Summary of Evidence Table – Definition of DBI
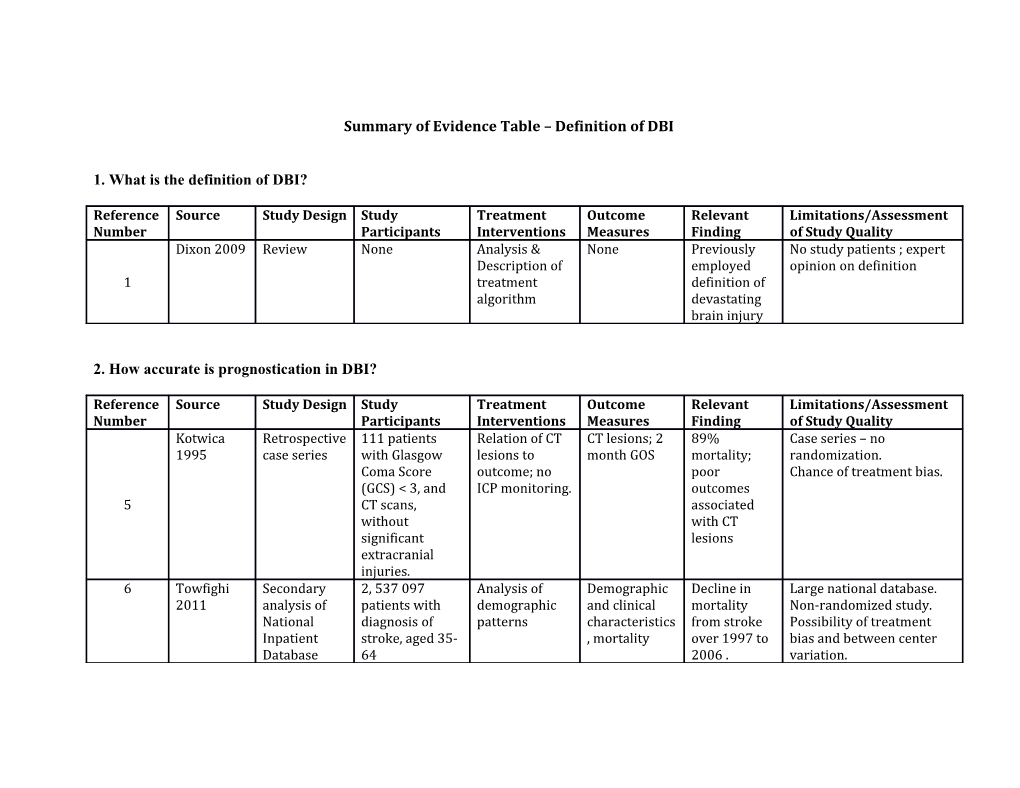
1. What is the definition of DBI?
Reference Source Study Design Study Treatment Outcome Relevant Limitations/Assessment Number Participants Interventions Measures Finding of Study Quality Dixon 2009 Review None Analysis & None Previously No study patients ; expert Description of employed opinion on definition 1 treatment definition of algorithm devastating brain injury
2. How accurate is prognostication in DBI?
Reference Source Study Design Study Treatment Outcome Relevant Limitations/Assessment Number Participants Interventions Measures Finding of Study Quality Kotwica Retrospective 111 patients Relation of CT CT lesions; 2 89% Case series – no 1995 case series with Glasgow lesions to month GOS mortality; randomization. Coma Score outcome; no poor Chance of treatment bias. (GCS) < 3, and ICP monitoring. outcomes 5 CT scans, associated without with CT significant lesions extracranial injuries. 6 Towfighi Secondary 2, 537 097 Analysis of Demographic Decline in Large national database. 2011 analysis of patients with demographic and clinical mortality Non-randomized study. National diagnosis of patterns characteristics from stroke Possibility of treatment Inpatient stroke, aged 35- , mortality over 1997 to bias and between center Database 64 2006 . variation. Better survival among women compared with men.
