Michigan Congenital Heart Center Workflow C.S. Mott Children’s Hospital University of Michigan Health System Final Report
Prepared For: Shaney Bowers, Clinic Manager Inter., UMHS, Client Jackie Lapinski, C&W Administrative Manager, UMHS, Coordinator Dale Jackson, MQS Fellow, UMHS, Coordinator Mark Van Oyen, Professor of IOE, College of Engineering, Instructor
Prepared By: Team 4 Luca Capicchioni Kevin Hergenreder Morgan Kelley Frank Talbot
April 22, 2014 Table of Contents
List of Tables & Figures Table E-1: Average Waiting Time for Clinic Patients:...... 2 Table E-2: Queuing Analysis Results...... 2 Table 1: Average Waiting Time for Clinic Patients...... 8 Chart 1: Patient Satisfaction Survey Results...... 9 Chart 2: Barriers to On-Time Arrival for Patients...... 9 Table 2: Queuing Analysis Results...... 10
22 Executive Summary
The Michigan Congenital Heart Center (MCHC) is a referral clinic at the University of Michigan Health System (UMHS) that treats patients of all ages that possess a congenital heart condition. The center includes multiple types of testing and care services. Some services, particularly echo and EKG, serve hospital inpatient units on both a scheduled and emergency basis; therefore, MCHC staff must occasionally leave the center to treat patients. These two factors make it difficult to schedule testing. Leadership at MCHC has expressed concerns over the workflow of the clinic due to the impact on overall satisfaction as well as visit volume and revenue. Workflow and patient wait times are specific concerns of the clinic manager. The clinic manager asked an IOE 481 team from the University of Michigan to identify ways to optimize workflow and efficiency to improve the patient experience and productivity through analysis and benchmarking.
The clinic manager speculates that the cause of workflow related issues are lack of standardization and lack of communication throughout the system. To determine why current workflow is inefficient and how to standardize the process, the student team performed the following tasks: conducted a series of observations and studies on each step of the process, performed engineering analysis to optimize flow, identified areas for improvement. With this information, the team developed recommendations to: improve the productivity of the staff, minimize wait time and the total time for each patient, standardize relevant processes that take place at the center, and improve patient and employee satisfaction.
Methods and Findings The team performed a variety of tasks to examine and improve the clinic workflow.
Literature Search The team conducted a literature search online. The team found that many tools exist to aid in process improvement in the outpatient clinic setting, such as MCHC [1].
Shadowing and Observations The team shadowed and observed all processes and staff in the clinic. The findings were an understanding of the processes, key parties involved, and general roles and responsibilities regarding clinic workflow. For example, the team found that echo was a source of frustration for the clinic staff since it seems that most delays result from this service. The information was the basis for the value stream map.
Value Stream Mapping The team created a value stream map, attached in Appendix B, to analyze the current workflow of the clinic. A member of each type of staff reviewed this map and provided feedback. Through the value stream mapping, the team identified the general clinic flow, which simplified the patient flow process and accounted for variation. Delays and other common issues were noted on the map. The team found how communication and standardization missing from the process was impacting flow.
Surveys The team created and distributed a patient-survey to obtain feedback on the clinic experience and quantify waiting time. From the 76 surveys collected, total wait time was found to be 71 minutes with a considerable standard deviation. The breakdown of these results is shown below in Table E-1. Although they complained of wait times, 97% of patients reported they were either satisfied or very satisfied with their visit.
Table E-1: Average Waiting Time for Clinic Patients (n=76, 3/10/2014-3/21/2014, Source: Patient Surveys)
Queuing Analysis The data analysis shows that the average patient spends 55% of their time waiting. Table E-2 shows more statistics on patient flow through the clinic from a queuing analysis.
Table E-2: Queuing Analysis Results (Source: Patient Surveys, MiChart 1/2/2014-1/23/2014, Little’s Law)
Conclusions Through the data collection and analysis the team has concluded the following: Confirmation of long wait times Significant communication breakdowns occur regularly Lack of standardization leads to delays in care Recommendations Based on the data collected and conclusions, the team has formulated three recommendations to improve workflow and reduce patient waiting times. Each recommendation is outlined below.
