Development Programme UNESCO United Nations Educational, Scientific and Cultural Organisation UNFPA United Nations Population Fund UNGASS United Nations General Assembly Special Session UNHCR United Nations High Commissioner for Refugees UNICEF United Nations Children’s Fund UNODC United Nations Office on Drugs and Crime WFP World Food Programme WHO World Health Organisation
Definition of Terms [Technical terms used throughout the document will be defined here]
Higher risk and most at risk groups Vulnerable groups Key populations
DRAFT ii UNAIDS Vision
Zero new infections. Zero discrimination. Zero AIDS-related deaths.
UNAIDS Mission
The Joint United Nations Programme on HIV/AIDS (UNAIDS) is an innovative partnership of ten United Nations Cosponsors1 and the UNAIDS Secretariat. UNAIDS’ strength derives from the diverse expertise, experience and mandate of its Cosponsors and the added value of the Secretariat in leadership and advocacy, coordination and joint accountability. UNAIDS’ mission is to lead and inspire the world in achieving universal access to HIV prevention, treatment, care and support by:
. Uniting the efforts of the United Nations system, civil society, national governments, the private sector, global institutions and people living with and most affected by HIV; . Speaking out in solidarity with the people most affected by HIV in defence of human dignity, human rights and gender equality; . Mobilising political, technical, scientific and financial resources and holding ourselves and others accountable for results; . Empowering agents of change with strategic information and evidence to influence and ensure that resources are targeted where they deliver the greatest impact and bring about a prevention revolution; and . Supporting inclusive country leadership for sustainable responses that are integral to and integrated with national health and development efforts.
1 ILO, UNDP, UNESCO, UNFPA, UNHCR, UNICEF, UNODC, WFP, WHO, World Bank. This document will be updated to reflect new Cosponsors.
DRAFT iii The Plan – At a glance
Our goals Achieve Universal Access to HIV prevention, treatment, care and support Halt the spread of HIV (MDG 6) and contribute to the achievement of the MDGs
Our strategic Revolutionise HIV prevention directions 7400 people are newly infected with HIV everyday. UNAIDS aims to revolutionise HIV prevention efforts by supporting communities to demand effective prevention approaches and supporting countries to deliver the appropriate combination of biomedical, behavioural and structural approaches. UNAIDS will help countries to improve the utilization, quality and cost-effectiveness of HIV prevention programmes that are suited to the epidemiological context and meet the needs of key populations at higher risk and vulnerable to HIV exposure. Catalyse the next phase of treatment, care and support Ten million people living with HIV are in need of treatment today. UNAIDS aims support the development of more effective, ethical, affordable and sustainable approaches to treatment including its delivery and to scale up HIV counselling, testing and treatment access and coverage. UNAIDS will also support community mobilization to demand and deliver services, strengthen legal and social protection for people living with and affected by HIV and improve the reach, quality and affordability of care and support services. Put human rights and gender equality to work for HIV Despite unprecedented global commitment to the protection of human rights of those vulnerable to HIV and living with it, major legal and social barriers block an effective HIV response. UNAIDS will intensify its support to governments to realize and protect human rights in the HIV response, promote the enactment and enforcement of supportive laws and the removal of punitive laws, support communities to challenge harmful social and gender norms, address gender-based violence and promote the rights of women and girls for gender equality.
Our guiding Focus on country People at the HIV synergies with themes ownership and centre of the broader MDG and sustainability response human development efforts
1 I The rationale for a new strategic plan
1 The need to accelerate progress towards Universal Access
The past decade has seen a significant increase in global political and financial commitment to address HIV. In many places, the silence surrounding AIDS has been shattered, driven by people living with HIV and most affected by the epidemic and replaced with a clarion demand for universal access to HIV prevention, treatment, care and support. The international community has responded with unprecedented commitment – through the Millennium Development Goals (MDGs), 2001 UN General Assembly Declaration of Commitment on HIV/AIDS and 2006 UN General Assembly Political Declaration on HIV/AIDS. This commitment resulted in the massive mobilization of resources through the Global Fund to Fight AIDS, Tuberculosis and Malaria, World Bank Multi-country AIDS Programme, US President’s Emergency Fund for HIV/AIDS Relief (PEPFAR), other bilateral donors, private foundations, new global initiatives and affected countries – and transformed the HIV response.
The urgency of the epidemic demanded and resulted in exceptional global solidarity and new ways of working. The AIDS movement has brought the principle of “nothing for us without us” to global health, establishing novel norms and standards for inclusiveness and transparency in development approaches. The AIDS movement has pioneered results-based approaches, established ambitious global targets and forged a novel consensus about the need to address social, political and economic determinants of HIV risk and vulnerability.
The AIDS movement has resolutely demonstrated its ability to transform resources into concrete results for people. An estimated 5.2 million people in low- and middle-income countries now receive life-saving antiretroviral therapy, compared with 400,000 in 2003. Between 2004 and 2008, annual AIDS-related deaths decreased from an estimated 2.2 million to 2 million—as opposed to the 2.6 million deaths that would have occurred in 2008 without treatment. Globally, the number of new HIV infections declined by 17% between 2001 to 2008.2
2010 heralds the year set by the United Nations for achievement of Universal Access to HIV prevention, treatment, care and support. Yet, the task is not over. Four in five low- and middle-income countries are not on track to meet Universal Access targets.3 2.7 million people were infected with HIV in 2008 and an estimated 10 million people living with HIV are in need of treatment today.4 New infections continue to outpace capacity to provide treatment, with five people newly infected for every two who start
2 UNAIDS 2009 AIDS Epidemic Update. 3 United Nations General Assembly. Progress made in implementation of the Declaration of Commitment and Political Declaration, Report of the Secretary-General 1 April 2010. 4 UNAIDS Outlook Report 2010.
DRAFT 2 treatment. An estimated 33.4 million people were living with HIV, including 2.1 million children below the age of 15 years, in 2008.5
While commitments have made by national governments to protect human rights and provide a protective legal environment for people living with HIV and at higher risk of exposure, much less has been done to realize these commitments. Major barriers remain to effective responses in the form of stigma and discrimination, gender-based violence and punitive laws and practices.
Thus, major challenges remain in HIV prevention, treatment and human rights protection, reinforcing the need to reshape the response: giving higher priority and rethinking approaches to HIV prevention; identifying simpler and less costly treatment regimens; and tackling inequalities, punitive approaches and social norms that increase vulnerability to HIV infection and its impact. The universal access agenda is far from over and calls out for renewed impetus, new sources of funding and renewal of its leadership, particularly from the coming generation.
2 The need to respond to a evolving epidemic
Accelerating progress towards Universal Access also means responding to an evolving epidemic. Across the globe, modes in which people are getting infected with HIV are shifting. HIV transmission among men who have sex with men has increased throughout sub-Saharan Africa and accounts for a much larger proportion of epidemics than previously understood.6 Sexual transmission is growing in significance in many countries in Eastern Europe and Central Asia where the epidemic has been largely concentrated among people who inject drugs, often due to stigma and discrimination.7 And in some countries in South Asia, epidemics are emerging among couples in stable, long-term relationships while the linkage between HIV infection and unmet sexual and reproductive health needs is most tellingly reflected in high rates of infection among young women.8
These transitions have not been sufficiently matched with resource re-allocation and programmatic coverage of those at higher risk of HIV exposure and to the most cost- effective interventions, while routine interventions do not sufficiently take into consideration HIV specific needs of select population groups. The development of the Know your epidemic and response methodology has significantly improved knowledge on the nature of epidemics and responses and is increasingly applied in the context of national planning. However, stronger political commitment to evidence-informed responses and better, up-to-date strategic information on epidemics and the influence of social, political, economic and legal environments are crucial to ensure that resource
5 UNAIDS Outlook Report 2010. 6 UNAIDS 2009 AIDS Epidemic Update. 7 UNAIDS 2009 AIDS Epidemic Update. 8 UNAIDS 2009 AIDS Epidemic Update.
