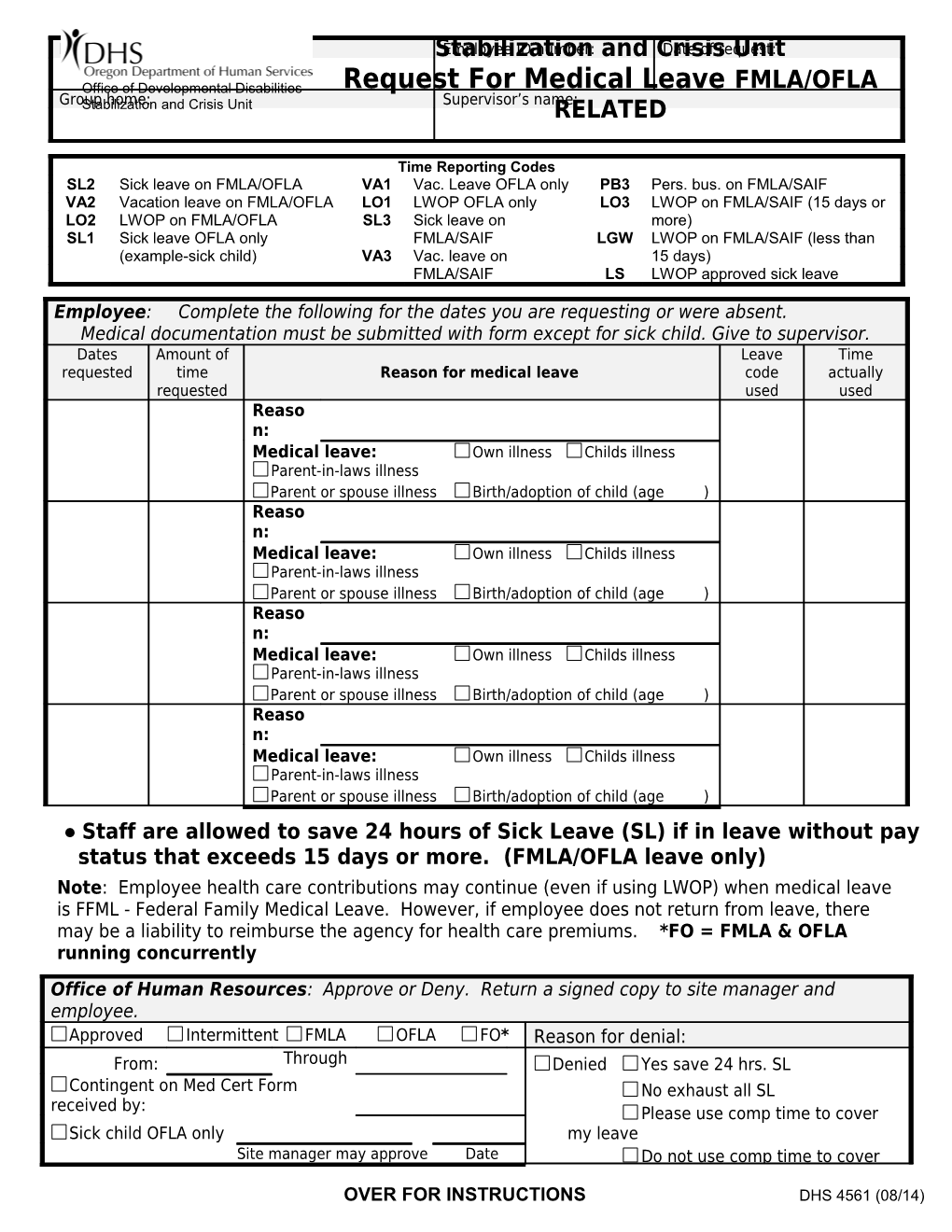
Name: StabilizationEmployee ID number: and CrisisDate of request: Unit
Office of Developmental Disabilities Request For Medical Leave FMLA/OFLA Group Stabilization home: and Crisis Unit Supervisor’s name: RELATED
Time Reporting Codes SL2 Sick leave on FMLA/OFLA VA1 Vac. Leave OFLA only PB3 Pers. bus. on FMLA/SAIF VA2 Vacation leave on FMLA/OFLA LO1 LWOP OFLA only LO3 LWOP on FMLA/SAIF (15 days or LO2 LWOP on FMLA/OFLA SL3 Sick leave on more) SL1 Sick leave OFLA only FMLA/SAIF LGW LWOP on FMLA/SAIF (less than (example-sick child) VA3 Vac. leave on 15 days) FMLA/SAIF LS LWOP approved sick leave
Employee: Complete the following for the dates you are requesting or were absent. Medical documentation must be submitted with form except for sick child. Give to supervisor. Dates Amount of Leave Time requested time Reason for medical leave code actually requested used used Reaso n: Medical leave: Own illness Childs illness Parent-in-laws illness Parent or spouse illness Birth/adoption of child (age ) Reaso n: Medical leave: Own illness Childs illness Parent-in-laws illness Parent or spouse illness Birth/adoption of child (age ) Reaso n: Medical leave: Own illness Childs illness Parent-in-laws illness Parent or spouse illness Birth/adoption of child (age ) Reaso n: Medical leave: Own illness Childs illness Parent-in-laws illness Parent or spouse illness Birth/adoption of child (age ) ● Staff are allowed to save 24 hours of Sick Leave (SL) if in leave without pay status that exceeds 15 days or more. (FMLA/OFLA leave only) Note: Employee health care contributions may continue (even if using LWOP) when medical leave is FFML - Federal Family Medical Leave. However, if employee does not return from leave, there may be a liability to reimburse the agency for health care premiums. *FO = FMLA & OFLA running concurrently
Office of Human Resources: Approve or Deny. Return a signed copy to site manager and employee. Approved Intermittent FMLA OFLA FO* Reason for denial: From: Through Denied Yes save 24 hrs. SL : Contingent on Med Cert Form No exhaust all SL received by: Please use comp time to cover Sick child OFLA only my leave Site manager may approve Date Do not use comp time to cover
OVER FOR INSTRUCTIONS DHS 4561 (08/14) Office of Human Resources Signature Date Employee’s signature Date
FMLA HOURS AVAILABLE as of -> Date OFLA HOURS AVAILABLE as of -> Date
INSTRUCTIONS
This form must be filled out, signed and dated by all employees who are absent due to the following FMLA/OFLA reasons only and faxed to the Office of Human Resources at:
Fax # 503-945-5866
1. Any employee who is out “Continually” (exceeding 3 days or more) or has a foreseeable absence in the future due to a FMLA/OFLA qualifying condition, must fill out, sign and date this form and return to Human Resources within 2 days of beginning the leave or within 2 days of returning to work.
2. Any employee who is approved for ‘‘Intermittent” FMLA/OFLA leave must fill out, sign and date this form for each absence relating to the approved intermittent leave and return to Human Resources within 2 days of returning to work.
3. Any employee who is absent due to “Sick Child” leave must fill out, sign and date this form within 2 days of returning to work and submit to manager for approval. Manager will notify Human Resources.
If you have questions, please call 503-945-6378
OVER FOR INSTRUCTIONS DHS 4561 (08/14)