Ovbiagele Secondary Patients with Analysis of Demographic Stroke Large national database. 2010 analysis of stroke from demographic and clinical hospitalization Non-randomized study. National 1997-2006 patterns characteristics s decreased Possibility of treatment Inpatient , mortality from 1997 till bias and between center Database 2006. variation. Mortality 7 decreased from 11.5% in 1997-98 to 10.3% in 2005-06.
Arabi, 2010 Single center, 434 comatose Implementatio Hospital Use of Standardized methods of comparison patients with n of Brain mortality, ICU protocol therapy, without specifying of mortality TBI, older than Trauma mortality, associated degree of adherence - pre- and 12 years Foundation tracheotomy with potential for treatment post- guidelines rate, duration reduction in bias. implementati based Protocol of mechanical hospital and Comparison between 8 on of ventilation, ICU mortality, historical cohorts – time treatment length of ICU without effect. protocol and hospital increase in Prospectively collected stays. survival with data. severe disability 9 Sturgeon Secondary Stroke cases in Analysis of Hospitalizatio Total stroke Retrospectively collected 2007 analysis of Minneapolis-St demographics n, mortality and data. Large regional regional Paul , older than and outcome demographics, hospital case database, with potential hospital 29 years, in mortality fatality for treatment and ICD-9 association 1980-2002 declined by up diagnosis variability database to 50% over the period Andaluz Secondary Patients with Analysis of In hospital Mortality Large national database. 2008 analysis of SAH from 1993 demographic mortality, declined by Non-randomized study. National to 2003 patterns routine 20% for SAH Possibility of treatment Inpatient discharge and by 50% for bias and between center Database (good unruptured variation. Discharge aneurysms. outcome), disposition used as 10 Clipping non-routine procedures did surrogate for outcome discharge not increase, (poor but outcome), endovascular Length of stay procedures doubled. Parry-Jones Retrospective 1364 patients Testing Clinical and Mortality Single center referral 2013 review of with ICH from accuracy of ICH demographic reported at database with possibility of prospective Jan 2008 till Oct grading scales factors, CT around 50%. bias. Blinded to ICH scores database 2010 against scan – ICH (& Age was poor during treatment. 11 outcome modified) predictor. GCS most score, ICH predictive part grading scale. of scale. 30 day mortality 12 Lu 2005 Secondary 1839 patients, Assessment of Clinical and Mortality in Amalagam of different analysis of GCS 3-8, aged changes in demographic the year 1984 databases, including combined 16-65 yrs over outcome over characteristics equaled 39% clinical trial. Differing multiple period of 1984- time , mortality and gradually protocols of care, and databases 1996. rate. decreased possibility of between to a level of 27% in 1996. center bias. Significant change despite controlling for age, gender, race, cause of injury, admission pupillary response and motor score