DRAFT 3 allocation and programming reflect the local context and epidemiological needs, as well as address the needs of key populations.
3 The need to respond to a changing environment
The remarkable gains of the AIDS response remain fragile and changes in the wider environment have implications for sustaining and strengthening the HIV response. While addressing HIV as a global emergency has been a powerful force in mobilising resources and expanding HIV programmes, the upward trend in resources is uncertain to continue given a global recession and shifts in donor priorities. The Global Fund to Fight AIDS, Tuberculosis and Malaria for example has shortfalls for existing grant commitments and for the coming years. Funding constraints could jeopardise what has been achieved and future efforts to expand HIV programmes.
There is an increasing need to demonstrate why investing in the AIDS response is critical to achieve wider health, development and human rights outcomes. There is growing international recognition that, in many countries, other MDGs cannot be achieved without tackling HIV. HIV-related illnesses are a leading cause of mortality in women of reproductive age and almost one in every five maternal deaths worldwide in 2008 was linked to HIV.9 In six hyper-endemic countries, AIDS is responsible for over 40% of child mortality.10
Investment in HIV carries benefits in terms of economic activity, universal education, family and social cohesion as well as leveraging broader health, legal and social system improvements. An important share of HIV funding goes to broader social protection, community development and poverty relief programmes that mitigate the impact of the epidemic on the most vulnerable people in the poorest countries. Evidence from several countries, including Haiti and Rwanda, demonstrates that HIV financing has helped to strengthen primary health care, laboratory capacity and human resources for health.
At the same time, as a recent report of the UN Secretary General noted11, an effective and sustainable HIV response also depends on wider health, development and human rights efforts. Strengthening systems, reducing gender inequality, improving access to education and addressing poverty are all critical to effectively tackling HIV. There is, therefore, a need for coordinated action on issues that limit progress towards all the MDGs and, where appropriate, for integrated delivery of HIV and other services.
Looking forward, the AIDS response will be affected by trends in the world’s global political-economy with the continued rise of the BRICS (Brazil, Russia, India, China and South Africa) and other emerging economies and the shift from a G8 to G20 world. The
9 REF 10 REF 11 United Nations General Assembly. Progress made in the implementation of the Declaration of Commitment on HIV/AIDS and the Political Declaration on HIV/AIDS, Report of the Secretary General 7 May 2009.
DRAFT 4 way UNAIDS manages the opportunities and challenges arising from this shift will significantly condition whether our goals are met. The burden of HIV in the BRICS alone constitutes one reason for special attention as does their potential as development partners. More strategically, the increasingly clout of the BRICS and other emerging economies in global negotiations on trade, development, human rights, intellectual property rights and other issues will have profound implications for many drivers of HIV and the response. The historic role of the BRICS in relation to TRIPS and essential medicines is a potential boon for the AIDS response while the failure of the G20 to adopt an explicit development agenda presents a major challenge.
4 The need to seize new opportunities
While aspects of the change we are seeing could undermine the AIDS response, recent developments also present major opportunities to be seized. Novel biomedical interventions and their application, including microbicides, pre/post-exposure prophylaxis, suppression of Herpes Simplex Virus-2 (HSV-2), vaccines, male circumcision and the prevention benefits of treatment have the potential to vastly reshape HIV prevention approaches. The wide availability of short-course treatments, combined with safer infant feeding, has made the virtual elimination of mother-to-child transmission of HIV achievable, as well as optimizing the health of the mother through expanded access to full treatment regimens. Integrating HIV, tuberculosis and sexual and reproductive health services is not only a more efficient use of available resources, but also maximizes prevention benefits. Innovations in telecommunications are increasingly being harnessed to scale up AIDS responses—mobile and web-based technology is utilized to disseminate health messages as part of successful behaviour change campaigns, train healthcare workers, support diagnosis and data collection and create spaces for information sharing and support. Further promise lies in the rise of a new, progressive and connected generation of leadership.
Indeed, this new leadership is key to the future social change required to achieve universal access and the MDGs. New data on the prevalence and impacts of stigma, discrimination and gender inequality in the context of HIV is positioning communities to drive social change agendas, for inclusion, dignity and equality. For example, people living with HIV have led the development and implementation of the People Living with HIV Stigma Index, which gives insight into how stigma and discrimination is experienced and underpins advocacy and programmatic action. There is near-universal reporting on the implementation of the Declaration of Commitment on HIV/AIDS and country progress towards universal access. This has generated important national dialogues between a range of stakeholders on how law and policy is either helping or hindering the national response to the epidemic. In 2010, the Global Commission on HIV and the Law was launched to review evidence and galvanise commitment and action in order to make law work for an effective and human rights-based response to HIV. Following the work of the International Task Team on HIV-related Travel Restrictions, several countries have either removed or are taking steps to remove restrictions on entry, stay
DRAFT 5 or residence due to HIV status, showing that we can remove punitive and discriminatory laws and practices that undermine effective responses to the epidemic, and in doing so, restore dignity to people living with and affected by HIV.
II A new Strategic Plan
This Strategic Plan sets out how UNAIDS Cosponsors and Secretariat aim to collectively respond to barriers limiting progress towards universal access, to an evolving epidemic and to the challenges and opportunities presented by a shifting global environment. With this plan, we aim to:
. Set out a clear agenda for strengthening the HIV response and accelerating progress towards universal access with cost-effective programmes. . Maintain commitment to HIV in the face of competing global priorities. . Highlight the links between achieving Universal Access and the MDGs, particularly those related to gender equality, education and health and bring the target date for universal access in line with the MDGs. . Move towards an efficient, sustainable and evidence-informed long term HIV response that is integrated within the wider health and development agenda. . Establish a framework for measuring and monitoring progress and mutual accountability of the work of the Joint Programme.
The plan aligns with and builds on the HIV strategies of the Cosponsors—some of which are sector-specific (such as the health sector orientation of the WHO-HIV strategy) and some of which are population-specific (such as UNHCR’s strategy to protect refugees, internally displaced persons and other persons of concern in the context of HIV) as well as the priorities and goals identified in the UNAIDS Outcome Framework 2009-2011. The plan is synthetic in that it integrates these strategies as well as a number of instruments and tools which define how the Joint Programme operates and will be made operational through the Unified Budget and Workplan and, from 2012 onwards, a new Unified Budget and Accountability Framework. The plan responds to UNAIDS’ Second Independent evaluation12, which emphasized its successful leadership and broad-based political and social mobilization of commitment at global and country level while recommending that UNAIDS be more focused, strategic, flexible and responsive, efficient and accountable.
The following sections outline the plan’s strategic directions, core themes and conclude with an overview of the plan’s implementation tools.
The hierarchy of goals and activities are defined by three interlinking strategic directions. Bold goals for 2015 are included for each strategic direction, which have
12 UNAIDS Second Independent Evaluation 2002-2008 Final Report. 25th Meeting of the UNAIDS Programme Coordinating Board, Geneva, Switzerland, 8-10 December 2009.
DRAFT 6 been articulated in the implementation process of UNAIDS Outcome Framework. UNAIDS Outcome Framework, which guides UNAIDS investments over 2009-2011, identifies critical gaps in the AIDS response as well as the social, political and structural constraints that limit results where synergies and integration of the Joint Programme’s collective action can make a difference. The Outcome Framework has brought greater specificity to the value-added of UNAIDS, optimized joint working and Cosponsors’ and Secretariat’s comparative advantages, further orienting UNAIDS towards more focused, selective, results-based approaches, and enhanced mutual accountability. Consequently, this strategic plan builds on the gains already made, extending the Outcome Framework to 2015 and rooting each of the Framework’s ten priority areas within this plan’s strategic directions. As with the priority areas, the strategic directions are interlinked—where progress in one area contributes to and depends on progress in others. The strategic directions provide a comprehensive list of priority actions, from which country level Joint United Nations Teams on HIV will identify and select the most suitable based on the needs of the epidemic and the capacity of the Joint Programme. UNGASS and MDG impact indicators have been included for each strategic direction to align with international monitoring of progress towards universal access and MDG 6.
