NICHOLLS STATE UNIVERSITY UNIVERSITY OF LOUISIANA SYSTEM FACULTY, STAFF AND DEPENDENTS FEE EXEMPTION POLICY
The exemption policy became effective at our University for the Fall1982 semester. The revised policy became effective March 4, 2013.
The revised policy can be found in the Nicholls State University Policy and Procedure Manual which can be found at http://www.nicholls.edu/documents/nicholls/NSU_Policy_Procedures_M.pdf -Tuition Waiver or at the University of Louisiana System website at www.ulsystem.net
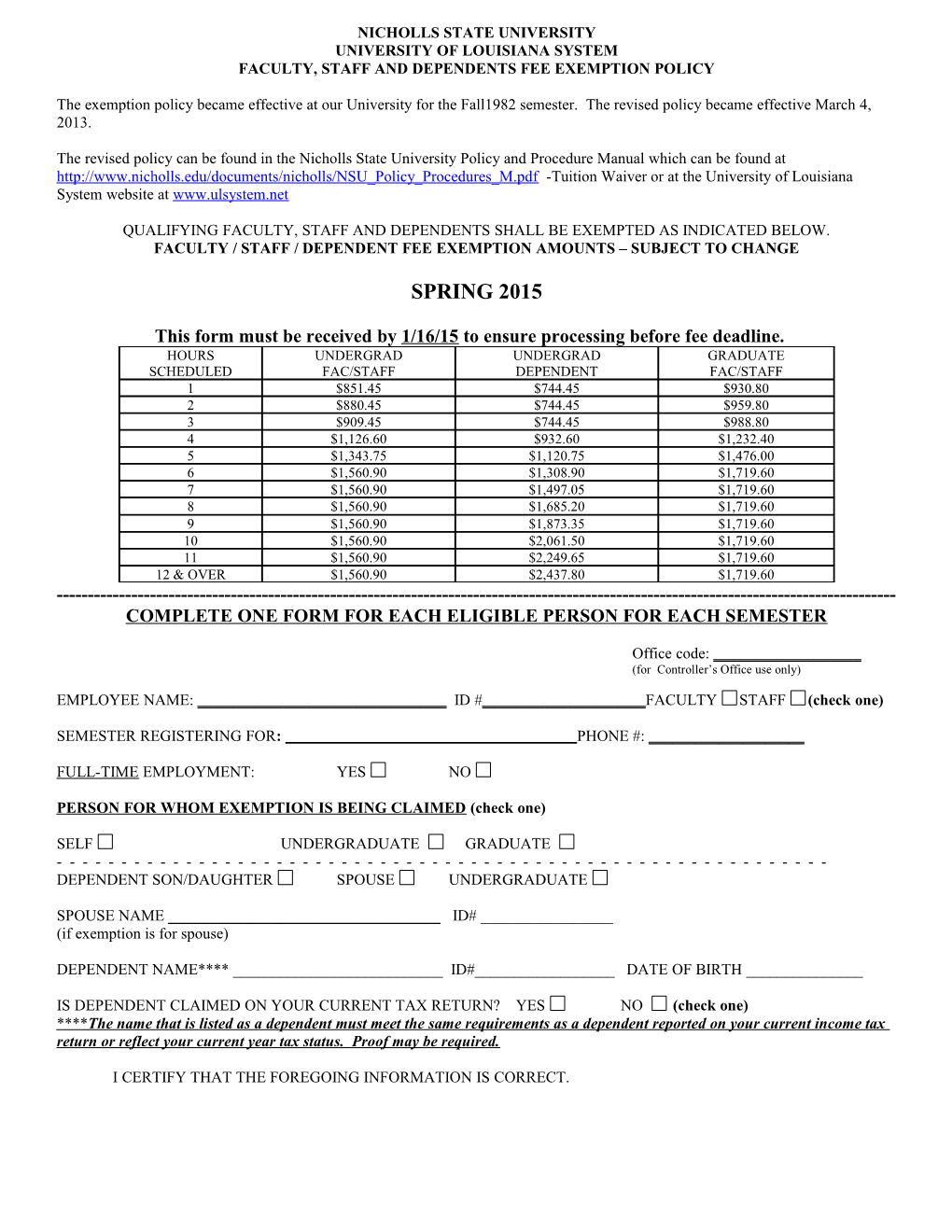
QUALIFYING FACULTY, STAFF AND DEPENDENTS SHALL BE EXEMPTED AS INDICATED BELOW. FACULTY / STAFF / DEPENDENT FEE EXEMPTION AMOUNTS – SUBJECT TO CHANGE
SPRING 2015
This form must be received by 1/16/15 to ensure processing before fee deadline. HOURS UNDERGRAD UNDERGRAD GRADUATE SCHEDULED FAC/STAFF DEPENDENT FAC/STAFF 1 $851.45 $744.45 $930.80 2 $880.45 $744.45 $959.80 3 $909.45 $744.45 $988.80 4 $1,126.60 $932.60 $1,232.40 5 $1,343.75 $1,120.75 $1,476.00 6 $1,560.90 $1,308.90 $1,719.60 7 $1,560.90 $1,497.05 $1,719.60 8 $1,560.90 $1,685.20 $1,719.60 9 $1,560.90 $1,873.35 $1,719.60 10 $1,560.90 $2,061.50 $1,719.60 11 $1,560.90 $2,249.65 $1,719.60 12 & OVER $1,560.90 $2,437.80 $1,719.60 ------COMPLETE ONE FORM FOR EACH ELIGIBLE PERSON FOR EACH SEMESTER
Office code: ______(for Controller’s Office use only)
EMPLOYEE NAME: ______ID #______FACULTY STAFF (check one)
SEMESTER REGISTERING FOR: PHONE #: ______
FULL-TIME EMPLOYMENT: YES NO
PERSON FOR WHOM EXEMPTION IS BEING CLAIMED (check one)
SELF UNDERGRADUATE GRADUATE ------DEPENDENT SON/DAUGHTER SPOUSE UNDERGRADUATE
SPOUSE NAME ______ID# ______(if exemption is for spouse)
DEPENDENT NAME**** ______ID#______DATE OF BIRTH ______
IS DEPENDENT CLAIMED ON YOUR CURRENT TAX RETURN? YES NO (check one) **** The name that is listed as a dependent must meet the same requirements as a dependent reported on your current income tax return or reflect your current year tax status. Proof may be required.
I CERTIFY THAT THE FOREGOING INFORMATION IS CORRECT. X______07/02/2014 Signature of Faculty or Staff Member