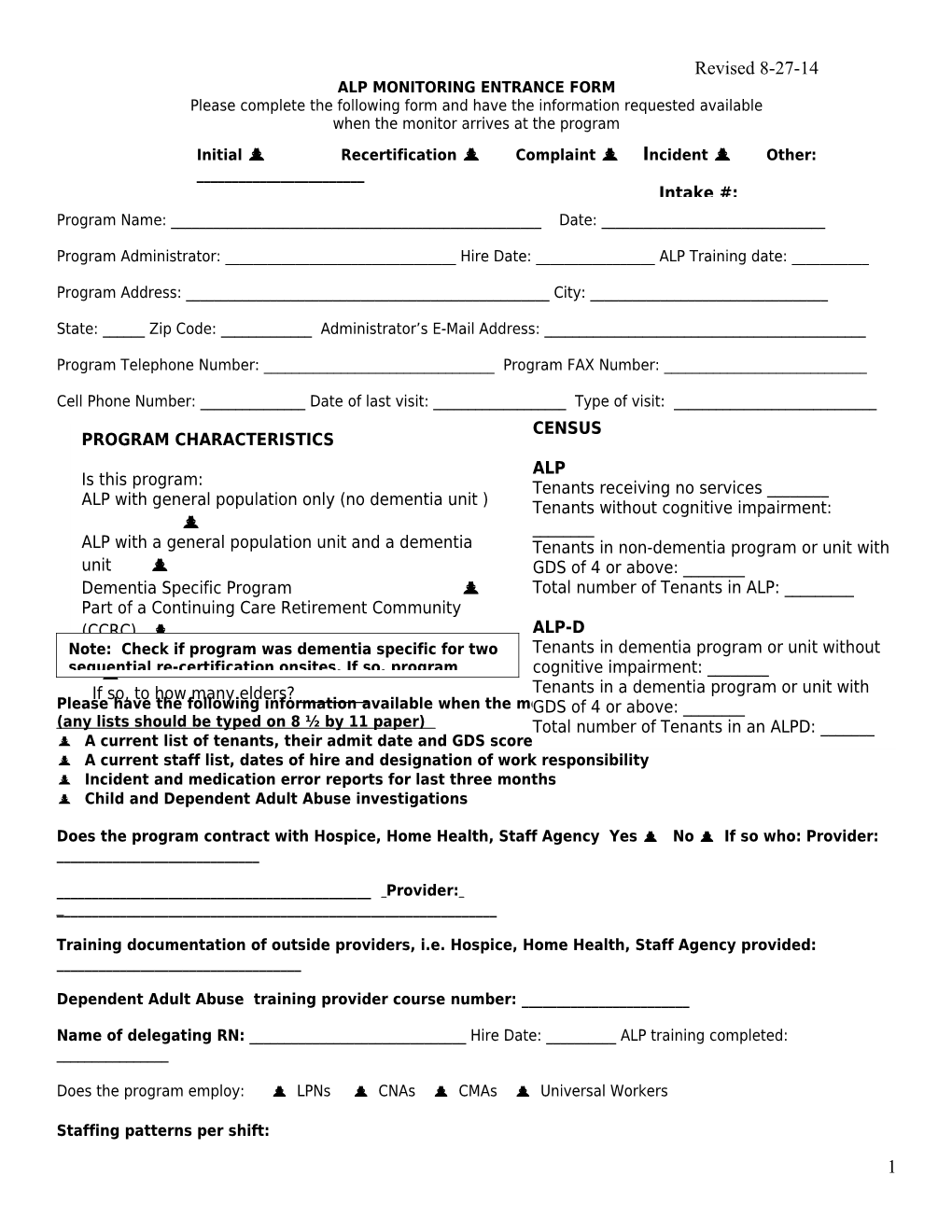
Revised 8-27-14 ALP MONITORING ENTRANCE FORM Please complete the following form and have the information requested available when the monitor arrives at the program Initial Recertification Complaint Incident Other: ______Intake #: Program Name: ______Date: ______
Program Administrator: ______Hire Date: ______ALP Training date: ______
Program Address: ______City: ______
State: ______Zip Code: ______Administrator’s E-Mail Address: ______
Program Telephone Number: ______Program FAX Number: ______
Cell Phone Number: ______Date of last visit: ______Type of visit: ______CENSUS PROGRAM CHARACTERISTICS ALP Is this program: Tenants receiving no services ______ALP with general population only (no dementia unit ) Tenants without cognitive impairment: ______ALP with a general population unit and a dementia Tenants in non-dementia program or unit with unit GDS of 4 or above: ______Dementia Specific Program Total number of Tenants in ALP: ______Part of a Continuing Care Retirement Community (CCRC) ALP-D Note:Respite Check provider if program was dementia specific for two Tenants in dementia program or unit without sequential re-certification onsites. If so, program cognitive impairment: ______If so, to how many elders? ______Tenants in a dementia program or unit with Please have the following information available when the monitorGDS of arrives: 4 or above: ______(any lists should be typed on 8 ½ by 11 paper) Total number of Tenants in an ALPD: ______ A current list of tenants, their admit date and GDS score if above four A current staff list, dates of hire and designation of work responsibility Incident and medication error reports for last three months Child and Dependent Adult Abuse investigations
Does the program contract with Hospice, Home Health, Staff Agency Yes No If so who: Provider: ______
______Provider: ______
Training documentation of outside providers, i.e. Hospice, Home Health, Staff Agency provided: ______
Dependent Adult Abuse training provider course number: ______
Name of delegating RN: ______Hire Date: ______ALP training completed: ______
Does the program employ: LPNs CNAs CMAs Universal Workers