DRAFT 7 III UNAIDS Strategic Directions 2011-2015
Catalyse the next Revolutionise phase of HIV prevention treatment, care and support
Put human rights and gender equality to work for HIV
UNAIDS added-value, vis-à-vis other actors in the development landscape, in achieving the vision of zero new infections, zero discrimination, zero AIDS-related death is articulated in its Mission Statement. Its core and unique strengths are leveraged in this strategic plan. In particular: As a UN body, UNAIDS promulgates norms and standards, convenes governments, people living with HIV, civil society organizations and the private sector and mobilize resources for the global response As a joint programme, UNAIDS promotes integration and synergy in support of multi-sectoral and coordinated responses As a global programme with a presence in nearly every low- and middle-income country, UNAIDS generates and promotes the use of strategic information and evidence-informed policy to guide investments in targeted and quality responses and brokers mutual accountability to ensure their implementation With a human rights mandate, UNAIDS advocates for the human dignity, equality, rights, security, empowerment of all people and give voice to and promotes the leadership and the inclusion of those living with and affected by HIV in all aspects of the response As a joint programme, UNAIDS models UN reform and delivering as one as exemplified by the implementation of the Outcome Framework by Joint Country Teams
Strategic Direction 1: Revolutionise HIV prevention
DRAFT 8 A Prevention Revolution Context and challenges To halt the HIV epidemic will require nothing short of a prevention revolution. UNAIDS has committed itself to While the past two decades have supporting a revolution mobilized by communities to seen episodes of remarkable 1/ demand transformative social and legal change to success in HIV prevention redress gender, power and economic inequalities that particularly in countries that have inhibit safe practices and 2/ to remove barriers to implemented a combination of access, uptake and sustained use of quality prevention proven prevention programmes, services In galvanising this revolution, UNAIDS is evidence-informed approaches working to ensure that countries have better information about the determinants, dynamics and have not been applied more impact of their epidemic, and to support countries in widely, and national prevention applying this information for a cost-effective response efforts are often inadequate and that reaches those most-at -risk and most vulnerable. poorly targeted. Episodic success UNAIDS is promoting the intensification and scale up is not enough for a sustainable of proven combination prevention approaches, response. bolstered by integration with innovative and promising new approaches. Three key ideas underpin the Effective programmes to reduce strategy of the prevention revolution: mother-to-child transmission of 1. Demand and support political leaders to HIV are well-known but global acknowledge the ways in which people are getting coverage of such programmes was infected by creating political incentives to direct resources to those at highest risk of HIV infection; and only 45% in 2008, resulting in over to address the controversial social issues that drive 400,000 babies becoming infected vulnerability, such as gender inequality, gender-based with HIV that year. Prevention violence and punitive laws. programme coverage for key 2. Focus on the game changers that will reshape the populations including most at risk epidemic, like ending mother-to-child-transmission. populations such as injecting drug 3. Create a movement that energizes the revolution users, men who have sex with from the bottom up and the top down and focusing men, transgender people, sex social and political movements around specific workers and prisoners as well as interventions—like we have seen in South Africa, vulnerable populations including where leadership is linking scientific evidence with persons affected by humanitarian social change. emergencies (e.g. refugees and internally displaced persons) and migrants remains unacceptably low. According to the Commission on AIDS in Asia, 95% of HIV infections in young people in the region occur in those at higher risk but more than 90% of resources are spent on low risk youth. Effective prevention depends on understanding and involving key populations in programme design and delivery, and on addressing the politics, laws and social norms that increase vulnerability and reduce access to services.
Heterosexual transmission of HIV accounts for two-thirds of infections worldwide and 90% of infections in sub-Saharan Africa. Prevention programmes that target multiple and concurrent, and intergenerational, sexual relationships and the prevention needs of couples who are married or in stable relationships remain inadequate and ineffective.
DRAFT 9 The social change which underpins changed patterns of risk behaviour requires sustained multi-sectoral action, from community, the private sector and government acting in concert and across health, justice, education, gender, employment and welfare sectors. Services delivered in health care settings are an important part of meeting prevention needs, but are unlikely alone to generate the demand required to overcome the structural barriers that block effective responses to HIV.
The HIV prevention needs of people living with HIV have also been neglected. Effective approaches that involve people living with HIV in spearheading positive health, dignity and prevention initiatives are required.
UNAIDS Outcome Framework13 Prevention Goals Goals/Targets for 2015 Outcome area 50% reduction in sexual transmission Reduce sexual transmission of HIV Virtual elimination of PMTCT i.e. less than 5% Prevent mothers dying and babies infected with transmission of HIV from mother to child HIV Prevent as many as 850,000 new cases of HIV Protect drug users from becoming infected with among people who use drugs in 20 countries14 HIV Reduce new infections among 15-24 year olds by Empower young people to protect themselves 30% from HIV
UNAIDS Prevention Agenda
National commitment to effective combination prevention responses
UNAIDS will:
. Advocate for increased national political and financial commitment to HIV prevention and for setting HIV prevention targets. . Provide policy guidance and technical support to assist countries to develop national prevention strategies that reflect the epidemic context, ensure coverage for those most vulnerable and at risk of infection with evidence-informed programmes and to implement a combination of proven, cost-effective biomedical, behavioural and structural interventions at sufficient scale, and monitor coverage and impact15.
13 See: Joint action for results: UNAIDS outcome framework 2009-2011 14 Afghanistan, Bangladesh, Belarus, China, India, Indonesia, Kazakhstan, Kenya, Kyrgyzstan, Lithuania, Mauritius, Myanmar, Nepal, Nigeria, Pakistan, Republic of Moldova, South Africa, Ukraine, United Republic of Tanzania and Viet Nam 15 Combination prevention has the following features: it is tailored to national and local needs and contexts, includes a combination of biomedical, behavioural and structural elements—to reduce both the immediate risks and the underlying vulnerabilities; is developed with the full engagement of affected communities, promoting human rights and gender equality; operates synergistically, consistently over time, on multiple levels—individual, family and society; invests in decentralized and community responses and enhances coordination and management; and is
DRAFT 10 . Work with people living with HIV, government, the private sector and civil society partners to empower communities to boost visible social transformation to shift social norms, change behaviours, reduce HIV risks, create and voice demand for effective prevention programmes and to plan for and deliver services.
Global commitment and consensus around HIV prevention
UNAIDS will:
. Utilize traditional and novel forums and communication tools to deliver prevention messages, including to advocate for increased global political and financial commitment to HIV prevention. . Coordinate with international partners and initiatives to ensure harmonised global policies, guidelines and support for HIV prevention. . Monitor HIV prevention progress and hold global and national partners to account for results.
Generation of strategic information
UNAIDS will:
. Support countries to strengthen surveillance, monitoring and evaluation systems of HIV prevention programmes and in sharing knowledge and lessons learned. . Facilitate the generation of evidence through Know Your Epidemic and Response (KYE/R) methodologies with emphasis on improving understanding of the social and cultural drivers of epidemics and demonstrating the links between effective HIV prevention, gender and human rights and the law.
Innovation in HIV prevention science, tools and delivery
UNAIDS will:
. Support countries and partners to develop and introduce new prevention methods, tools and technologies. . Develop and evaluate approaches which maximise the prevention benefits of HIV treatment. . Enhance effectiveness and efficiency of HIV prevention programmes and programmes and strengthen the evidence base for new and promising prevention approaches, including for under-served and most-at-risk populations.
flexible and based on continuous learning—it can adapt to changing epidemic patterns and can rapidly adjust and deploy new tools and innovations.