Recommendation 1: Standardize Patient Flow and Communication Expectations To reduce variation and increase communication throughout the clinic, the team recommends holding a continuous improvement event. The key staff members would be brought together to establish a standard flow, communication expectations for staff, roles and responsibilities for staff regarding flow, how to manage deviations from the standard flow, and how to maintain the changes in the long term. Standard operating procedures should be written to capture the decisions made during the event. The procedures should include how communication tools, such as whiteboards, will be used.
Recommendation 2: Implement Huddles The team recommends that the clinic staff implement huddles on a daily basis. These huddles would give staff a chance to discuss the day and any changes to the routine process that may occur. These huddles should consist of representatives from the Medical Assistants, physicians, echo sonographers, and technicians. Communication problems were found during shadowing, observing, and value stream mapping. The recommended huddles should reduce these problems.
Recommendation 3: Future Work – Echo Flow & Schedule Optimization Echo testing on average accounted for about 31% of a patient’s wait time in the clinic. In this project echo testing was considered out of scope since it also services inpatient units. The team recommends that a future IOE 481 project be devoted to this area due to the impact it would have on the clinic and hospital operations.
Expected Impact The team anticipates implementing these recommendations will provide the tools and methods to achieve desired patient wait times and satisfaction levels. In addition, reducing waiting times will allow for more capacity and increase revenue. Introduction The Michigan Congenital Heart Center (MCHC) is a referral clinic at the University of Michigan Health System (UMHS). MCHC treats patients from all ages with a congenital heart condition. The outpatient clinic offers many diagnostic services that are necessary for the care of their patients. Patients, who are on the inpatient side of Mott, Von Voigtlander Women’s, or University hospitals, may require services from this clinic. Leadership has expressed concerns over the workflow of the clinic because of the impact it may have on the patient, family, and staff satisfaction, as well as, visit volume and revenue. The clinic manager asked an IOE 481 team from the University of Michigan to identify ways to optimize workflow and efficiency to improve the patient experience and productivity through analysis and benchmarking. The purpose of this report is to provide the clinic with methodology of the clinic analysis, present findings, and deliver recommendations that the team believes will improve the workflow of the clinic.
Background The Michigan Congenital Heart Center (MCHC) serves patients who have a congenital heart condition. These patients include children and adults, as well as, hospital inpatients and scheduled outpatients. 70% of MCHC patients live more than 100 miles from the center. Because of the required travel, all required tests and treatments for an individual are scheduled to be completed in one visit when possible.
Containing all required diagnostics within MCHC helps to reduce patient confusion and expedite service. The center contains patient check-in with waiting room, exam rooms, consultation rooms, rooms for echocardiograms (echo), electrocardiograms (EKGs), exercise test lab, and x- ray. Doctors work in the team rooms to discuss test results and care plans. Some of these services, such as echo and EKG, serve hospital inpatients and other specialty areas on both a scheduled and emergency basis. Occasionally, MCHC staff must leave to serve hospital inpatients that cannot easily leave their beds. Outside demands make it difficult to schedule echos, which may last one hour, and EKGs. Some ambulatory patients have a minimal wait time between tests while others can wait several hours. The clinic manager hopes to see these inconsistencies and long wait times reduced.
There is not one standard path that each outpatient follows as care is customized based on the individual; however, the standard visit is as follows. The patient schedules an appointment in advance. Most required tests are ordered in advance. To aid in team communication, each day the medical assistants (MAs) and technicians (techs) create a schedule board with the patient’s name and physician’s orders. On the day of the appointment, the patient arrives at the center and checks-in at the MCHC desk. The receptionist ensures all required paperwork is filled out and alerts the MA’s of patient arrival. An MA then guides the patient from the waiting room to take height, weight, and other information. The patient then goes to each ordered test, waiting in the waiting room if necessary. After testing is completed and analyzed by physicians (attending and/or fellows), the patient has a consultation with their provider. If additional tests are needed that day, they will be ordered and performed at that point. After all care has been completed, patients proceed to checkout and leave the clinic. All testing is done within MCHC with the exception of lab draws, which are completed on the second floor of the hospital during the visit.
