FUN2: 10:00-11:00 Scribe: Joan-Marie Manolakis Monday, October 20, 2008 Proof: Andrew Richardson Dr. Barnum Immunology Introduction Page 1 of 7 Specific Description of the Topic Being Discussed Today I. Introduction : a. [email protected] phone: 4-4972. b. [S1] If you haven’t bought the textbook and you’ve never had immunology in the past, I suggest you buy it because it’ll be a good resource that’ll be useful for a lot of classes. If you have a book from a previous course, then it should be fine. c. Immunology is important for a lot of reasons for your future as a clinician. You need to know at least some of the major players, how it works in order to treat these individuals, and also to safeguard yourself and the people that work for you d. [S2] Most people will come see you because they are having problems with their immune system. Either it’s failed to cope with an infection or trauma that’s occurred, like the little kid that gets his tooth knocked out, his eye poked out or has an infection, gum infections, etc. e. Cavities are basically a bacterial infection in the tooth, so all those components, or all the reasons you see that individual, is because of an immune response. For example, inflammation, trauma, and potential infection of the immune system can’t handle that. You need to understand some of the mechanisms of what is going on in those given settings so that you can treat them. f. When someone says that he/she is immuno-compromised and you have to treat me accordingly, you don’t want to have to say that you don’t know what he/she is talking about. So, you need to be able to understand some of that. g. The immunological status of your patient determines how you treat your patient. For example, if the patient is on chemotherapy and their immune system is wiped out, then they are extremely susceptible to infection. You have to figure out how to treat an individual and that given setting so that you don’t infect them and cause problems. h. You’ll also have patients that have allergies. If you forget to ask and you prescribe penicillin for an infection, they will go and fill it not knowing. Then you get a call and the patient’s in the ER with a massive allergic reaction to penicillin. i. Thus, you must understand the underlying mechanism behind these events in order to treat patients properly. j. You also need to protect yourself and staff because people will come into the office sick. Again, you need to be able to protect yourself and staff so that your office doesn’t become a fantastic place for your patients to get sick. k. You don’t want to be known as Dr. Infection as you try to start your practice. II. Immune System Components [S3] a. There are a handful of you that haven’t ever had immunology before, so I’ll give you a basic idea. b. It’s an old term from the latin word immunitas, meaning exempt. It originally applied to politicians so that they’d be exempt from being tried. That definition still holds. c. Over time, it came to mean individuals that were exempt from being sick. In old times an infection used to wipe out entire towns, and there’d always be someone who didn’t get sick. So, they were considered immune from that infection. Some of them gained great status because they had special powers. d. Immunology is basically the study of the cellular and molecular events that occur in response to invading pathogens. e. Does it always target invading pathogens? No. Sometimes it targets your own tissues, and then you have autoimmunity. f. Individuals who have autoimmune disease know the full power of the immune system, and it can be extremely destructive because they’ll lose their pancreas, kidney, thyroid, etc., because it will wipe them out when improperly directed. g. Autoimmune diseases are a major focus of study when dealing with immunology. h. You’ll have a lot of lectures on the components of the immune system. FUN2: 10:00-11:00 Scribe: Joan-Marie Manolakis Monday, October 20, 2008 Proof: Andrew Richardson Dr. Barnum Immunology Introduction Page 2 of 7 i. It can be broken down into a number of different parts: cells and organs. One of the primary organs that you’ll learn about in another lecture is the thymus. It’s a small organ that sits near the throat; it’s the source of T cells and is involved in immune response. j. The spleen is major for filtering immune complexes and sits right next to the liver. k. Lymphnodes are scattered throughout and gather antigens (invading bacteria/viruses) wherever they’ve entered the host and get them in contact with the right type of cell (T cells, B cells, and antigen presenting cells). Then you can mount a very specific immune response to that invading pathogen. You’ll hear much more about them. l. All of the cells involved in immune response come from pleurypotent stem cells that are self renewing. If you end up with cancer and they have to wipe out all of your immune system, they can take out stem cells, wipe out the immune system and then basically give you a new immune system by putting the stem cells back in. They’ll divide and turn into all the different types of cells. Then you’ll hopefully have a fully functional immune system. m. There are a number of different progenitor cells that give rise to all the different cell types. n. T and B cells are