DRAFT 11 Core MDG and UNGASS Indicators . Percentage of young women and men aged 15–24 who are HIV-infected . Percentage of infants born to HIV-infected mothers who are infected
Strategic Direction 2: Catalyze the next phase of treatment, care and support
Context and challenges
While HIV treatment access has expanded significantly, there is still a significant treatment gap. An estimated 10 million people living with HIV eligible for treatment do not have access to antiretroviral drugs. Paediatric treatment coverage remains unacceptably low in many countries. In sub-Saharan Africa, children living with HIV are about one third as likely to receive treatment as adults. Until the treatment gap is met, many people living with and affected by HIV will continue to need care and support to mitigate the impact of the epidemic. HIV has driven a resurgence of tuberculosis (TB) and contributed to the spread of drug resistant TB. TB is a major cause of death among people living with HIV. In 2007, cases of HIV/TB co-infection accounted for more than 25% of all TB deaths and 23% of all deaths among people living with HIV.16
HIV testing is a critical step towards accessing treatment but, despite the shift to provider-initiated testing and counselling and expansion of testing services, fewer than 40% of people living with HIV are aware of their status.17 Reported rates of testing among populations at the highest risk of HIV exposure are even lower. In 2008, only 38% of sex workers in 45 countries, 30% of men who have sex with men in 31 countries, and 23% of people who inject drugs in 26 countries received HIV testing and counselling.18
The costs of HIV treatment are set to increase, as countries scale up treatment, adopt recommendations on earlier initiation of ART, provide safer but more expensive regimens and respond to the growing need for second- and third-line treatment. As countries scale up access to ART, prevention and control of HIV drug resistance is also a key challenge. While available evidence suggests that resistance remains low, greater efforts are needed to minimise the emergence of drug resistance and to support countries to put systems in place to monitor and manage drug resistance. Further, while drug prices have been reduced, the non-drug costs of delivering ART remain high, accounting for up to 80% of the overall costs of treatment.
There is an urgent need to develop simpler, more effective and more affordable drug regimens, in order to scale up access, enable treatment to start earlier in the course of
16 REF 17 REF 18 REF
DRAFT 12 the disease, improve adherence and prevent the development of drug resistance, and to ensure the sustainability of HIV treatment. Reducing costs also requires the development of simpler and more affordable point-of-care diagnostic tools, in particular to monitor CD4 cell counts and viral load, as well as action to address policy barriers and improve the efficiency of health systems.
Particular attention needs to be given to addressing shortages of critical human resources for health, strengthening procurement and supply management and establishing the basic infrastructure needed to support service delivery, and in strengthening and expanding HIV treatment in resource poor settings including countries affected by humanitarian emergencies. The current approach largely depends on specialist doctors, limiting access to treatment in countries with shortages of trained medical staff and for people who live far from specialised facilities. New delivery approaches, including integration of HIV treatment within wider health services and community-based delivery of ART to bring treatment closer to where people live, are critical to scale up access. Countries such as Lesotho and Malawi have significantly increased treatment access through nurse-managed and community-driven provision of ART services at primary care level. Radical simplification of treatment and lab procedures are critical to move HIV treatment out of isolation, with implications for stronger systems as every dollar invested into primary care level treatment benefits a broader health system.
Integration or linkages between HIV and other health, community and social services are critical to meeting the range of people’s health needs and to improving coverage, quality and cost-effectiveness. The extent of integration or linkages depends on factors such as the epidemiology of HIV, the organisation of health and social systems, and the resources available. Improved availability of HIV services must be matched by action to generate greater community demand for HIV testing.
Improving the quality of services, including ensuring that service delivery is based on respect for the human rights of all people living with HIV, is also critical to the effectiveness and sustainability of treatment. Poor quality services have an adverse impact on treatment uptake and adherence, and low treatment adherence has implications for the emergence of HIV drug resistance and for the costs of providing second-line and third-line regimens. Greater attention also needs to be paid to nutrition, which plays an essential role in maintaining the health of people living with HIV and in treatment adherence, and nutrition counselling and support needs to be better integrated with delivery of HIV treatment.
Ensuring that all who need it receive treatment remains a priority, to save lives and improve quality of life. But investing in treatment also has wider benefits. There is growing evidence that ART can reduce the risk of HIV transmission as well as rates of TB disease. Increasing treatment coverage therefore has the potential to make a significant contribution to HIV prevention and TB control.
DRAFT 13 UNAIDS Outcome Framework Treatment, Care and Support Goals
Goals/Targets for 2015 Outcome Area Ensure all people living with HIV in need receive Ensure people living with HIV receive treatment treatment 50% reduction in TB deaths among people living with Prevent people living with HIV dying from TB HIV19 Ensure that national social protection strategies are Enhance social protection for people affected inclusive of people and households affected by HIV by HIV
UNAIDS Treatment, Care and Support Agenda
Global commitment to treatment access
UNAIDS will:
. Promote the Treatment 2.0 agenda20. . Advance the case for sustained investment in HIV treatment, care and support, including the contribution of treatment to HIV prevention, with donors and national governments. . Support global, national civil society organisations and people living with HIV to advocate for universal access to treatment for all who need it. . Mobilize the private sector, particularly the pharmaceutical and diagnostics industries, to increase access to treatment. . Support countries to expand access to HIV counselling, testing and treatment in accordance with evidence-informed national strategies . Promote concerted action on international trade and patent laws including the removal of tariffs and taxes and support for countries on use of provisions under the trade-related aspects of intellectual property rights (TRIPS) agreement. . Provide strategic information to countries to support procurement, including through the WHO AIDS Medicines and Diagnostics Service.
Better drug regimens, diagnostics and delivery
19 Compared with 2004 baseline 20 Text on Treatment 2.0
DRAFT 14 UNAIDS will:
. Advocate for investment in research and development of simpler, more affordable fixed dose combination drug regimens with fewer side effects and less long-term toxicity, and simpler, more affordable point-of-care tools for monitoring CD4 cell count and viral load. . Advocate for reduced pricing of drugs for second-line treatment and diagnostic tools. . Strengthen the evidence base for innovative, rights-based approaches to delivery of HIV testing and treatment to support of treatment adherence and monitoring treatment outcomes.
Strengthened national and community systems to deliver HIV treatment, care and support
UNAIDS will:
. Provide technical support for integrating delivery of HIV treatment and care with TB, maternal, neonatal and child health, sexual and reproductive health, nutritional support and hepatitis care, as appropriate to the country and epidemic context. . Provide technical support to strengthen human resources for health, commodity procurement and supply management, laboratory capacity, and monitoring and management of drug resistance. . Provide technical support to strengthen social protection systems for people living with and affected by HIV. . Support government and NGOs to ensure continuity of treatment during and following humanitarian emergencies . Partner with government, private sector and civil society partners to strengthen community systems and mobilise communities and marginalised population groups to increase demand for decentralised, community- and rights-based delivery of HIV testing and treatment.
MDG and UNGASS Indicators . Percentage of adults and children with HIV still alive and known to be on treatment 12 months after initiation of antiretroviral therapy . Percentage of women and men with advanced HIV infection receiving antiretroviral therapy
DRAFT 15 Strategic Direction 3: Put human rights and gender equality to work for HIV
Context and challenges
The AIDS movement, particularly its vibrant civil society sustained by people living with HIV, continues to record victories, from the reading down of repressive laws on sodomy to the end of HIV-related restrictions on entry, stay and residence in global powers. Nevertheless, punitive laws remain widespread—and, in many countries, on the rise. These laws criminalize men who have sex with men, sex workers and their clients, and people who use drugs. They also criminalize HIV transmission in an overly-broad fashion in direct contradiction to the commitment in the Political Declaration on HIV/AIDS to create a legal environment safe for voluntary disclosures. Stigma and discrimination remain extremely widespread undermining public health approaches, human rights and dignity. In this context, there is an urgent need to refocus UN support for evidence- informed prevention and treatment programmes, laws and law enforcement that will secure access to services and programmes to empower those vulnerable to HIV and living with it.
A number of countries have repealed punitive laws and restrictions on the mobility and migration of people living with HIV. Supportive legal and policy environments are having a positive impact – ensuring non-discrimination in schools and the workplace, protecting the inheritance and property rights of women and children, and guaranteeing access to treatment.