The clinic manager has expressed concern with the workflow of the clinic: some days go very smoothly and others do not. The manager speculates that the cause is lack of standardization in processes: each staff member performing tasks with their unique methods. It was also mentioned that the clinic lacks standardized communication. Some tools that are in place such as flags outside of exam room doors and instant messaging are used inconsistently. While each diagnostic service is within the center, testing/consultation rooms are separated by some distance or down different hallways, which impacts communication. One group of exam rooms is located past a fire door and far from the MA’s desks. The clinic manager has also stated that a reduction in patient wait times is desired with a long term goal of 30 minutes or less in total waiting time per visit.
Key Issues The following key issues are driving the need for this project: ● Lack of standardization in workflow processes. ● Lack of communication throughout the system. ● Extremely long patient wait times.
Goals and Objectives To develop recommendations to improve the current workflow and form solutions to create a standardized process, the student team has performed the following tasks: ● Conduct a series of observations and studies on each step of the process. ● Perform engineering analysis to optimize flow. ● Identify areas for improvement.
With this information, the team developed recommendations to: ● Improve the productivity of the staff. ● Minimize wait time and the total time for each patient. ● Standardize relevant processes that take place at the center. ● Improve patient and employee satisfaction.
Project Scope The scope includes the moment the patient arrives for an appointment until the patient checks out of the clinic. This process includes the following events: available appointment times, patient check-in, MAs exam, echo, EKG, exercise test, chest x-ray, reading of all tests, provider’s exam, and provider’s consultation with patients about results and treatments.
The project considers the impact of the volume of inpatients requiring services on the operations of MCHC, but will leave the inpatient workflow outside of the scope. The project will not include studies of any tasks or activities associated with the actual care taking of the patients once they have been admitted. The project also will not consider the process within echo testing, but will treat that step as a black box, analyzing the effects of echo on patient flow and the communication lines between echo and other departments.
Methods & Findings The team performed five types of data collection including: literature search, shadowing and observation, value stream mapping, surveys, and queuing analysis. The data collection methods have each led to important findings about the clinic operations.
Literature Search The team conducted a literature search in two parts. At the beginning of the project, each team member collected two articles for reference. Relevant concepts on data collection techniques and methods used on similar projects were shared during meetings with the team’s coordinators and client. This search helped introduce the team to industrial engineering in a hospital setting and assisted the team in the initial brainstorming phase. After data was collected, the team conducted another literature search to find tested solutions to the identified problems. Ten hours were devoted to this task.
The Institute for Healthcare Improvement had many different resources and articles on their website for improving efficiency and safety of a clinic [1]. These resources included data collection forms, how to use queuing theory, and the establishment of a volunteer who would help direct traffic flow. Other research showed the use optimization modeling to schedule patients in clinics. Specific to MCHC, research found that congenital heart care is a growing field [2].
Shadowing and Observation Shadowing and observation were done on all processes to gain an understanding of how the clinic operates. In total during this process the team spoke with three MAs, two receptionists, six attending physicians, four residents, one nurse practitioner, three sonographers, one sonographer scheduler, one EKG scheduler, three EKG technicians, one clinic manager, seven patients, and two volunteers. The team spent 40 hours observing to ensure that all position types were observed. Each team member shadowed five times for two hours a visit in pairs.
Through shadowing and observations the team was able to gain an understanding of the five key parties involved: patients, check-in/out clerks, doctors, MAs, sonographers, and techs. The team found that patients are a widely diverse group with many specific needs. Patients can vary in many ways such as: age, family situation, travel distance, condition, and disease progression. The check-in/out clerks are responsible for the schedules, collecting payment, getting the paperwork for the patient ready to start their visit, and scheduling follow-up care.
Doctors typically are with patients in the exam room or are in a team room. There are two types of doctors: attending physicians who are the responsible physician and fellows who are doctors in training. When in the team room, physicians are discussing cases, discussing test results, and determining plans of care. They decide to go to see patients based on information from the whiteboard or at their convenience.
MAs are responsible for taking patients from the waiting room to start their exams and testing for the visit. They appear to be juggling moving the patient between different areas of the clinic and keeping track of where they are between many different tests.
Sonographers who perform echos are located within the walls of the clinic and serve many MCHC patients but have many external stressors from inpatient and emergency demand. The other key player, techs who perform EKGs, seem to be able to accommodate the stochastic nature of the clinic.