involved in adaptive immunity. They’re critical for specific immune response. o. Macrophages and neutrophils are part of the innate immune response. Their job is to eat and kill whatever doesn’t belong there. So, they gobble up bacteria, viruses, and whatever else they encounter. p. Dendritic cells are found in lymphnodes, the spleen and other tissues in the body that are involved in antigen-presentation (APC’s)You’ll have some lectures that cover this topic. There are APC’s. q. Dendritic cells (DC’s) are important antigen presenting cells. Macrophages can also serve as antigen presenting cells, and B cells (though they’re the source of antibodies in immune response) also serve as antigen producing cells. Other cells can be when they’re induced, but these are the important ones. r. Mast cells are important in hypersensitivity types of reactions. It’s the mast cells that give those of you with allergies a fit. s. There are a few other types that you’ll hear about as you go along, but these are some of the most important players. t. The other system that I didn’t put up there is the bone marrow. u. T cells come from the thymus, and B cells come from the bone marrow, but lots of other cells types come from bone marrow (macrophages, dendritic cells, neutrophils, etc.) v. It’s a major source of cells involved in immune responses. w. Humoral/Soluble components: The most predominate known is antibody. There are many types or isotypes of antibody. You’ll have a lecture on their generation. x. Cytokines are one of the most important components. The number of them is about 100 or so, including chemokynes. y. These are small molecules that are critical for sending signals for development of different lymphoid lineages, all the different leukocyte lineages, cells involved in activation of T cells and B cells, and other types that participate in immune responses. They all get their signals from cytokines. z. The complement system is part of the innate immune response. It is critical for killing invading pathogens and actually punching holes in them by a protein complex called a MAC. aa.They target invading pathogens by covalently attaching proteins to the surface of that pathogen so that they can be taken up by macrophils or nuetrophils. It also produces small molecules that are important in inflammation, and a number of the acute phase proteins also do this. They basically rev up the body to eliminate invading pathogens by making more cytokines by changing the number of cells that are produced, like macrophages and neutrophils, to get their numbers to go up. All of this is done to help eliminate invading pathogens and turn on the immune response. bb.There are lots of different enzymes, and some are found free floating in serum or at sites of tissues, and others are inside the cells (like macrophages and nuetrophils) that have these vesicles inside so once they’ve engulfed the bacterium, for example, they have every class of enzyme to chew up proteins, lipids, DNA, etc. to almost nothing. FUN2: 10:00-11:00 Scribe: Joan-Marie Manolakis Monday, October 20, 2008 Proof: Andrew Richardson Dr. Barnum Immunology Introduction Page 3 of 7 cc. The body produces its own antibiotics, defensins (produced by a number of cells in the body), and some are bacteria static and prevent it from growing. You won’t hear too much about those, but they come into play in a variety of settings and cell types. dd.That’s an overview of the major components of the system. ee.I mentioned this term innate and adaptive immunity. ff. The immune system has been broadly classified into innate and adaptive immunity. There have been discussions about relative importance of one part of the immune system when you classify them this way. gg.Both of these parts of the immune system are interrelated, and you can’t have a great immune response without both of them. hh.If you’re missing components that are part of the innate immune system, like the complement system, you’re going to have serious immuno-deficiency. If you’re missing T cells or B cells you might still have a fully intact innate immune system, but you’ll be seriously immuno-compromised. ii. Both of these arms are necessary in mounting good efficient immune responses to eliminate invading pathogens. They work together to do so. jj. The innate immune system is responsible for early elimination of pathogens. It’s also important in antigen presentation so that pathogens can be presented to T cells to mount a good response. So, this response is a little later in eliminating pathogens. kk. We’ll talk about that a little later. III. Innate vs. Adaptive Immunity [S4] a. Are you using adaptive interchangeably for acquired? Yes. b. This slide breaks down the components of the innate and adaptive immune responses. c. If you get a cut, the innate immune system will be at work immediately because once it’s cut, you’ve torn open vessels and activated cells in the immediate side of the cut like mast cells. Mast cells will be activated and cytokines will be activated. Immediately the innate immune system will try to eliminate that pathogen. If it can do so efficiently because there’s not a lot of bacteria, you might not need the adaptive immune response engaged under those circumstances, but that doesn’t always happen. d. The