Despite progress, human rights violations, discriminatory laws and policies and persistent stigma continue to undermine efforts to prevent new HIV infections and reach most-at-risk populations including injecting drug users, men who have sex with men, transgender people, sex workers and prisoners as well as vulnerable populations including persons affected by humanitarian emergencies and migrants in HIV-related programming and service delivery. These populations are understandably reluctant to seek services in contexts where their behaviour considered unlawful. Furthermore, laws that criminalise HIV transmission also discourage people from seeking HIV testing or revealing their HIV status.
Even as there is evidence of elevated HIV prevalence among men who have sex with men in all regions, a number of countries have legislation that criminalises same-sex sexual conduct. Many countries prohibit or limit access to harm reduction services for people who use drugs. In 2008, nearly two-thirds of countries reported having policies or laws that impede access to HIV services by vulnerable populations.21 In the same year, one in three countries did not have laws prohibiting discrimination against people
21 REF
DRAFT 16 living with HIV22, and most countries did not have legislation to protect men who have sex with men, sex workers and people who use drugs from discrimination. More than 30 countries have enacted HIV-specific laws that criminalise HIV transmission or exposure, and over two dozen countries have used non-HIV-specific laws to prosecute individuals on similar grounds.
Punitive and coercive laws and policies are both counterproductive from a public health perspective and antithetical to the human rights basis of effective prevention. Leaders must demonstrate political courage in removing punitive laws and enacting protective laws, addressing social norms that increase HIV vulnerability, and challenging stigma and discrimination within their societies.
Beyond a harmful legal environment, harmful social and cultural norms and practices create detrimental power imbalances, undermining individuals and entire populations’ ability to protect themselves from HIV. Efforts to promote gender equality, reduce gender-based violence and realise the human rights of women and girls are central to the HIV response, as well as to the achievement of the MDGs. In sub-Saharan Africa, the region that continues to bear the brunt of the epidemic, women are disproportionately infected and affected by HIV. Social norms that prevent equality in decision-making related to sexuality and reproduction and promote stigma, secrecy, shame, discrimination and violence are at the core of the HIV epidemic. Social norms governing behaviours and attitudes related to issues including multiple concurrent relationships, insufficient and inconsistent condom use, low levels of circumcision, intergenerational sex, gender and sexual violence, stigmatization of men who have sex with men and other sexual minorities, drug use and harmful traditional practices must be addressed and positively transformed. Discriminatory policies and practices including inequity in sufficient and meaningful access to services by persons affected by humanitarian emergencies and migrants need to be addressed.
There is an urgent need for practical action on gender that protects and enforces individual’s rights, engages communities, and links efforts to reduce vulnerability, particularly of women, to HIV to wider health and development issues including maternal health, education and employment opportunities, property rights and sexual violence.
Data on the impact of discrimination, punitive laws, gender-based violence indicate that there must be a major shift not only in the populations more intensively covered by the response but also in the nature of the content of the programmes. Increasingly called for are programmes that reduce stigma, discrimination, gender inequality, gender-based violence and harmful gender norms, as well as programmes that empower vulnerable people with legal literacy and support, economic opportunities and social protection. It has become clear that working with police, judges, Parliamentarians, Ministries of Justice, Interior and Migration, traditional community and faith-based leaders is as
22 REF
DRAFT 17 important as working with health care workers, health care facilities and the Ministry of Health.
UNAIDS Outcome Framework Human Rights and Gender Equality Goals
Goals/Targets for 2015 Outcome area Legal, regulatory and social environments advance Remove punitive laws, policies, practices, stigma and safeguard dignity, health and justice in the and discrimination that block effective responses to context of HIV in all settings AIDS Men who have sex with men, transgender people Empower men who have sex with men, sex workers and sex workers empowered to avoid HIV infection and transgender people to prevent HIV and to fully and claim their rights access ART National AIDS responses address the specific needs Meet the HIV needs of women and girls and stop and rights of women and girls and reduce sexual sexual and gender-based violence and other forms of gender-based violence
UNAIDS Human Rights and Gender Equality Agenda
Removal of punitive laws, policies and practices that block the AIDS response and elimination of HIV-related discrimination
UNAIDS will:
. Support countries to enact or reform laws and policies to protect the rights of people vulnerable to HIV infection and people living with and affected by HIV and to eliminate HIV-related stigma discrimination in all sectors of society, including workplaces, health care and educational settings. . Engage Ministries of Interior, Justice, Migration, and Gender as well as parliamentarians, the judiciary and the police. . Support national partners to monitor enforcement of laws and access to justice, as well as implement and expand programmes to provide human rights and legal literacy, to provide legal assistance and redress, to train health care workers and police in non-discrimination, to reform law and to reduce violence against women and harmful gender norms and traditional practices. . Monitor progress on enabling legal environments, respond to human rights violations and hold governments to account for commitments on human rights and gender equality.
Socially-inclusive, rights-based HIV responses
UNAIDS will:
DRAFT 18 . Promote socially inclusive, rights-based responses that promote the empowerment and resilience of women and girls, men who have sex with men, transgender people and other sexual and gender minorities, sex workers and people who inject drugs and other vulnerable groups such as migrants and persons affected by humanitarian emergencies. . Advocate for the active involvement of these populations in the design, implementation, and monitoring and evaluation of HIV programmes. . Build leadership and advocacy capacity of organisations of these populations.
Supportive, non-stigmatizing social and gender norms
UNAIDS will:
. Support national partners to implement programmes and mobilise communities to change harmful social and gender norms and practices. . Highlight the impact of harmful social and gender norms on the epidemic and promote dialogue with stakeholders who influence norms including political, religious and community leaders and the media. . Promote effective, evidence-informed programmes to encourage positive social and gender attitudes towards vulnerable and most at risk groups . Support national partners to implement, expand and monitor programmes to reduce stigma and document and disseminate evidence on effective approaches to stigma reduction.
Reduction of gender-based violence
UNAIDS will:
. Advocate for enactment and enforcement of laws to provide women, men who have sex with men and transgender people with equal rights and to prohibit gender-based violence and discrimination. . Document and disseminate evidence on effective approaches to reduce gender- based violence and discrimination, including those that promote active involvement of men and boys.
MDGs and UNGASS Indicators . Percentage of most-at-risk populations23 who are HIV-infected
UNAIDS Indicators . Number of countries with HIV travel restrictions . Number of countries that criminalize HIV transmission
23 Define
DRAFT 19 IV Core themes guiding UNAIDS action
Achievement of UNAIDS Vision and the Goals of the Strategic Plan requires stronger engagement with countries, communities and people living with and affected by the epidemic and integration of HIV within wider health and development agendas. UNAIDS action across the Strategic Directions will therefore be under-pinned by the following core themes.
Increased focus on country ownership and sustainability of the HIV response
UNAIDS’ guiding principles include a focus on the country-level results and outcomes through support for nationally-defined priorities, processes and accountability mechanisms and a commitment to national ownership, alignment, harmonisation and capacity development. While UNAIDS will continue to use its comparative advantage at global level, the Joint Programme will focus efforts in 2011-2015 on making a stronger impact where it most counts—at the country level. UNAIDS will:
. Promote effective country leadership and ownership of the HIV response, including the “Three Ones”. . Support governments to coordinate strategic national responses, informed by the Know Your Epidemic and Your Response approach, using mechanisms best suited to their context and promote harmonisation and alignment of actions by all stakehold- ers with national plans. . Strengthen government accountability and transparency for delivering universal ac- cess, including support for the development of broad-based accountability mechan- isms. . Shift emphasis from programme and project approaches to support for policy devel- opment and multi-sector strategic and operational planning. . Tailor support to country priorities and plans rather than to organisational mandates and historical relationships, recognising that different epidemics and country con- texts require different strategies. . Strengthen country monitoring and evaluation (M&E) capacity to track the effi- ciency, effectiveness and transparency of HIV responses, to conduct context-relev- ant operations research, including return on investment analyses, and to better un- derstand their epidemic and develop evidence-informed programming and resource allocation. . Leverage partnerships with international actors, particularly the Global Fund, to en- hance support for building national capacity, including strengthening of key institu- tions such as health professional schools, reference laboratories and centres of ex- cellence for HIV prevention, care and treatment to assure a sustainable response to HIV.