Understanding the roles, responsibilities, barriers, and success of the clinic is crucial to finding solutions for improvement. The team determined that since the process has immense variation, simplification will be necessary to analyze the problem.
Value Stream Mapping Based on results from shadowing and observation, the team created a value stream map (Appendix B) to analyze the current workflow of the clinic. MAs, physicians, residents, sonographers, receptionists, the clinic manager, and project coordinators reviewed this value stream map. The team completed the following: interviewed key members of the team, identified areas of improvement, identified interdependencies in the system, identified staff responsible for each step, identified pre-requisite information for each key step of the system, and collected times for each step. There are many deviations from patient-to-patient, inconsistencies in process time, and preference differences between doctors. To counter these obstacles, the team mapped a general clinic flow, typical to that of an average visit.
Through value stream mapping, the team identified the general clinic flow to simplify the process and account for variation. Through the process of getting staff input, the team furthered their understanding of the delays that may occur in the clinic.
The general clinic flow is as follows: ● Patient arrives at the front desk, checks in with receptionist, and waits in the waiting room. ● MAs take the patient to one of three stations to measure height, weight, and gather information that will be used later on during the visit. ● The patient then goes back to the waiting room to wait for echo or is placed in an exam room. ● If needed, the patient has diagnostic testing done, such as echo, EKG, and/or pacemaker testing. ● One of the clinic fellows then does the first exam with the patient. ● After the fellow has done the first exam and discussed it with their attending physician, the attending will see the patient.
Many opportunities for improvement exist, such as: ● Reducing long waiting times. ● Staff members knowing where patient is at all times and alerting next person patient is ready. ● Reducing the many different pathways for patients based on diagnosis and differences in physician practices. ● Increasing communication between staff members. ● Reducing delays because of scheduling issues with echo. ● Using same whiteboard practices in each team room and amongst all staff.
A pattern of need for communication and standardization is very apparent from the value stream mapping.
Surveys The team created and distributed a patient-survey to collect feedback from patients and quantify the process times and waiting times. The survey is attached in Appendix A. The survey was distributed March 10 through March 21 and 76 surveys were completed. The clinic manager alerted staff of the survey.
From the 76 surveys collected, patients reported average total waiting time of 71 minutes. A breakdown of where these waits occur is shown in Table 1.
Table 1: Average Waiting Time for Clinic Patients (n=76, 3/10/2014-3/21/2014, Source: Patient Surveys)
Chart 1 shows that about 79% of patients are satisfied with their care at the clinic. The clinic manager has determined that a score of 4 or 5 will be considered satisfied while a score of 3 or less will be considered unsatisfied.
Chart 1: Patient Satisfaction Survey Results (n=76, 3/10/2014-3/21/2014, Source: Patient Surveys)
Chart 2 shows the largest barrier to arriving to their appointment on time is parking, among the various reasons for late arrival.
Chart 2: Barriers to On-Time Arrival for Patients (n=25, 3/10/2014-3/21/2014, Source: Patient Surveys)
Responses to other questions on the survey indicate that reducing waiting time will improve patient satisfaction. The results also shows that each member of “the staff was very pleasant, nice, [and] friendly.”
Queuing Analysis The clinic manager provided the team with data from the electronic medical record system, MiChart, on visit volume, check-in times, and checkout times for January 2, 2014 through January 23, 2014. The patient survey provided data on wait times. The team used Microsoft Excel® to obtain means and standard deviations for the data. By obtaining the arrival rate, average time in the system, and average time waiting, a queuing analysis using Little’s Laws was performed. This allowed the team to obtain other useful data.
The results of the data analysis and subsequent queuing analysis are provided in Table 2.
Table 2: Queuing Analysis Results (Source: Patient Surveys, MiChart 1/2/2014-1/23/2014, Little’s Law)
The data shows that, on average, there are about 11 patients in the clinic. This seems reasonable since there are 12 patient exam rooms plus other testing and waiting areas.