3. What is the impact of early prognostication (before 72 hours)?
Reference Source Study Design Study Treatment Outcome Relevant Limitations/Assessment Number Participants Interventions Measures Finding of Study Quality Massagli Retrospective 75 patients less Association of Abstracted Late outcome Small cohort in study. 1996 cohort than 17 years, indices of GOS at 5- 7 significantly Retrospective indirect with GCS < 8, traumatic brain yrs after associated determination of GOS. over Jan 1985 to injury in injury. with head AIS Single center. Dec 1986 children with score, ISS outcome at score, pupils hospital in the field, 14 discharge, and GCS scores at 5 to 7 years 24 and 72 later. hours, length of coma, site of discharge, and early GOS scores. 15 Gatson Prospective 18 patients with Correlation 6 month CSF oligomer Small study. Single center. 2013 observational TBI and GCS<9, between CSF Extended GOS, levels within No breakdown of CSF cohort study with beta-amyloid Disability 72 hours sampling times. ventriculostomy oligomers and rating scale correlated GOS at 6 (DRS) with GOS-E, months and DRS Chabok Prospective 28 patients GCS Serum S100B CSF sampling Increased Small study – 2012 observational < 9, with diffuse and Neuron at 6,24, 48 and levels of NSE nonrandomized, selected study axonal injury, specific enolase 72 hours. and S100B at study population, with over March (NSE) levels in Mortality by 72 hours are possibility of bias. 16 2008 to May relation to GOS time of associated 2009 discharge, GOS with poor at 3 months outcome and 2 years Settervall Prospective 277 patients > Comparison of Clinical Hospital Single center study, 2011 cohort study 14 years old predictive demographics, mortality exclusion of extracranial with TBI accuracy of hospital related to all injuries in model admitted to initial, best, and mortality three scores – trauma center worst GCS over strongest within 12 hours first 72 hours. association 17 of injury, over with best December 2006 score, but no and October significant 2007 differences between scores. Eriksson Retrospective 32 patients with Comparison of Clinical pBrO2 less Small study –heterogenous 2012 case series severe TBI and pBrO2, ICP and demographics than 299 injuries, dispersed ISS, brain tissue CPP in , hospital mmm Hg variability in time of oximetry survivors and mortality over first 72 insertion 18 monitoring non-survivors hours was Single center study (pBrO2), over predictive of Retrospective data January to July mortality 2008 19 Kahraman Retrospective 30 patients >14 Assessment of Clinical PTD for CPP Standardized protocol of 2011 case series years with effect of demographics > 100 after care review of severe TBI, GCS accumulated , in hospital first 24 hours Retrospective data prospectively < 9, admitted ICP and CPP mortality, was most Model did not include collected data within 6 hours insults over discharge GCS, significantly therapeutic intensity of injury, with time (pressure length of ICU predictive of ICP monitoring x time dose and hospital mortality [PTD]– stays, 3 month measured extended GOS automatically and manually) , with outcome Van Prospective 57 TBI patients Serial Clinical CBFV Standardized treatment Santbrink cohort study with GCS<9 assessment of demographics reduction protocol. 2002 transcranial 6 month GOS. associated Nonrandomized. Doppler with poor Possible selection bias. estimated outcome. Small study. cerebral blood Reduced flow flow is most 20 velocity(CBFV), evident and ipsilateral to relationship focal injury with outcome, concentrating on first 72 hours 21 Wolach Prospective 14 males aged Evaluation of Humoral and Severe brain Small numbers, non- 2001 cohort study 16-65 years immunological cellular injury randomized with with TBI, and defects within immunological induces possibility of selection GCS < 8 72 hours of function, significant bias . TBI, compared complicating immune Single center. healthy infections, deficiency controls and mortality and within 72 with previous consciousness hours. study on (up to 6 Cellular persistent months) function most vegetative state compromised . Effect does not persist beyond months. Togha 2004 Retrospective 122 patients Exploration of Clinical One third of Single center. No case series with primary mortality and demographics, deaths withdrawal of support. intracerebral associated in-hospital occurred hemorrhage(IC features in mortality within first H), admitted patients with two days between May ICH. after brain 1999 and April injury. In 2002 hospital mortality 22 associated with admission GCS, hematoma volume, diabetes, and intraventricul ar hematoma 23 Becker Retrospective 87 patients with Exploration of Demographics, Clinical CT scan reviewers blinded 2001 case series. supratentorial mortality and radiologic and communicati to clinical data. ICH over 1994- associated clinical on of Single center study, with 97. features in variables, prognosis no controls to accurately patients with discharge was at odds assess variability between ICH. status, in with providers. Surgery very hospital prognostic likely subject to selection mortality, models and bias surgical most intervention, significantly withdrawal of affected support withdrawal of support decisions and subsequent outcome O’Callahan Prospective 47 patients To determine Clinical Life support Single center study. 1995 cohort study aged 18 to 83 frequency of variable, withdrawn in Interviewed residents years, with withdrawal of predicted over 50% of rather than attendings. severe head support in prognosis and patients. Non-randomized study. injury over 12 patients with contributing Prognosis month study severe head factors, based on period injury, with outcome judgment (as relationship to opposed to 24 prognostic scoring accuracy and systems) of communication neurologic with families function. Families generally agreed with physicians assessment. 25 Tien 2006 Retrospective 245 patients , Comparison of Clinical Patients with Excluded use of paralytics case series aged 15-90 mortality with demographics; GCS 3 and and legal intoxicants only. review years admitted reactive pupils in-hospital bilateral fixed Single center. No with blunt death dilated pupils standardized protocol. injury and an had 100% Probable selection and admission GCS mortality. treatment bias. of 3 over Patients with January 2001 to reactive December 2003 pupils had 42% mortality, but were more likely to receive surgical treatment Brody 2010 Retrospective 68 patients with Factors Clinical 48% not Small sample size. case series fatal gunshot affecting demographics, admitted to Concerns of inconsistent review wounds(GSW), frequency of hospital ICU and record keeping. over September organ donation disposition, expired in 2003 to organ ED. Only 18% September 2008 donation of those 26 received vasopressors. Identified missed donor opportunities .