Staffing patterns per shift: 1 Revised 8-27-14 a.m. shift: General Population ______Dementia Unit ______p.m. shift: General Population ______Dementia Unit ______night shift: General Population ______Dementia Unit ______
Have direct care staff been trained by a RN and demonstrated their competency to an RN? Yes No Program Name: ______Date: ______
MEDICATION ADMINISTRATION
Does the program have a list of medications taken by tenants who self-administer Yes No
Are medications stored in tenant’s rooms Centralized medication room Medication cart
______# of tenants who self-administer ______# of tenants who receive medication administration
Medications locked when administered by the program? Yes ___ No ___ Narcotics count completed Yes ___ No __ Shift count ___ Weekly___
Medication administration times: ______
List the following information by full name (be specific with full name of tenant listed):
______# of tenants who are known sex offenders ______
______# of tenants with a waiver from the department as they exceed level of care, i.e. hospice, recent hospitalization, etc.
______
______# of tenants with managed risk statements. Do these tenants have a GDS of 4>
______
______# of tenants hospitalized in last three months
______
______# of tenants/spouses who receive veteran’s benefits
______
______# of tenants who have eloped from the program
______
______# of tenants who wander throughout the program.
______
______# of tenants for whom funds are managed
______
______# of tenants who require or wish to use bedrails 2 Revised 8-27-14
______
______# of tenants with a history of suicidal ideation ______
______# of tenants who experienced theft of personal belongings, medications ______
______# of tenants who are consistently refusing personal and/or health related cares ______
______
Program Name: ______Date: ______
______# of tenants receiving Hospice care ______
Tenant: ______Hospice Agency Name: ______Phone Number: ______Address: ______City: ______State: ______Zip: ______Hospice RN: ______Hospice Contact: ______
Tenant: ______Hospice Agency Name: ______Phone Number: ______Address: ______City: ______State: ______Zip: ______Hospice RN: ______Hospice Contact: ______
Tenant: ______Hospice Agency Name: ______Phone Number: ______Address: ______City: ______State: ______Zip: ______
3 Revised 8-27-14 Hospice RN: ______Hospice Contact: ______
4