DRAFT 20 . Support countries to mobilise sustainable and predictable financing required to meet commitments, including support for country-led Global Fund proposal devel- opment, implementation and oversight processes. . Support the mobilisation of external funding through national planning, budgeting, disbursement and monitoring mechanisms, including working with external donors.
People at the centre of the response
Partnership, empowerment and inclusion are guiding principles for UNAIDS. Major successes in the global HIV response have come about due to the dynamism of people living with and affected by HIV and the alliances they have built with health, development and rights stakeholders around issues of common concern. Leadership by those most affected has substantially strengthened the development of HIV policies and strategies, generated political and financial commitment, galvanised the expansion in treatment access and transformed the way that services for those most at risk of HIV have been delivered. But more must and can be done to ensure that the voices of people living with HIV and key affected populations are at the centre of the HIV response and to maximize the potential of people and communities to strengthen collective efforts. During 2011-2015, the Joint Programme will promote ‘people-centred approaches’ that build on successes to date. UNAIDS will:
. Advocate for and overcome the barriers to the active engagement of civil society organisation, private sector, people living with HIV and key affected populations in the response. . Strengthen the capacity of networks and organisations of key affected populations and of people living with HIV to demand better leadership and services, engage in policy dialogue, decision-making and programme design, implementation and M&E, and to hold governments, donors and the UN to account through appropriate technical assistance and organizational development. . Build consensus around indicators and targets for inclusion, empowerment, and community capacity, and for their inclusion in proposals and accountability mechanisms. . Develop a consistent approach to facilitate and fund the involvement of private sector, civil society, people living with HIV, young people, women and key affected populations across the Joint Programme, including in the development of policies, strategies and costed plans, with shared objectives against which progress can be assessed. . Hold ourselves and partners accountable for planning and investing in community capacity development . Facilitate country-led partnerships between government, civil society, community stakeholders, private sector and development partners. . Document and disseminate evidence demonstrating the value, contribution and impact of involving civil society, private sector, people living with HIV and key affected populations in HIV responses.
DRAFT 21 . Support efforts to increase community involvement, including through support for resource mobilisation and inclusion of community systems strengthening in national plans and Global Fund proposals. . Use the experience of the AIDS movement to build coalitions for action to address gaps in the HIV response and to mobilise efforts to achieve the MDGs.
HIV synergies with broader MDG and human development efforts
The effectiveness and sustainability of the HIV response is largely dependent on the success of wider health and development efforts. Moreover, investment in HIV is critical for the strengthening of health systems and achievement of the MDGs. UNAIDS is advocating for an AIDS+MDGs agenda that highlights the essential role of the HIV response in achieving the MDGs and promotes concerted action to maximise impact across multiple MDGs. UNAIDS will:
. Advise countries on integrating HIV into national development plans, poverty reduction strategies and budgets. . Work with international partners to ensure that global policies, strategies and guidelines support full integration of HIV programmes with other health services and to develop common strategies to address health system weaknesses that impact all the health-related MDGs. . Provide technical support for appropriate and cost-effective approaches to programme and service integration in different contexts, including promotion of best practices concerning prevention of mother-to-child-transmission programmes as an entry point to strengthening maternal and child health services, sexual and reproductive rights and health services and primary health care services in general. . Provide technical support to Global Fund proposal and implementation processes to strengthen synergies between HIV and health systems. . Advocate for donors and national governments to meet their commitments to health and development funding. . Build and support collaboration between various networks and movements of health and development actors (e.g. human rights, education, women’s equality, decent and full work) to share lessons learned to improve wider programme implementation and outcomes and to generate momentum for political commitment to the MDGs. . Collaborate with health and development partners to develop indicators to measure progress on the AIDS plus MDG integration as well as composite impact indicators measuring human development . Increase understanding of the ways in which AIDS interacts with poverty and income inequality, human rights, education, gender and other key structural drivers as reflected in the MDGs so as to act decisively on the structural determinants through multi-sectoral, joined up approaches.
V Delivering Results
DRAFT 22 (Note: this section will be updated over the coming months to reflect progress in the implementation of the various Evaluation work streams. Finalization of the following tools is expected by December PCB and will be captured below: Joint Programme Division of Labour; Partnership Strategy; Technical Support Strategy; Knowledge Management Strategy; Human Resources Deployment Strategy; Resource Mobilization Strategy).
UNAIDS has played a significant role in providing leadership for the global response to HIV, mobilising unprecedented political and financial support, strengthening strategic information, supporting country-led responses and galvanising action by a wide range of stakeholders. UNAIDS must, however, change the way it does business if it is to take forward the agenda set out in this Strategic Plan and deliver results in a changing environment.
Strengthening joint working
Guided by a set of core principles24, the Division of Labour (DoL) consolidates how the UNAIDS family collectively implements the Strategic Plans by accentuating the comparative advantages of the Joint Programme as a whole—Cosponsors and Secretariat—and its constituent parts. By leveraging respective organizational mandates and resources, enhancing joint working and partnerships, major efficiencies are gained and transaction costs for countries are reduced.
To strengthen oversight and accountability the DoL identifies a lead organization from among Cosponsors, and where relevant, the Secretariat, for each of 10 areas of the Outcome Framework25. The Lead/Convening26 agencies will guide a given thematic area under the Division of Labour to ensure that the programme needs in that area are identified and addressed through collective work with designated partners for that area.
The designated Partners in a given thematic area will collectively work with the Lead Agency in providing or brokering the required technical and financial programmatic support for that thematic area.
The UNAIDS Secretariat shall exercise responsibility for ensuring the overall functioning and accountability of the Division of Labour, with focus on 1) leadership and advocacy through the generation and use of strategic information, 2) overall coherence, cohesion and coordination across all the thematic areas, and 3) ensure mutual accountability, including the collection and synthesis of key data on the epidemic that reflects the impact of the Joint Programme.
24 25 Maybe more- discussions are underway to extend the areas 26 The Term Lead/Convener has to still to be discussed and agreed
DRAFT 23 In the spirit of national ownership and to ensure sustainability of the response, the DoL will not be rigidly applied at country level, but rather be understood and promoted as a flexible framework to assign roles and responsibilities within the UN system, taking into account the presence and relative strength of individual Cosponsors and the Secretariat on the ground, so as to maximize the effectiveness and impact of UN resources in a country.
Practising more strategic partnership
Partnerships are central to UNAIDS’ capacity to deliver results and integral to successful implementation of this Plan. UNAIDS promotes a strong and consistent strategic direction to its partnerships so as to: 1/ ensure a shared understanding of and commitment to the purposes, responsibilities and accountabilities of UNAIDS partnerships across the Joint Programme at country, regional and global levels; and 2/ leverage technical and financial resources for sustainable, predictable, long term support and to advance results-based country responses that are integral to, and integrated with country-specific efforts, “delivering as one” and principles of efficiency and to maximize the synergies between the main parties involved in the HIV response.
UNAIDS approach to partnerships is guided by the following principles: Focus on delivering results; Recognition that people living with HIV and key affected populations are full partners; A people centred approach; A human rights based approach; Equity and Social Justice; Rigorous use of evidence; Country ownership; and Mutual accountability. The strategy also identifies operational arrangements that include institutional capacity analysis and development, monitoring and evaluation and advocacy and dissemination.
During the plan period, UNAIDS will engage selectively with a broad range of individuals, organizations, networks and institutions that have essential and complementary roles to play in responses to HIV. These partnerships (based on written agreements) and collaborative relationships (based on informal interactions and ongoing relationships) evolve over time. To take forward its Strategic Directions, UNAIDS will strengthen partnerships with community organisations, the research community, organisations and networks working on gender and human rights issues, youth-led organizations and networks, religious and faith-based organizations, parliamentarians, sector ministries responsible for justice and social protection, and the pharmaceutical and diagnostic industries. In line with the core themes of the Strategic Plan, UNAIDS will continue to give high priority to partnerships with civil society and people living with and most affected by HIV and with national governments, and will place more emphasis on strategic partnerships with initiatives working to achieve the MDGs.