4. What factors identify patients at high risk for death due to brain injury?
Reference Source Study Design Study Treatment Outcome Relevant Limitations/Assessment Number Participants Interventions Measures Finding of Study Quality 27 Combes Prospective 198 patients Association of Abstracted Late outcome Small cohort in study. 1996 cohort less than 17 indices of GOS at 5- 7 significantly Retrospective indirect years, with GCS traumatic brain yrs after associated determination of GOS. < 8, over Jan injury in injury. with head AIS Single center. 1985 to Dec children with score, ISS 1986 outcome at score, pupils hospital in the field, discharge, and GCS scores at 5 to 7 years 24 and 72 later. hours, length of coma, site of discharge, and early GOS scores. 28 Murano Retrospective 298 patients Analysis of Clinical In-hospital Single trauma center – 2005 case series with GSW to clinical data to demographics, mortality was referral pattern may confer head, presenting determine trajectory 51 per cent. selection bias. Extracranial to a level 1 predictors of Admission injuries contribute to trauma center death GCS <5 and mortality and may between ISS >25 were confound. No exact data January 1992 to associated on mode of death December 2003 with (withdrawal vs mortality. progression to death) 7% of survivors had admission GCS of 3. Respiratory arrest or hypotension on admission, along with transhemisph eric and transventricu lar trajectories were all predictors of death, but not absolute. Bershad Retrospective 248 patients Analysis of Clinical Acute Retrospective 2008 case series with subdural effect of demographics, Physiology observations. No hemorrhage coagulopathy in hospital And Chronic standardized protocol for (SDH) admitted on outcome mortality Health reversal of coagulopathy to Evaluation Single center. Aggressive Neurosciences (APACHE) III INR target. No CT scan ICU over score and data. January 1997 to coagulopathy December 2001 independentl 29 y predicted in-hospital death, while surgical evacuation was associated with reduced in-hospital deaths 30 Park 2009 Retrospective 672 patients Accuracy of Clinical Both scales Retrospective data. Single case series with SAH or TBI Simplified demographics; overpredicte tertiary care center. No admitted to Acute In-hospital d mortality. data on state prior to Neurosurgical Physiology mortality SAPS II was admission including ICU over July Score (SAPS) II independent transfer from other 2003 to June and APACHE II predictor in centers. 2005 scoring SAH only, systems in while both predicting scales were mortality in 1st predictive in 24 hours of TBI. TBI admission patients are more affected by systemic insults than SAH patients, 31 Labib 2011 Retrospective 276 patients Analysis of Clinical Falls were Retrospective data. Single Registry over 65 with ISS geriatric demographics; principal tertiary care center. No review > 15 admitted to mortality after In-hospital cause of data on state prior to Canadian Level severe injury mortality injury, while admission including 1 trauma center intubation, transfer from other between blood centers. January 2004 to transfusions, December 2006 and trauma to head, C- spine, or chest were all associated with risk of death. Subsequent respiratory, gastrointestin al, or infectious complication s were associated with in- hospital mortality (26.8%), which was comparable with US National Trauma Data Bank. Mortality was not different either side of 80 years of age.
