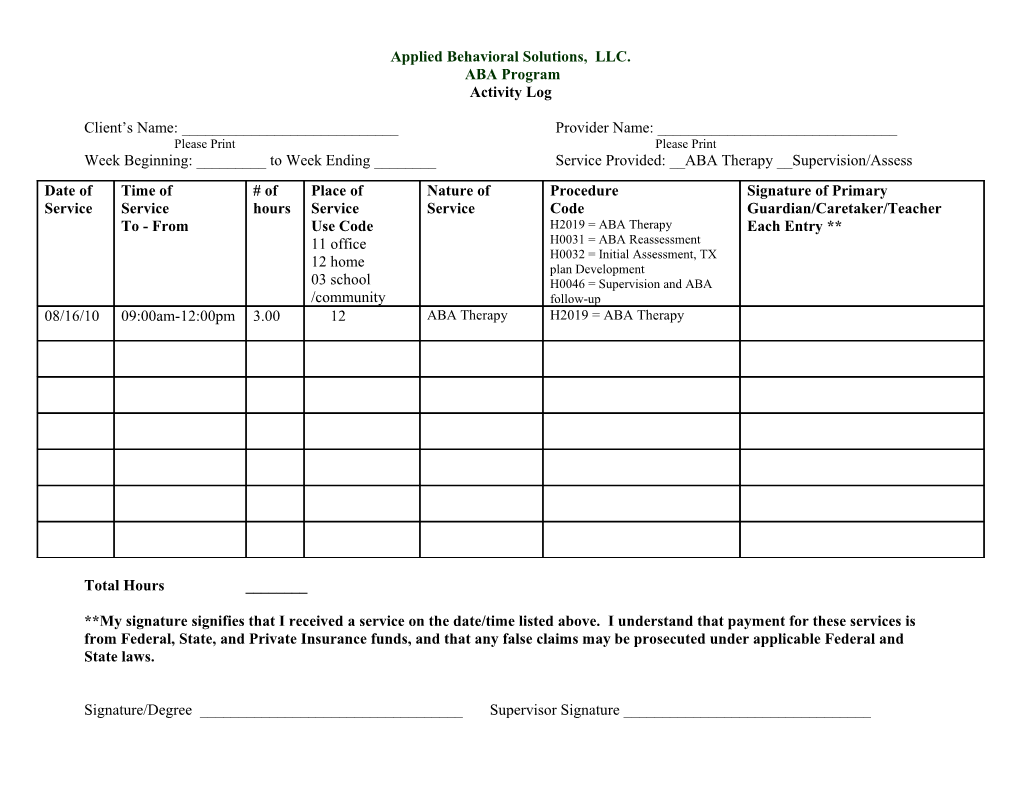
Applied Behavioral Solutions, LLC. ABA Program Activity Log
Client’s Name: ______Provider Name: ______Please Print Please Print Week Beginning: ______to Week Ending ______Service Provided: __ABA Therapy __Supervision/Assess Date of Time of # of Place of Nature of Procedure Signature of Primary Service Service hours Service Service Code Guardian/Caretaker/Teacher To - From Use Code H2019 = ABA Therapy Each Entry ** 11 office H0031 = ABA Reassessment H0032 = Initial Assessment, TX 12 home plan Development 03 school H0046 = Supervision and ABA /community follow-up 08/16/10 09:00am-12:00pm 3.00 12 ABA Therapy H2019 = ABA Therapy
Total Hours ______
**My signature signifies that I received a service on the date/time listed above. I understand that payment for these services is from Federal, State, and Private Insurance funds, and that any false claims may be prosecuted under applicable Federal and State laws.
Signature/Degree ______Supervisor Signature ______