adaptive immune response takes days because it’s extremely specific. The innate immune response will go after whatever it finds and it doesn’t care what it’s going after. The adaptive is very specific in what it targets. You have to get whatever invaded you in contact with the specific B or T cell immediately. e. If you have cut on your wrist, for example, and the T cell that was specific for that invading pathogen is in the lymphnode in the back of your left leg, it’ll take time for the two hook up. You don’t have a million T cells specific for everything you come in contact with. You might have hundred. It takes time to get the two together to mount a specific immune response. It takes longer to do that. f. The innate immune response is specific for molecular patterns, aka PAMPS (Pathogen Associated Molecular Patterns). g. These are things like lipopolysaccharides, cell wall materials, peptidoglycans, single and double stranded RNA, etc. h. It allows the innate immune system with a few receptors to recognize millions of different pathogens based on these common structures in bacteria, yeast and other pathogens that might invade. i. The adaptive immune response is extremely specific. The adaptive immune response can discriminate between molecules that are very subtly different. Just the shift of an amino group can yield antibodies that recognize one structure and not the other. It is extremely specific in what it recognizes. j. In the innate immune response there isn’t much diversity. The diversity lies in the receptors that recognize these PAMPS. There’s not a lot of these receptors, maybe 20 or 30, that will allow you to recognize lots of bacteria and viruses. k. The adaptive immune response you have a highly diverse repertoire. At any given moment your body is churning out millions of T cells and B cells, all of which have a single specificity for a single FUN2: 10:00-11:00 Scribe: Joan-Marie Manolakis Monday, October 20, 2008 Proof: Andrew Richardson Dr. Barnum Immunology Introduction Page 4 of 7 invading pathogen. You have a massive diversity that’ll allow you to recognize anywhere up to 10^8 or 10^9 different microorganisms. The adaptive immune response has clones for everyone. It allows you to eliminate them very efficiently. l. Innate immune responses have no memory so the next time you encounter the same thing it’ll respond with the same vigor as the first time around because there isn’t any memory component or cells there. m. Adaptive immune response has persistent memory. If you develop a good antibody response to an invading pathogen, you make a lot of B cells that will produce that antibody and they’ll go hide in the bone marrow and continue to chunk out antibodies for years after that. You’ll have memory B and T cells. There will be great numbers of them compared to before you encountered the pathogen, so the next time you encounter it’s much faster response than before (a few days instead of a week or two). n. This is a point that sometimes gets a little tricky: self vs. nonself immune responses o. The innate immune system is geared to recognize PAMPS, but it can be misdirected and attack your own tissues. For example, in the cases of autoimmune diseases where you have antibodies to your own tissues, antibodies can bind to the cells in those tissues, and if they’re the right isotype they can activate the complement system. The complement doesn’t know it’s your own tissue, it’s just been activated and it can destroy your own tissue. p. Or if you have a really big infection, the innate immune system will do its best to eliminate the infection, but in the course it’ll destroy some of your own tissue. It elaborates lots of enzymes and cells that can cause damage to your own tissues. q. It doesn’t recognize you, but it can damage you. It’s perfect in that it’s not geared to ever recognize you, but it can certainly cause damage. r. The adaptive immune response does a good job of discriminating self from nonself. s. Everybody in this room has a few T cells and B cells with specificity towards their own systems. The immune system has mechanisms to clamp those down they never get a chance to take off. That’s the price you pay for this repertoire that allows you to recognize a lot of invading pathogens. t. Many of the innate immune system components are found in blood, like complement proteins or defensin molecules. u. The major player of the soluble part of the adaptive immune system is antibodies. Almost every tissue and fluid has antibodies. There are antibodies in tears, saliva, etc. If you squeeze your arm, you’ll find them there. They’re everywhere to protect you at all times. v. The major cell types: phagocytic cells like monocytes, macrophages, neutrophils, natural killer cells, etc. w. The major players in the adaptive immune response: T cells, B cells, and antigen presenting cells. x. Question: Can you distinguish between specificity and diversity? y. Question: INAUDIBLE AND LENGTHY z. Innate doesn’t produce autoimmune diseases; it becomes activated by being misdirected. aa.If this is the thymus and you have an autoimmune disease where you make antibodies to your own thymic tissue, and if they’re the right isotype, they can activate the complement system. bb.When the complement system is activated, it can