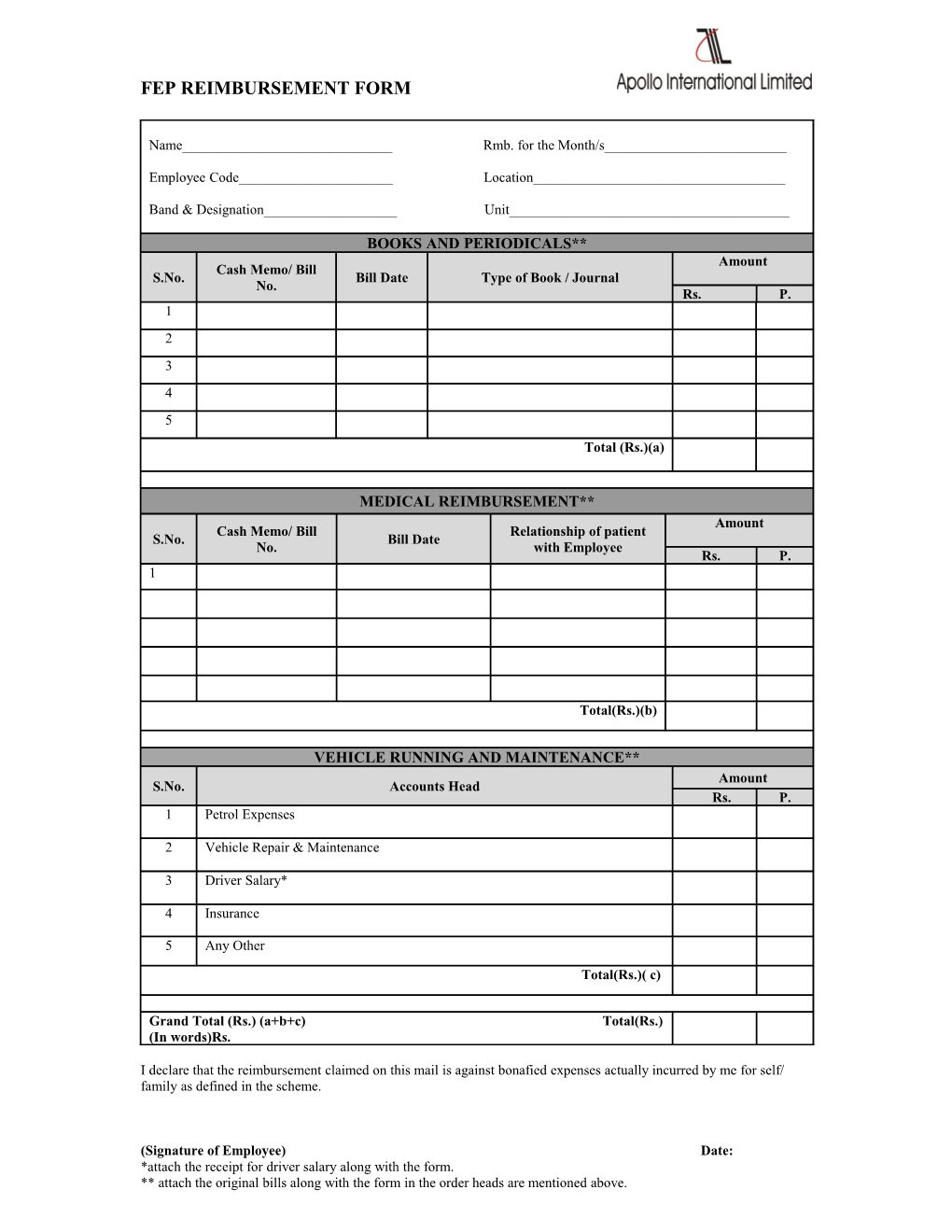
FEP REIMBURSEMENT FORM
Name______Rmb. for the Month/s______
Employee Code______Location______
Band & Designation______Unit______
BOOKS AND PERIODICALS** Amount Cash Memo/ Bill S.No. Bill Date Type of Book / Journal No. Rs. P. 1 2 3 4 5 Total (Rs.)(a)
MEDICAL REIMBURSEMENT** Amount Cash Memo/ Bill Relationship of patient S.No. Bill Date No. with Employee Rs. P. 1
Total(Rs.)(b)
VEHICLE RUNNING AND MAINTENANCE** Amount S.No. Accounts Head Rs. P. 1 Petrol Expenses
2 Vehicle Repair & Maintenance
3 Driver Salary*
4 Insurance
5 Any Other
Total(Rs.)( c)
Grand Total (Rs.) (a+b+c) Total(Rs.) (In words)Rs.
I declare that the reimbursement claimed on this mail is against bonafied expenses actually incurred by me for self/ family as defined in the scheme.
(Signature of Employee) Date: *attach the receipt for driver salary along with the form. ** attach the original bills along with the form in the order heads are mentioned above.