B&NES Primary Care Talking Therapies Service Referral Form
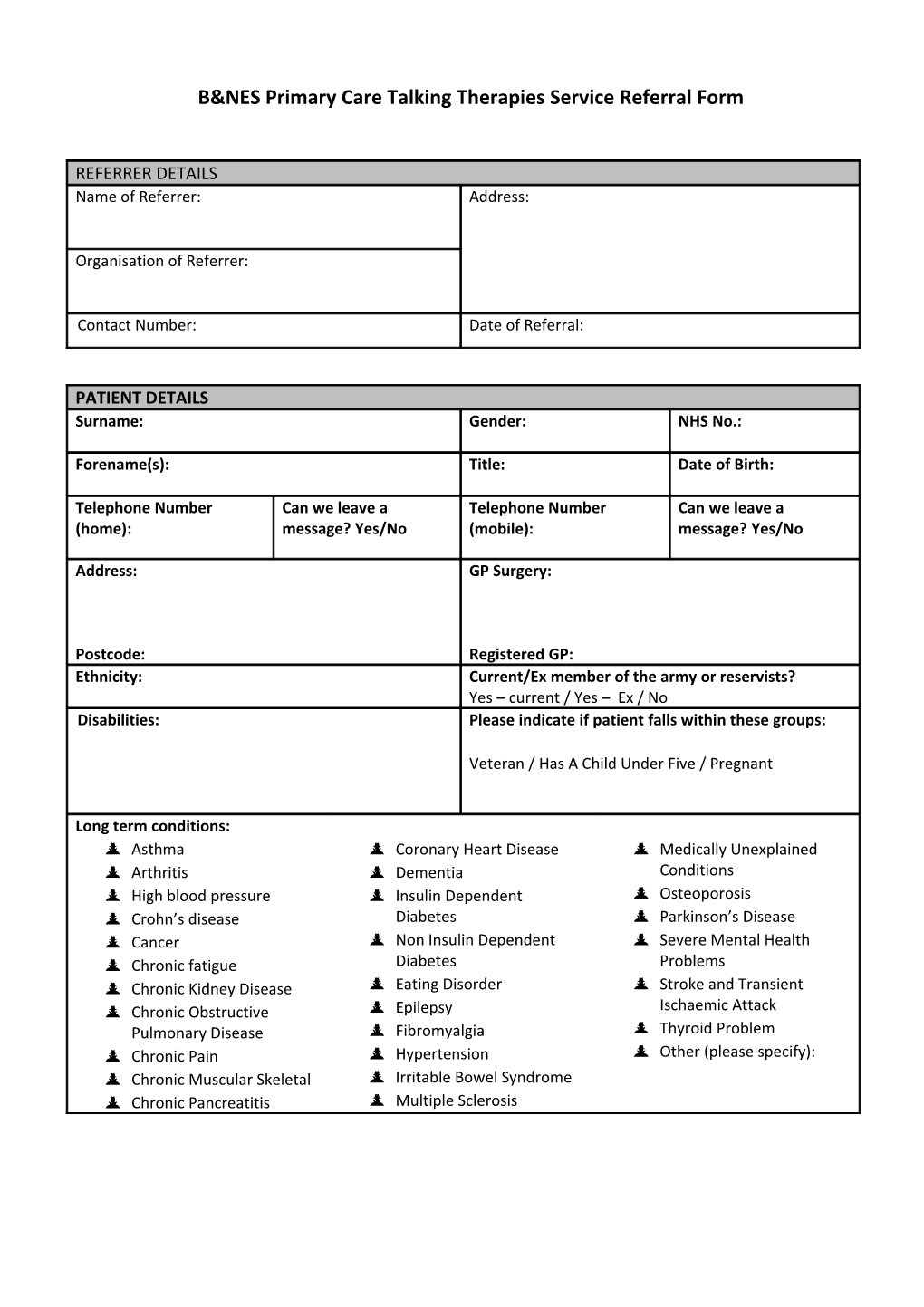
REFERRER DETAILS Name of Referrer: Address:
Organisation of Referrer:
Contact Number: Date of Referral:
PATIENT DETAILS Surname: Gender: NHS No.:
Forename(s): Title: Date of Birth:
Telephone Number Can we leave a Telephone Number Can we leave a (home): message? Yes/No (mobile): message? Yes/No
Address: GP Surgery:
Postcode: Registered GP: Ethnicity: Current/Ex member of the army or reservists? Yes – current / Yes – Ex / No Disabilities: Please indicate if patient falls within these groups:
Veteran / Has A Child Under Five / Pregnant
Long term conditions: Asthma Coronary Heart Disease Medically Unexplained Arthritis Dementia Conditions High blood pressure Insulin Dependent Osteoporosis Crohn’s disease Diabetes Parkinson’s Disease Cancer Non Insulin Dependent Severe Mental Health Chronic fatigue Diabetes Problems Chronic Kidney Disease Eating Disorder Stroke and Transient Chronic Obstructive Epilepsy Ischaemic Attack Pulmonary Disease Fibromyalgia Thyroid Problem Chronic Pain Hypertension Other (please specify): Chronic Muscular Skeletal Irritable Bowel Syndrome Chronic Pancreatitis Multiple Sclerosis REFERRAL INFORMATION Reason for referral- PLEASE ATTACH CARE PLAN AND RISK ASSESSMENT :
Risk Information (Please provide any information about current or previous self-harm or suicide risks):
Previous contact with mental health services (please include any previous psychological therapy):
Any other relevant information (please include information concerning why the patient is unable to self-refer and how best for us to contact the patient):
OFFICE USE Date Received: IAPTUS No.:
Please fax this form to 01225 362799 or email to [email protected] or post to: BANES Primary Care Talking Therapies Service, Hillview Lodge, RUH, Bath, BA1 3NG. Guidance for BPCTTS Referrals
The majority of individuals self-refer into our service, they can do this by contacting our service directly on 01225 675150. We also offer a range of psycho-educational courses that can be booked directly through our website, http://iapt-banes.awp.nhs.uk. If a patient is able to self-refer, please provide them with a ‘working it out’ leaflet and encourage them to do so.
This referral form is for the minority of individuals who are unable to self-refer. Below is a list of people that we typically work with, as well as our exclusion criteria. If you are making a referral to our service, please ensure that the patient fits this criteria. If you are unsure you can contact our office and ask to speak to a duty practitioner.
People We Typically Treat Exclusion Criteria
• People who fit within the traditional IAPT • People who are at immediate or unstable framework – ie: mild/moderate anxiety risk (no consolidated period of stability) and/or depression AND • Main problem is an eating disorder and • Moderate/Severe anxiety disorders their BMI (Body Mass Index) indicates any and/or depression risk • People under the care of Specialist • People experiencing a current psychotic Mental Health Services episode • People who have a diagnosis of • Anyone under 16 yrs Personality Disorder or who may • People who present a risk to staff experience similar symptoms and are willing/able to engage in regular group • People using drugs or alcohol to a level treatment that would prevent them engaging in • People who use drugs or alcohol treatment • People with long term health conditions • People who are not stable enough to engage in a talking therapy • People with psycho-sexual difficulties • People wanting long term therapy • Bereavement • People under the care of Specialist Mental • Couples Health Services who are engaged in specialist psychological treatment with • Relational difficulties the Therapies Team • Stress
• Carers