punch holes in cells and lyse them. In that setting, the innate immune system is damaging your tissues, but it wasn’t doing it on its own volition because there’s complement proteins like antibodies in your blood and tissues. It had to be activated and directed to do that. cc. If you have a massive infection, you’ll recruit all kinds of cells to eliminate that infection. In the process, they’ll release enzymes and molecules that can kill the invading pathogen but can damage the tissue at the same time. dd.The innate immune system is often associated with damage to your own tissues, but it’s not because it’s an autoimmune response rather it doesn’t discriminate your tissue from the pathogen in trying to eliminate it. FUN2: 10:00-11:00 Scribe: Joan-Marie Manolakis Monday, October 20, 2008 Proof: Andrew Richardson Dr. Barnum Immunology Introduction Page 5 of 7 ee.In terms of specificity and diversity, you can say the adaptive immune response has a large repertoire of T and B cells. Each T and B cell has its own antigen receptor on its surface. Each one has a different antigen receptor than the one next to it. That gives you about 10^9 different B cells and different T cells. Each one is specific for a different pathogen. ff. The innate immune system is associated with damage of the tissue. gg. Basically there’s almost nothing that the adaptive immune system can’t recognize. You’ll see how it is possible to make T cells and B cells specific for your own tissues. IV. Innate Immune Mechanisms of Protecting the Host [S6] a. Most textbooks go from a cut in the arm and present the systemic response, but really 99.9 % of the infections are things you inhale or eat. b. Your skin is very important in protecting you from pathogens. Some of the most important facets of how this system works were developed at UAB. c. (Mucosal Immune System) One of the major players in protecting you from invading pathogens is the skin. If someone gets a large burn over their body, they normally die of infection. That’s a major barrier. d. The skin also has a lower pH, which isn’t going to favor all microorganisms. There are also some defensins found in skin. We also have oils that may be bacteria static or soluble. So aside from a physical component, you also have some components that are responsible for at least keeping things in check if not killing them. e. In terms of mucosal surfaces (lungs, gut), one of the major components that serves sort of as a skin, is mucous. Invading pathogens encounter mucous in the mucosal tissues, and some won’t be able to get into the surrounding tissues. f. Some of the material will be swallowed down to the stomach. With all the different digestive enzymes in the stomach, they might be eliminated in that fashion. g. You also have in your tears and saliva enzymes, for example, lysozyme. It is responsible for chewing up cell wall material in some types of bacteria. There are all different components so that as soon the invading pathogens hit these tissues sites, they’re in trouble already. They can’t attach to tissues to cause infection. There are enzymes like defensins, and they are doing their best in protecting from infection. There might also be some complement proteins there. h. Anything that makes it from the mouth to the stomach… with a pH of 2, warm temperature, lots of different enzymes. It goes to the small intestine where it undergoes pH reversal and encounters many digestive enzymes and defensin molecules. It then goes to the large intestine which has more bacteria. i. You have more bacteria in your gut than you have cells in your body. Their job is to stay there and do important things. You’ll have problems without them. There are invading pathogens that will try to set up shop. Since the gut is already loaded with bacteria, they’ll have a hard time competing and they’re not going to be able to stay there. j. In the lungs and airways you have cilia that will sweep things out. You cough and sneeze to get things out. There are also macrophages resident in the lung. Any time something comes in and sits on the mucosal tissues in the lung, the macrophages can be stimulated and start an immune response. k. In some of these tissues you don’t want a massive immune response because it’ll be bad for survival of the host. l. For example, the lungs or the eyes, you don’t want a large immune response. m. The eye is another example and is in somewhat immuno-suppressed to prevent that kind of immune response from occurring.
V. Innate Immune System [S7] a. I’ve already kind of alluded to this already. b. They do so via Pathogen Associated Molecular Patterns (PAMPS) c. They are found on invading pathogens, like lipoproteins, peptidoglycan, RNA species, etc. FUN2: 10:00-11:00 Scribe: Joan-Marie Manolakis Monday, October 20, 2008 Proof: Andrew Richardson Dr. Barnum Immunology Introduction Page 6 of 7 d. These receptors that recognize them are called PRRs, Pattern Recognition Receptors. There is only a hand full of these so you only need a few of these receptors to recognize a large array of invading pathogens. Some of them are in a family of collectins. e. You may have heard that cyriactive (sp?) protein can recognize lot of pathogens. Toll-like receptors are really the most important. They have been recently described.