[Discuss evolving approach to strategic partnerships with Global Fund and PEPFAR]
Enhancing technical support
DRAFT 24 Technical support is a core function of the UN and the UNAIDS Cosponsors and Secretariat are significant providers of HIV-related technical support. Country requirements for technical support have increased and recent years have seen a proliferation of technical support providers. UNAIDS’ technical support strategy, developed in 2009, has been revised to respond to reflect the priorities in this Strategic Plan.
The new technical support strategy focuses on assisting countries to identify their technical support needs and to manage technical support for maximum impact. UNAIDS will strengthen capacities for coordinating and brokering the provision of technical support, improving the delivery of high quality technical support by UNAIDS and other providers, monitoring the quality and outcomes of technical support. Greater emphasis is placed on building national and regional capacities and systems.
The new strategy also clarifies the comparative advantages and respective roles of the UN, UNAIDS-related technical support mechanisms and other technical support providers in short-term technical support and longer-term capacity building for countries. And, in line with its focus on country priorities and ownership, UNAIDS will ensure that UNAIDS technical support is demand-driven and focused on countries with the greatest needs.
Enhancing the generation and use of strategic information
The Joint Programme plays a normative role as an arbiter of what new research findings are credible, relevant, reliable and valid. UNAIDS provides authoritative advice to countries on policies and strategies, and provides consistent and credible information, analyses, and recommendations for norms, policy development and programming guidance to UN partners and other major partners. UNAIDS’ work on identifying resource requirements and tracking funding has underpinned efforts to mobilise greater financial commitment for the HIV response. UNAIDS has also made an important contribution to the research agenda by identifying gaps in knowledge and advocating for research to address these gaps. To improve its effectiveness and efficiency UNAIDS will develop a new knowledge management strategy to ensure that the Joint Programme meets country needs. The new strategy will promote more coherent and coordinated action across the Joint Programme, improve global tracking of the epidemic and the response, support countries to build evidence for more cost-effective action and to monitor progress, strengthen evaluation and dissemination of good practice, and articulate a clear research agenda.
UNAIDS recognises the need for scientific and strategic inputs to policy formulation and programming at all levels but with a priority focus on countries. UNAIDS is strengthening the capacity of its country and regional staff to support the translation of knowledge into better national policies and strategies. UNAIDS’ Knowledge
DRAFT 25 Management Strategy emphasizes UNAIDS comparative advantage in the following roles: . Generate state-of-the-art, timely, high-quality scientific information and strategic knowledge on the HIV epidemic, its trends, its impact and responses to it, ranging from the human to macroeconomic levels . Build capacity at country level for the definition, compilation, analysis and dissemination of consistent, credible, high-quality scientific information and strategic knowledge . Undertake effective knowledge translation of scientific information relevant to the response to HIV to external partners, including to the general public through the media. Examples include the UNAIDS web site which has a high number of hits, our use of Twitter and Facebook and other social media, and the science blog HIV This Week . Lead knowledge translation in areas that are new, cutting edge, under researched and in which the UN should take a stance. Recent examples include male circumcision, HIV vaccine development, and microbicides. . Address the implementation gap that sees interventions proven effective in clinical and controlled research settings not being translated into successful delivery on the ground, particularly in settings with large HIV epidemics. This means supporting and building capacity in country to increase the number of persons reached with effective programmes for measurable impact on HIV and health outcomes as well as identifying and overcoming the barriers to scaling up . Identify barriers to effective programme performance, and advocating and supporting the creation of generalisable knowledge that can be applied across settings and contexts. This means expanding the knowledge base on: o how to deliver interventions efficiently and effectively o transfer interventions from one setting or population to another o make informed choices between competing interventions
Measuring progress and improving accountability
The Strategic Plan will be regularly monitored and progress in achieving the goals in the Plan will be reported annually to UNAIDS governing board, the Programme Coordinating Board (PCB). A review of the Strategic Plan is expected to take place in 2013 at which point it will be updated or revised, as necessary, to ensure the Strategic Plan remains relevant throughout 2015. Increased efforts will be made to strengthen measurement of results and reporting by the Cosponsors and Secretariat, including through the Committee of Cosponsoring Organisations (CCO). In particular, this will entail alignment of results across global, regional and country levels; use of more harmonised and streamlined indicators, and; involving and holding all stakeholders to account.
A two-year Unified Budget and Accountability Framework (UBAF) will be developed based on the Strategic Plan to provide a simple and transparent mechanism to enhance management, monitoring and reporting on activities and resources of the Joint
DRAFT 26 Programme. The UBAF will replace the current Unified Budget and Workplan, present the expected results of the Joint Programme’s work on HIV and AIDS, and clearly show the contributions of the different Cosponsors and the Secretariat. Commitments will be monitored and evaluated to demonstrate the link between resources and results, especially at country level, and to serve as a basis for future resource allocations. The development of the 2012-2013 UBAF will be guided by a PCB subcommittee, and will involve broad consultation with all stakeholders before it is presented to the PCB for approval in June 2011.
Organizational Change for a more effective Joint Programme
In order to deliver on the Strategic Plan, and for maximum impact of implementing the strategic directions, the UNAIDS Cosponsors and the Secretariat will ensure that the resources made available to the Joint Programme are used in the most cost-effective manner possible and that UNAIDS continues to represents real value for money. To ensure a rational and cost-effective deployment of human resources, the Secretariat and Cosponsors have, for the first time in the history of the United Nations, joined together to analyse the capacity requirements at country and regional levels, and agreed upon the key requirements for UNAIDS staffing – respecting the division of labour, agency mandate, capacities on the ground, and financial resources available.
Using country delivery as the basis for staffing, the Secretariat has initiated measures, that will be implemented throughout the 2011-2015 Plan, to enhance the utilization of resources while improving managerial efficiencies and ensuring flexibility in the provision of the most cost-effective administration services. New corporate strategies, and commensurate policies, have been developed in the areas of finance, human resources, administration, and information management and technology to ensure the most cost-effective investment in the management support to programme delivery. Policies and procedures have been introduced to simplify funding to country teams and joint programmes while enabling closer scrutiny of and accountability for the utilization of all sources of funding.
The Secretariat is also developing a resource mobilisation strategy, which aims to consolidate contributions from existing donors and attract new donors. This will require the Secretariat to strengthen its capacity to raise funds and to monitor and report on donor funds at headquarters, regional and country levels.
The Secretariat will sustain support for UN+, the UN system-wide advocacy group of staff living with HIV, and recently launched a new internal policy on diversity and inclusion, which will ensure that UNAIDS’ guiding principles are put into practice within the organisation.
DRAFT 27 Annex 1. UNAIDS’ ECOSOC Mandate
The UN Joint Programme on HIV/AIDS is mandated by ECOSOC to:
. Provide global leadership in response to the epidemic. . Achieve and promote global consensus on policy and programmatic approaches. . Strengthen the capacity of the UN system to monitor trends and ensure that appropriate and effective policies and strategies are implemented at country level. . Strengthen the capacity of national governments to develop comprehensive national strategies and implement effective HIV/AIDS activities at the country level. . Promote broad-based political and social mobilisation to prevent and respond to HIV/AIDS within countries, ensuring that national responses involve a wide range of sectors and institutions. . Advocate greater political commitment in responding to the epidemic at the global and country levels, including the mobilisation and allocation of adequate resources for HIV/AIDS-related activities.
Annex 2. UNAIDS’ Guiding Principles
(Note: these were developed during the Vision and Mission statement development process, drawing from outcomes of the Bangkok consultation and the online survey, as well as existing materials. They are proposed here as a zero draft).
