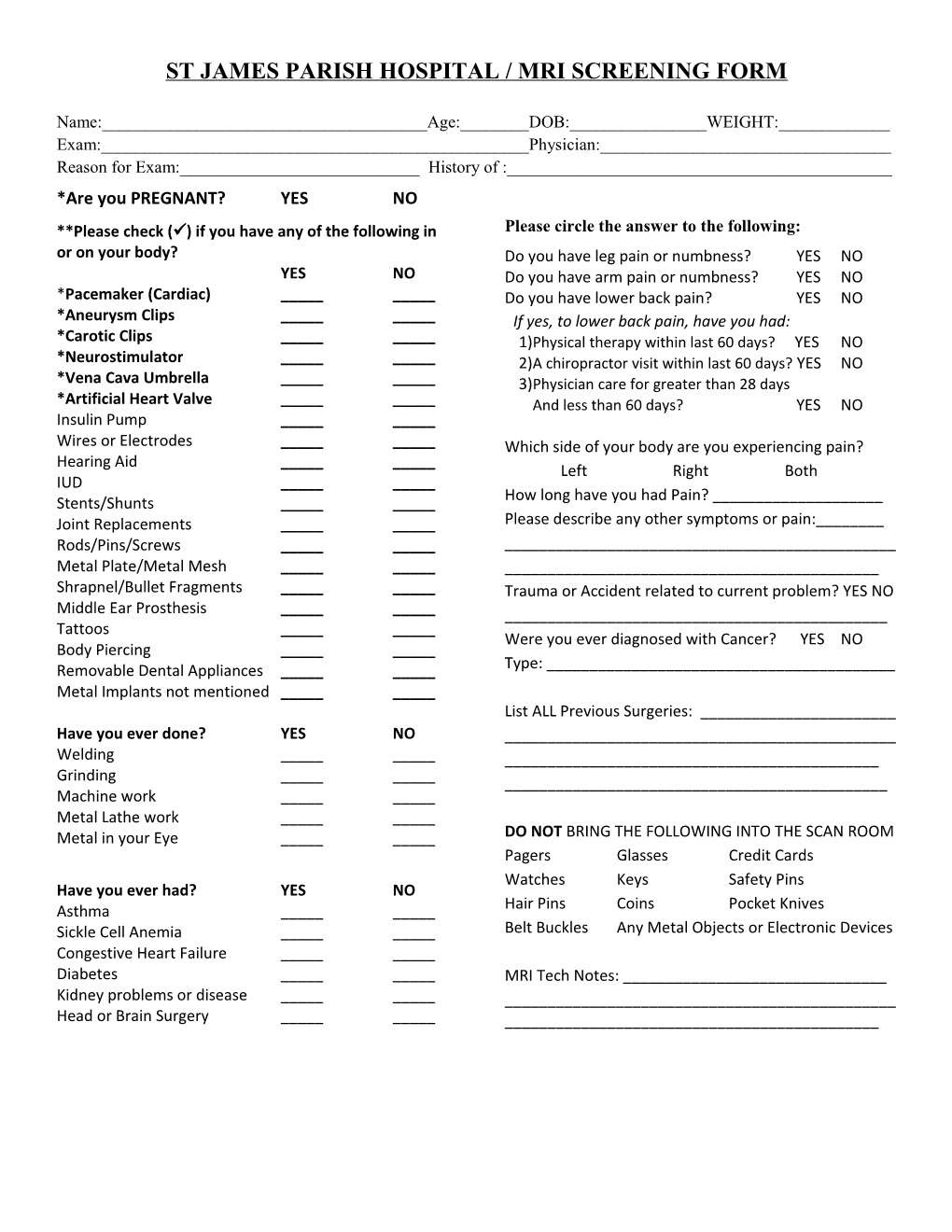
ST JAMES PARISH HOSPITAL / MRI SCREENING FORM
Name:______Age:______DOB:______WEIGHT:______Exam:______Physician:______Reason for Exam:______History of :______*Are you PREGNANT? YES NO **Please check () if you have any of the following in Please circle the answer to the following: or on your body? Do you have leg pain or numbness? YES NO YES NO Do you have arm pain or numbness? YES NO *Pacemaker (Cardiac) ______Do you have lower back pain? YES NO *Aneurysm Clips ______If yes, to lower back pain, have you had: *Carotic Clips ______1)Physical therapy within last 60 days? YES NO *Neurostimulator ______2)A chiropractor visit within last 60 days? YES NO *Vena Cava Umbrella ______3)Physician care for greater than 28 days *Artificial Heart Valve ______And less than 60 days? YES NO Insulin Pump ______Wires or Electrodes ______Which side of your body are you experiencing pain? Hearing Aid ______Left Right Both IUD ______Stents/Shunts ______How long have you had Pain? ______Joint Replacements ______Please describe any other symptoms or pain:______Rods/Pins/Screws ______Metal Plate/Metal Mesh ______Shrapnel/Bullet Fragments ______Trauma or Accident related to current problem? YES NO Middle Ear Prosthesis ______Tattoos ______Were you ever diagnosed with Cancer? YES NO Body Piercing ______Removable Dental Appliances ______Type: ______Metal Implants not mentioned ______List ALL Previous Surgeries: ______Have you ever done? YES NO ______Welding ______Grinding ______Machine work ______Metal Lathe work ______Metal in your Eye ______DO NOT BRING THE FOLLOWING INTO THE SCAN ROOM Pagers Glasses Credit Cards Watches Keys Safety Pins Have you ever had? YES NO Asthma ______Hair Pins Coins Pocket Knives Sickle Cell Anemia ______Belt Buckles Any Metal Objects or Electronic Devices Congestive Heart Failure ______Diabetes ______MRI Tech Notes: ______Kidney problems or disease ______Head or Brain Surgery ______