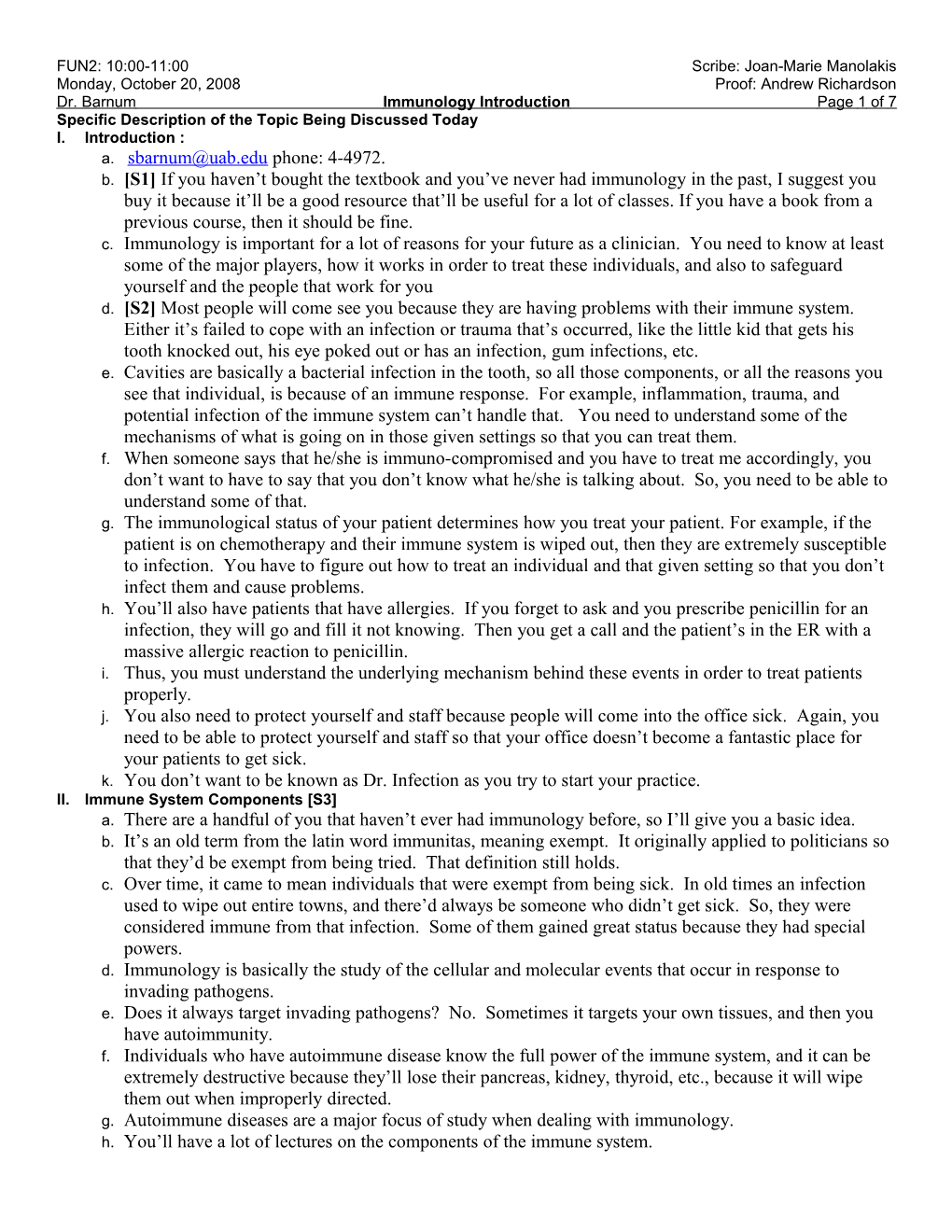
VI. Toll-like Receptors (TLRs) [S8] a. This is an example of what they look like. b. They are intramembranous molecules and have the characteristic hook structure. This shows nine of them, but there are maybe eleven. c. The different toll-like receptors recognize different bacterial or invading pathogen components. d. TLR 1 recognizes microbacteria. e. TLR2 recognizes gram positive bacteria (lots of different pathogens)…. It recognizes certain features. f. You also have toll-like receptors that live inside the cell because viruses like to live inside the cell. These are key receptors that are responsible for recognizing viral components and invading pathogens inside the cell. They recognize different components.