Conclusions Through the qualitative and quantitative data collection and analysis, the team identified three main conclusions: confirmation of long wait times, significant communication breakdowns occur regularly, and lack of standardization leads to delays in care. Confirmation of Long Wait Times Data from surveys now confirm the speculation that patients are experiencing long wait times. The survey showed that although they are satisfied with their care, patients are still complaining about delays. The clinic manager has mentioned different stories of how the waiting causes unnecessary anxiety for patients and families who are juggling many responsibilities. For instance, a mother who has to take one of her children to MCHC but has to be back on time to pick up her other children from the bus stop.
Significant Communication Breakdowns Occur Regularly The team noticed that the lack of standard work and communication practices results in staff working to accomplish their own tasks and suboptimal coordination of care with other key parties. The communication breakdowns and lack of communication are the cause of many delays because the next person responsible for care is unaware the patient is ready, patient location was not communicated, or changes in plan of care are not disseminated.
Much of the communication between the key players in the clinic is done non-verbally through whiteboards in the team rooms. This raises two big issues: over reliance on whiteboards that are not standardized and lack of talking between staff about the flow of the patient.
Lack of Standardization Leads to Delays in Care Two sources of variation are physicians’ different preferences in the flow of their patients and patients many different needs. The two sources of variation in addition to the lack of standardization in clinic processes and procedures, create delays. Although it is not possible to make the patients less complex, it is possible to standardize the processes and to account for the variation so long wait times do not occur.
Whiteboards in the team rooms of the clinic are another source of delays due to lack of standardization. Each whiteboard, although containing the same basic information, is different. There is no standardization to who writes on the board and when. For instance, there is not a standard for when to cross a patients name off the list or if it is expected that sonographers write on the board to indicate testing.
One example of where standardization would be helpful is when people decide to alter the process to expedite care. For instance, a physician who has a free moment decides to go see a patient but the EKG tech has just shown up to do a test. Now there is a delay for the patient who has to wait for the tech to come back. There is no standard process for when to see the patient additionally, there was not standard to communicate that change. In this case, the patient was not out of the clinic any earlier. Recommendations The team developed three recommendations to address the needs of the clinic and accomplish the goals. The recommendations, based on the data, findings, and conclusions, are: standardize patient flow and communication expectations, implement huddles, and future projects.
Recommendation 1: Standardize Patient Flow and Communication Expectations In order to address the variation and delays in the clinic there needs to be a standardization of the expected patient flow. Since the clinic has many staff involved in the care of one patient during the visit, communication expectations need to be established. In order to accomplish the standard flow, the team recommends holding a continuous improvement event (CIE). The recommendation is rooted in adopting the Lean culture spreading throughout C.S. Mott Children’s Hospital. The Lean philosophy is that the people doing the work everyday are the best people to make the changes. The CIE is a tool to help facilitate standardization and expectation setting. Note that CIEs are also known as Kaizen events in traditional Lean literature.
At the CIE, members from each of the key staff areas should attend: MAs, doctors, echo, and EKG. The clinic manager should serve as the facilitator. The clinic team working together in the CIE should improve team cohesion.
The event has 3 key deliverables including: standard operating procedures (SOPs), implementation plan, and progress/ audit plan. The first of three SOPs that need to be written is the “Standard Patient Flow.” This SOP will establish the standard patient flow through the different areas of the clinic. By designing a single flow, variation will be reduced and the entire clinic staff will know what to expect. The next SOP will address staff members’ roles and responsibilities regarding patient flow. Each staff member should have a clear understanding of what his or her role and responsibility is to maintaining patient flow in the clinic. For instance, the MAs may act as traffic controllers who are ultimately responsible for getting the patient out in a timely manner. This SOP is not intended to address medical care or scope of care (i.e. how take blood pressure). The third SOP discusses plan of care changes for patients during the visit. Plan of care changes may be ordering more tests or changing orders. This SOP should set the standard for communicating the changes and executing the changes so that unnecessary additional delays are not created.
All the SOPs should clearly define what tools and technology will be involved and how it will be utilized. The tools and technology currently used are: MiChart, phones, whiteboards, and instant messaging. The team strongly encourages that whiteboards are discussed and standardized during the CIE. The findings suggest that the lack of standardization of whiteboards – in terms of design and use – causes many delays.