UNAIDS work is guided by our commitment to: . Human rights UNAIDS works to overcome stigma and discrimination, promote tolerance and uphold the human rights of all people—including the right to HIV prevention, treatment, care and support—and stands in solidarity with people affected by HIV. . Inclusion UNAIDS fosters participatory and inclusive processes that encourage the active participation and engagement of all sectors of society, including people living with HIV, the private sector, academia and the broader civil society. . Partnership UNAIDS expands and optimizes strategic partnerships and networks and leverages the strengths of partners (the United Nations system, governments, civil society, private sector and communities affected by HIV) to maximize the impact and sustainability of AIDS responses. . Measurable, time-bound goals UNAIDS works to achieve the Millennium Development Goals and Universal Access to HIV prevention, treatment, care and support, as well as national and regional health and development goals—and to hold relevant parties to account for their attainment.
28 . Focus on the country level UNAIDS focuses on country-level results and outcomes by supporting nationally-defined priorities, processes and accountability mechanisms. . Evidence UNAIDS is a leading provider of strategic information to guide AIDS responses. UNAIDS puts science, technology and data to work through evidence- informed, context-specific responses to HIV that build on the principles of Know Your Epidemic (KYE). . Efficiency UNAIDS increases the impact and sustainability of AIDS investments and seeks to achieve the highest possible levels of efficiency and effectiveness in our work. . Harmonization UNAIDS responses are consistent with the ‘Three Ones’ principles and reflect a commitment to the goals of national ownership, alignment and harmonization. . Development UNAIDS seeks to integrate AIDS responses with other health and development efforts to maximize health and security for all people and communities at risk. . Empowerment UNAIDS is committed to the empowerment of, and full access to HIV services for, all populations at risk of HIV, including women and girls, young people, orphans and vulnerable children, men who have sex with men, transgender people, sex workers and their clients, people who inject drugs, and for vulnerable people including women and girls, young people, orphans and vulnerable children, persons affected by humanitarian emergencies, and migrants.
Annex 3. Core principles governing the Division of Labour
(i) moving from the concepts of “Division of Labour” to a clustering for results around priority objectives (ii) National ownership and country priorities; (iii) mutual and reciprocal accountabilities; (iv) A differentiation of “Division of Labour” at global, regional and country levels flexibility for the global “Division of Labour” to be adapted to individual Country circumstances taking into account Co sponsors comparative advantage & core mandates of different co- sponsors; in country presence or non-presence of the Secretariat or agencies; existing national capacities; and availability of funding for different functions and priorities at country level (v) Identifying various incentives, other than financial ones, for the Joint Programme to work together to deliver results
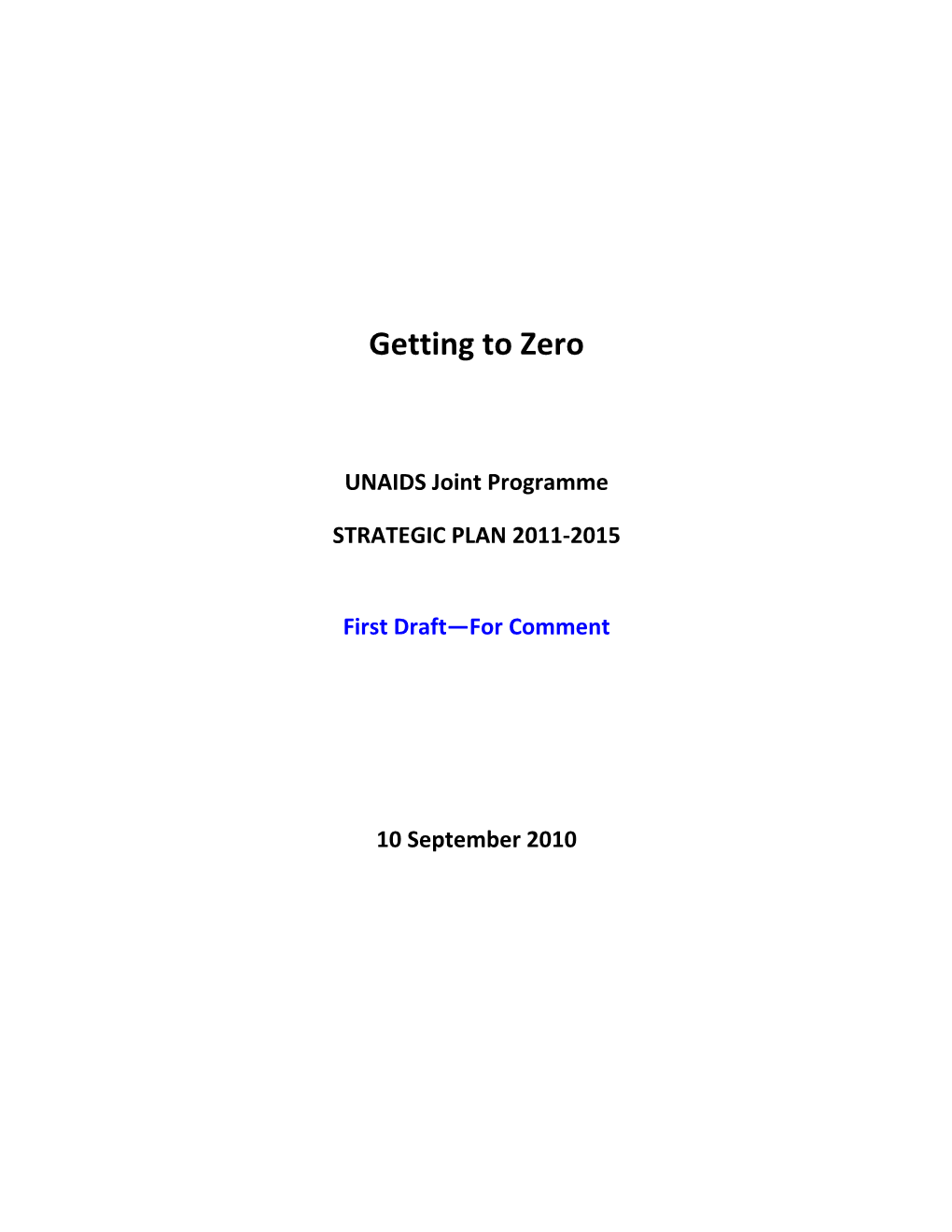
DRAFT 29 DRAFT 30 UNAIDS STRATEGIC FRAMEWORK 2011-2015 DRAFT
V I S I O N Zero Zero new new HIV HIV infections. infections. Zero Zero Discrimination. Discrimination. Zero Zero AIDS-related AIDS-related deaths. deaths.
Achieve Universal Access to HIV prevention, treatment, care and support Achieve Universal Access to HIV prevention, treatment, care and support O A L S Halt the spread of HIV and contribute to the achievement of the MDGs G Halt the spread of HIV and contribute to the achievement of the MDGs
STRATEGIC Revolutionise HIV Catalyse the next phase Put human rights and DIRECTIONS Prevention of treatment, care and gender equality to work for support HIV + ACTION AREAS National commitment to Global commitment to Removal of punitive laws, s effective combination treatment access e prevention responses policies and practices that Better drug regimens, block AIDS response and
m Global commitment and diagnostics and delivery elimination of HIV-related e Country-Focused consensus around HIV
h discrimination Strengthened national prevention T Socially-inclusive, rights- Generation of strategic and community systems to
g HIV+MDG Synergies based HIV responses information deliver HIV treatment, care n
i Supportive, non-stigmatizing and support Innovation in HIV
d social and gender norms i People-Centred prevention science, tools u Reduction of sexual- and and delivery
G gender-based violence
Aligning OF 1/ Reduce sexual transmission 3/ Ensure access to treatment 6/ Empower MSM, TGs and 2/ Prevent mothers dying and 4/Prevent PLHIV dying of TB SWs to prevent HIV and access Priority Areas: babies infected with HIV 10/ Enhance social protection treatment WE CAN 5/ Prevent infection among drug for HIV-affected 7/ Remote punitive laws users 8/ Meet needs of women and 9/ Empower young people to girls & end sex & gender- prevent HIV based violence
31