32 Cho 1997 Retrospective 200 patients . 13 Analysis of Clinical No Retrospective data. Single case series years with acute predictive demographics; differences center. Possible selection head injury, power of GCS, In-hospital between bias for surgical treatment admitted to and APACHE II mortality scoring but no influence of surgery neurosurgical and III, in systems on on outcome model. ICU over relation to hospital September 1992 hospital mortality, but to December mortality and APACHE III 1994. functional and II outcome. predicted death and functional outcome more accurately after 14 days. Physiologic derangement and comorbidities seem to be most relevant in later period after injury. Alvarez Secondary Secondary Comparison of Clinical MPM II Same database used to 1998 analysis of analysis of 401 APACHE II, demographics; provide best create MPM II. No uniform European – patients with SAPS II, and In-hospital prediction. protocol of care. Possible North head trauma, Mortality mortality APACHE II selection and treatment American ICU admitted to 12 Probability and SAPS II bias. 33 study European/ Models (MPM) did not North American II, as well as calibrate ICU’s. GCS, in well, and predicting underpredict mortality ed mortality 34 Hyam 2006 Secondary 11,021 patients Comparison of Clinical The ICNARC Explicit variable analysis of with TBI within SAPS II, MPM II, demographics, model, SAPS definitions, data collection Intensive ICNARC APACHE II and outcome on II and MPM II training for observers, and Care National database, III and the discharge have superior use of objective variables Audit and composed of ICNARC model from ICU, and calibration limiting scope for inter- Research 374,594 plus raw GCS discharge and observer error Centre admissions to from hospital discriminatio (ICNARC) 169 general n compared database ICUs and 5,743 to APACHE II admissions to and III in TBI two although neurosurgical none had units, over perfect December 1995 calibration to May 2005 Lowest GCS in the first 24 hours in ICU discriminated well when available, but could not be objectively assessed for 57% of admissions Dalgic 2009 Review of 266 patients Comparison of Clinical APACHE II is Retrospective data; single retrospective with TBI and APACHE II and demographics, superior to center; used initial GCS on case series systemic trauma GCS in mortality GCS for ICU admission and in 2003 and predicting prediction of approximated Verbal 35 2004 mortality in mortality in scores in intubated TBI plus multitrauma patients. systemic patients, Possible selection and trauma treatment bias 36 Ivascu, Retrospective 109 patients, Analysis of Clinical ASA and Retrospective data; single 2008 case series age 50 or interaction of demographics, clopidogrel center. Possible selection review greater, with CT antiplatelet mechanism of are both and treatment bias, evidence of agents with injury, associated especially with regard to ICH, while traumatic ICH (GCS), with high use of platelet transfusion taking ASA, on mortality, grading of mortality, clopidogrel, or and assess head secondary to both, over effect of CT scans, and initial August 1999 to treatment. outcomes hemorrhage November 2004 and comorbidities rather than extension of bleeding – in contrast to warfarin. The initial GCS and hemorrhage on CT scan are most predictive of death. Progression of hemorrhage after admission is unusual Zafonte Retrospective 27 patients > 16 Effect of Functional Rehabilitatio Small number. 2001 review of years, comatose inpatient Independence n was Retrospective data; single case series with severe TBI rehabilitation Measure, associated center. Non-randomized admitted to on Disability with study with possible level I trauma outcome, after Rating Scale, improved selection and treatment 37 center within 24 GSW to the and length of outcome in bias hours of injury, head. stay survivors. between December 1989 and April 1999 38 Arboix Secondary 184 patients Analysis of Clinical Fischer score, Retrospective data with 1999 analysis of with non- clinical demographics. progressive patients accrued over a 16 prospective traumatic SAH predictors of mortality neurological year period = small yearly Barcelona admitted to two in-hospital deficit and number. Stroke Spanish mortality limb Registry hospitals within the first weakness between 1977 72 hours