The implementation plan should have deadlines and assigned responsibilities so the CIE does not turn into a useless meeting without results. The audit system should use data to determine if the changes were successful. Using data provides a more objective way to help guide decisions as well as maintain a blame-free environment. The team has provided a value stream map, survey data, and a queuing analysis. Other data available includes MiChart check-in to checkout data and defect tracking. The defect tracking will also serve to audit the changes and see how successful they are. This data can be reviewed at another CIE for long-term results. Some key metrics to start out with are as follows: Total time in clinic (Manager’s goal: 80% check out in 90 minutes or less) Total waiting time (Manager’s goal: 30 minutes or less)
Patient satisfaction Staff satisfaction
Recommendation 2: Implement Huddles Changes to schedules and flow will are likely to occur because of the stochastic nature of the clinic (patients arrive late, changes to plans of care, etc.). Additionally, with the implementation of data based standardization, it is important to reflect on the previous day’s performance in order to improve in the future. The team recommends implementing two types of huddles: Morning Huddles and Time-Out Huddles. The Institute for Healthcare Improvement recommends huddles to help anticipate needs [3].
The morning huddles will review the key metrics and defects from the day before. The defects could be tracked on a whiteboard in a central area. During this time, staff can also brainstorm ideas for improvement. Morning huddles should also address any obstacles or changes to operations for the day.
The time-out huddles are to be conducted every two hours starting two hours after the morning huddle. Representatives from MAs, echo, EKG, and physicians need to attend to discuss the patients in the clinic and patients who are supposed to be arriving. During this huddle, the clinic team can discuss the patients who are in the clinic and who are scheduled to arrive. The staff can coordinate or confirm any additional testing needs, changes to care plans, or how to deal with an early or late patient arrival.
Recommendation 3: Future Work – Echo Flow & Schedule Optimization During the team’s time in the clinic, echo was a major source of contention because of the perceived delays that this testing caused. The team found that 31% of total wait time was from echo waiting. The issue is that echo has many different customers who need its limited resources throughout the hospital. The team recommends that another project be devoted to first improve the workflow of echo and then to optimize the scheduling and resources. Much research on optimization modeling of schedules exists in literature. This will also affect the clinic flow by further reducing the total time the patient is in the clinic.