VII. Adaptive Immunity [S9] a. It may also be called Active immunity or Acquired Immunity. Acquired immunity refers to a setting where you’ve actually been infected with something and mounted a good immune response under the circumstances. b. Vaccination is an artificial mounting of an immune response. It is one of the major breakthroughs in modern medicine. c. It goes by all these different monitors. d. Passive immunity, for example, is a mother’s milk. The antibodies in the milk are protective. The isotype is IgA. e. Another mechanism of passive immunity involves giving you a gamma-globulin (Ig) injection. He uses the example of going to eat at a greasy restaurant, and then there’s a breakout of hepatitis. To be sure you’re okay they give you the injection. Basically, they give you a major injection of antibodies from people they’d pooled who have hepatitis, so they will protect you from developing the disease. f. Antivenom used to be the way to be the way to protect people. They would inject horses and then they’d give you the injection from the horse. If you get bit twice from a snake and received antivenom after the first bite, then you don’t need antivenom again because by that time you should have developed an antibody for it. If you haven’t yet developed one you’ll probably get immune complex disease where these antibody complexes sit in your joints and you’ll feel awful. g. You can also have passive transfer through the placenta before birth, and that’s IgG. When a baby is born it already has its mom’s IgG to protect it. If it drinks breast milk it’ll also have specificity to protect it for what all those antibodies are. After time, that’ll turn over and the baby’s immune system will start to develop. It takes some time for adaptive immunity to take over and fully develop. h. When we say humoral immunity we’re basically talking about B cells and antibody. These are cells that are found in lymphnodes and the spleen, circulating in blood, and bone marrow. Once they’ve been activated, they actually are called plasma cells. At that point they are just a factory for producing antibodies. They chunk out 1000 antibodies/minute when they’re fully activated. i. Then there’s something called cell-mediated immunity. Generally that refers to T cell mediated immunity. You’ll learn about two types through the course, and you should learn about CD4+ and CD8+. j. CD4- they are the master regulators of the adaptive immune response and their job is to produce cytokines that regulate the other players that will eliminate the invading pathogen. Their job is to produce cytokines. FUN2: 10:00-11:00 Scribe: Joan-Marie Manolakis Monday, October 20, 2008 Proof: Andrew Richardson Dr. Barnum Immunology Introduction Page 7 of 7 k. CD8-can also produce cytokines, but if they get the right kind interacting with receptors on the surface of the CD8+ T cell, they can become what’s known as CTL, cytotoxic lymphocyte (important in viral infection). They recognize virally infected cells and kill them, which prevents the production of more viral particles. l. CD4+ T cells can be subdivided into Th1 and Th2, and the subdivision is based on their cytokine production. m. Th1-produce cytokines like gamma interferon (IFN). They are very important in cell-mediated immune responses like CTLs. The IFN, when it interacts with a CD8, interferon serves as a powerful push to activate that cell to differentiate into a cytotoxic lymphocyte. n. Th2 typeproduce cytokines like IL-4 or IL-5, which are important in antibody-mediated immunity. They’ll interact with B cells and stimulate the production of antibody. o. [S10] They all have surface receptors that recognize antigen. p. A B cell expresses on its surface membrane-bound B cells. q. On any one given B cell, all the antibodies on the surface recognize the same thing, the one specific thing (T cells too). r. Because you have millions of B cells, there are millions of specificities. s. It’s the same on T cells. You’ll hear of the T cell receptor on T helper cells or CD4+ cells and CTL- type cells. They have on their surface either CD 4 or 8 molecules, and that’s how we distinguish the two types for given purposes.
VIII. Cardinal Features [S11] a. Specificity-you can have molecules that are extremely similar and differ only in the position of the side chain. b. The adaptive immune response is extremely specific. Just the subtle change of a few molecules and it won’t recognize that anymore. c. Diversity- you have lots of different T cells and B cells that recognize a lot of invading pathogens. I’ve already mentioned that you can recognize up to 10^9 different pathogens. At the genomic level you don’t have 10^9 different genomic antibody genes. d. If you did, say an antibody gene is 2000 bp’s( x) 10^9 Ab you’d need 2 x 10^12 bp’s just for antibody genes. That’s a problem. The human genome only has 3.8 x 10^9 base pairs. How can you generate this diversity of antibodies and T cell receptors? The immune system does gene rearrangement. During the development of T cells and B cells, they break their DNA and rearrange segments of it to produce antibodies and T cells with different specificities. There’s risk that the DNA won’t go back as you want it or it’ll become an oncogene. e. Memory-you have long term memory with the adaptive immune response. Sometimes the memory can last decades from invading pathogens. f. Self-limiting response- it is very powerful in eliminating pathogens, so you need a way to turn it off because you don’t want to continue making macrophages and T cells in response to the new pathogens. You have shut the response down. One way to do that is to eliminate the pathogens. With the pathogen gone, the immune system goes back down. g. Once an immune system is initiated, you start to make cytokines that are anti-inflammatory cytokines that’ll interact with T cells and B cells and macrophages to help turn them off. There’s a self-limiting response to help shut it down. h. Most of the mechanisms are short-lived. It’s on the order of minutes to hours that they’re produced. i. If there’s still pathogen around then there will be another need for a burst of cytokines, but if not, then that’ll take system down. It’s very tightly regulated. j. Self vs. non-self- it’s exquisitely specific. We’ve talked about immunity, and some people have much more capacity to autoimmune responses.