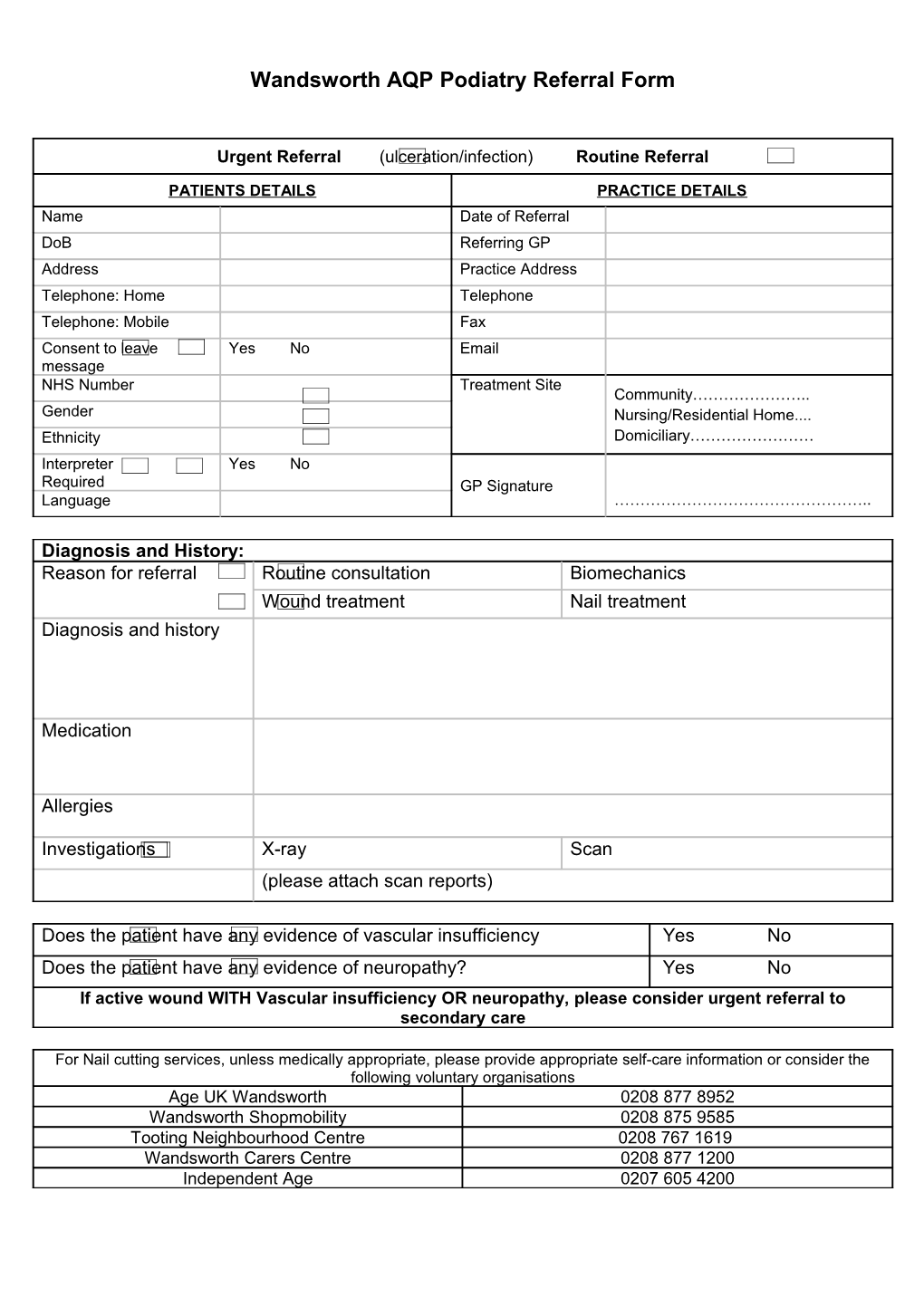
Wandsworth AQP Podiatry Referral Form
Urgent Referral (ulceration/infection) Routine Referral
PATIENTS DETAILS PRACTICE DETAILS Name Date of Referral DoB Referring GP Address Practice Address Telephone: Home Telephone Telephone: Mobile Fax Consent to leave Yes No Email message NHS Number Treatment Site Community………………….. Gender Nursing/Residential Home.... Ethnicity Domiciliary…………………… Interpreter Yes No Required GP Signature Language …………………………………………..
Diagnosis and History: Reason for referral Routine consultation Biomechanics Wound treatment Nail treatment Diagnosis and history
Medication
Allergies
Investigations X-ray Scan (please attach scan reports)
Does the patient have any evidence of vascular insufficiency Yes No Does the patient have any evidence of neuropathy? Yes No If active wound WITH Vascular insufficiency OR neuropathy, please consider urgent referral to secondary care
For Nail cutting services, unless medically appropriate, please provide appropriate self-care information or consider the following voluntary organisations Age UK Wandsworth 0208 877 8952 Wandsworth Shopmobility 0208 875 9585 Tooting Neighbourhood Centre 0208 767 1619 Wandsworth Carers Centre 0208 877 1200 Independent Age 0207 605 4200