of were and 1993. admission independent predictive factors of death within 72 hours in patients with non- traumatic SAH Zhang 2011 Retrospective 155 patients > Assessment of Clinical Poor Hunt– Single center. review of 18 years, possible risk demographics. Hess grade, Retrospective data. case series admitted to factors for in-hospital presence of Possible treatment bias. hospital within fever and its mortality IVH and older 7 days of SAH, influence on in- age were from January hospital independent 2006 to 2009, mortality predictors of fever. In- 39 hospital mortality was associated with fever,unconsc iousness on admission and older age. 40 Arboix Secondary 393 patients Analysis of the Clinical Higher Retrospective review. 2000 analysis of with diabetes in effect of demographics. incidence of Limited follow-up of 1840 patients larger stroke diabetes on in-hospital atherothrom outcome. in stroke registry, ischemic stroke mortality botic stroke registry. between and and lacunar January 1986 determining infarction in and December predictors of patients with 1997. in-hospital diabetes. No mortality. significant effect of diabetes on mortality. Patient's age, decreased consciousnes s, chronic nephropathy, congestive heart failure and atrial fibrillation were all predictors of in-hospital mortality. 41 Fanshawe Retrospective 61 patients Examine ICU, in- Intensive Small study numbers. 2002 review admitted to the mortality rate hospital and care Retrospective data. ICU with the and the three-month admission Possible selection bias for diagnosis of functional mortality; was admission to ICU – no stroke, outcomes of functional associated standardized criteria. excluding SAH, stroke patients, outcome with a high between along with mortality rate January 1994 predictors of and a high and December poor outcome likelihood of 1999. dependent lifestyle after hospital discharge. Haemorrhagi c stroke, fixed dilated pupil(s) and GCS <10 during assessment were associated with increased mortality and poor functional outcome. Cucchiara Secondary 564 patients Assessment of Clinical Initial Retrospective data. 2004 analysis of with anterior predictive demographics, decreased Dichotomous placebo arm circulation power of a level 30 day level of categorization of edema of stroke, without of mortality consciousnes and midline shift rather multicenter impaired consciousness s, than continuous effect. No drug trial consciousness at score on independentl cardiopulmonary data baseline, and outcome. y after admission. enrolled within predicts 42 12 hrs of mortality symptom onset within the initial hours after onset of major anterior circulation ischemic stroke. 43 Smith 2010 Derivation 274 988 Assessment of Clinical Predictors Trained abstractors. and ischemic stroke factors demographics; of increased Consistent data entry tool validation patients from predicting risk in hospital mortality with standardized data study 1036 hospitals for in-hospital mortality. were definitions and detailed between ischemic stroke increasing coding instructions. Data October 2001 mortality. age (for quality monitored for and December each year completeness and 2007, excluding greater than accuracy. hemorrhagic 60), atrial stroke or fibrillation, transient coronary ischemic attack artery disease, diabetes mellitus, and peripheral vascular disease. Reduced risk of mortality was associated with history of previous stroke or transient ischemic attack, known carotid stenosis, hypertension, dyslipidemia, current smoking, and presentation during regular weekday hours 44 Savadi- Retrospective 238 patients Comparison of Clinical Overall Retrospective data. Oskouei case series. from 13 to 88 consciousness demographics; mortality Possible selection and 2010 years with ICH level with CT CT data; prediction treatment bias. from 2002 to hemorrhage mortality. was better 2005. size, location, with level of and consciousnes intraventricula s, rather than r penetration CT size and location Rordorf Retrospective 63 patients with Prediction of Clinical Leukocytosis, Retrospective data, 2000 cohort study. ischemic stroke death after demographics; renal including calculation of ischemic stroke in hospital function, and APACHE scale. Possible using APACHE mortality. temperature selection and treatment 45 II as bias. components of APACHE II predicted death