Expected Impact Through the recommendations stated above, the team believes that through the tools and methods provided, desired patient wait times and satisfaction levels can be achieved. Along with lowering wait times and increasing satisfaction levels of the patients, the recommendations will also help the clinic from a financial perspective. Reducing wait times, leads to fewer patients that are in the clinic system. This permits for greater capacity, allowing the clinic to see more patients, increasing revenue.
References
[1] Institute for Healthcare Improvement, Resources, Institute for Healthcare Improvement. [Online]. Available: http://www.ihi.org/resources/Pages/default.aspx. [Accessed: 30 January, 2014].
[2] M. A. Gatzoulis, S. Hechter, S. C. Siu, and G. D. Webb, “Outpatient clinics for adults with congenital heart disease: increasing workload and evolving patterns of referral,” Heart, vol. 81, no. 1, pp. 57-61, January 1999.
[3] Institute for Healthcare Improvement, Huddles, Institute for Healthcare Improvement. [Online]. Available: http://www.ihi.org/resources/Pages/Tools/Huddles.aspx. [Accessed: 3 April, 2014]. Appendices
Appendix A: Patient Data Collection Survey
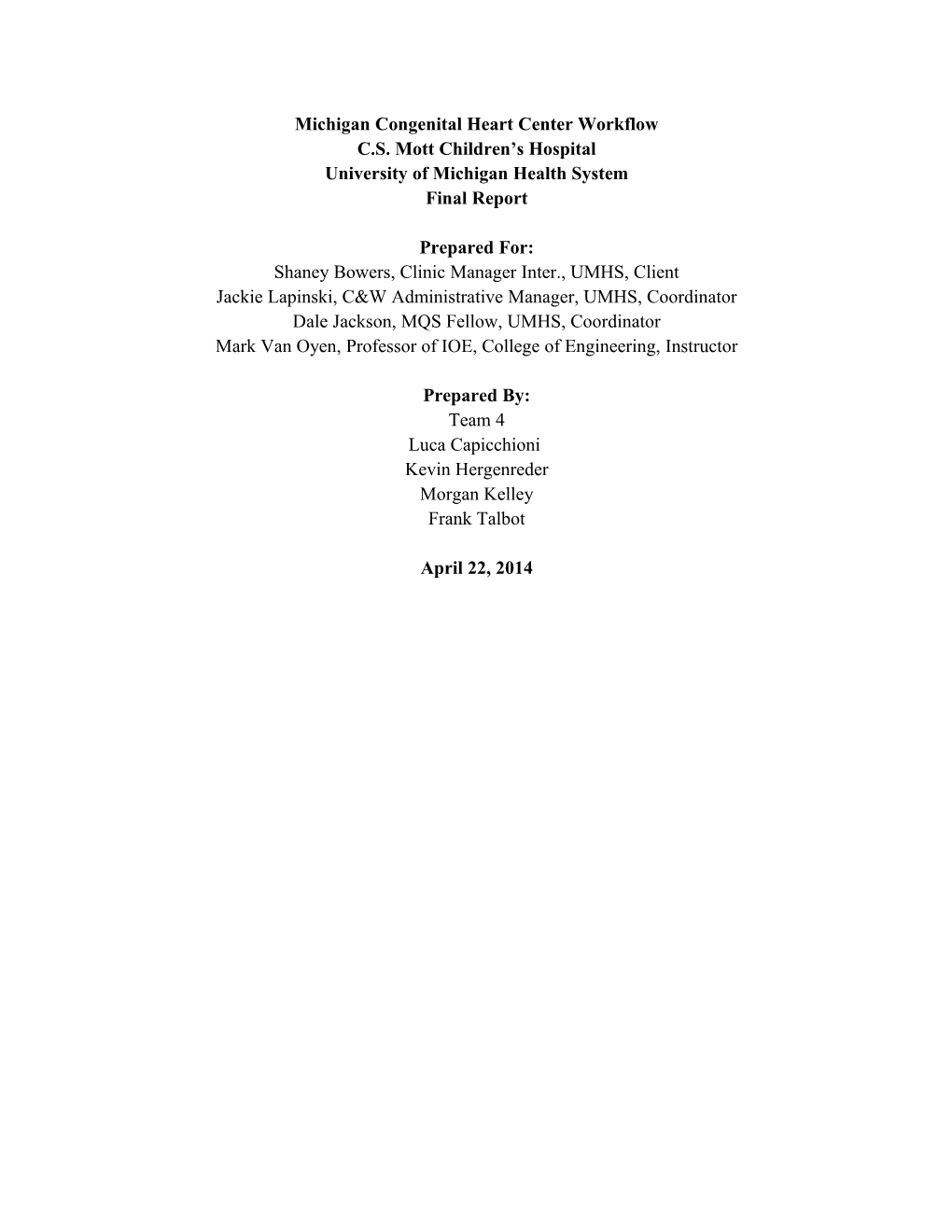
Appendix B: Value Stream Map
C l i n i c W o r k f l o w Schedule Visit Not notified when pt is Pt not waiting Patient registered th Arrives on 11 MA not Walk in EKGs Delay with Floor Chart aware of pt cause slow reading not arrival down tests closed F e l l o w , N u r s e P a t i e n t H e i g h t a n d P a t i e n t C h e c k - i n P r a c t i c i o n e r o r A t t e n d i n g E x a m P a t i e n t C h e c k o u t W e i g h t a r e t a k e n E c h o E K G Receptionist R e s i d e n t E x a m Attending Receptionist/ MA Sonographer Technician Check in Fellow, NP, Doctor Clerk Exam/ Echo room Exam Room desk Resident Exam Room Checkout Consultation Paper/ Paper/. Paper and Exam Room Paper/ Desk Room Electronic Electronic Electronic Paper/ Electronic Paper/ Electronic Info 22 Minutes 8 Minutes Info Electronic 15 Minutes Electronic 10 Minutes 16 Minutes
-Pt is late No -Appt. cancelled disposition and pt is not notified
-Not notified when pt More tests are is ready ordered -Pt is late No communication -Not aware fellow needs teaching -Communication Issues KEY T y p e o f A c t i o n P e r f o r m e d -MiChart Info Wrong Staff conducted procedure -Sonographers busy Location w/ IPD Type of Information Problem Transferred Points Wait Time before Procedure