Fundamentals: 10:00 - 11:00 Scribe: Myra Dennis
Friday, October 30, 2009 Proof: Hillary Carney Dr. Waites Neisseria and Chlamydia Page 1 of 9
I. Neisseria and Chlamydia II. Objectives a. We’re going to continue talking about groups of bacteria and the diseases they cause. First we’ll talk about neisseria and chlamydia, and the 2nd hour we’ll talk about spirochetes and rickettsiae. I put neisseria and chlamydia together – not they have anything to do with one another in terms of the type of bacteria they are – but they cause similar types of diseases so they fit nicely together. So like we did earlier in the week, we’ll talk about their characteristics, epidemiology, how they produce the diseases they produce, and how we would identify them from a diagnostic standpoint. We have several organisms within these groups that we’ll speak about: 2 species of neisseria and 3 in the chlamydia group. III. Neisseria meningitidis a. N. meningitidis is a gram negative bacteria and a coccus. It usually appears as a diplococcus, meaning it appears in pairs. These are neutrophils, and you see it will often be inside the neutrophils. It will be little small, gram negative cocci that will be in pairs inside cells when you look in body fluids. IV. N. meningitidis
a. They possess the enzyme cytochrome oxidase, so they are oxidase positive. They like to grow in CO2, so they’re considered capnophiles. They’re non-motile. This particular organism is not especially fastidious (fastidious means it requires special and complex cultivation requirements). We think of the organism Neisseria gonorrhea as very fastidious. Neisseria meningitidis is not quite so fastidious because it will grow on regular sheep blood agar - like you saw with the staph and strep in the lab earlier this week - as well an enriched media (chocolate agar). V. The Meningococcal Cell Wall a. N. meningitidis is also known as the meningococcus. The structure of the cell wall is shown here. Since it’s a gram negative organism, it’s structure is very different from gram positive. You’ve not had the lectures on other gram negatives yet, but remember Dr. Yoker talked with you last week about the basic differences between gram positive and gram negative bacteria in terms of the inner and outer cytoplasmic membrane, the lipopolysaccharide (a component of the endotoxin that’s present there). And that’s what you see here in this diagram of the cell wall. This is very important because the endotoxin is the most significant virulence factor of N. meningitidis. VI. N. meningitides - Pathogenesis a. In addition to the endotoxin that’s responsible for many of the clinical manifestations you get when you get a systemic infection with this organism, such as the shock and disseminated intervascular coagulation, you also have a capsule. The capsule, as in other bacteria, helps protect the organism from phagocytes in the host. b. Thirdly, another virulence factor of the organism is an IgA protease. Remember, IgA is the immunoglobulin present in body secretions (saliva, respiratory tract, mucosal surfaces). It’s main role is to bind microorganisms that come into the body through the mucosal surfaces and bind them and then fix complement and opsonize them for phagocytosis. One of the ways the N. meningitidis has of getting around this and avoiding the host immune system is by breaking open the IgA. So if the IgA is cleaved, it cannot effectively bind the organism. So this is a very important defense mechanism it has. VII. Nasopharynx -> Blood -> CSF a. N. meningitidis is primarily an organism that causes severe disease because it can get into the central nervous system and cause meningitis. This is the organism you here about, especially in schools where high school students have spinal meningitis, where there’s an outbreak of it and several people are sick. This is a very serious illness because you can be fairly normal and feel good this morning, and then the organism can invade your body, and by dinnertime tonight, you can be quite ill, and you can be in a coma and die within a matter of hours. So it’s a very rapidly progressing illness. That’s why it’s important to recognize it and treat it quickly. b. The organism invades the body through the nasopharynx, and from there it goes to the bloodstream, and it may go to the cerebrospinal fluid following that. Many people may actually carry the organism in their nose. There are multiple serotypes of the organism. The reason you see outbreaks in schools, etc. is where you have several people together in close approximation and the organism is present in the Fundamentals: 10:00 - 11:00 Scribe: Myra Dennis
Friday, October 30, 2009 Proof: Hillary Carney Dr. Waites Neisseria and Chlamydia Page 2 of 9 respiratory tract so it can be spread by droplets. So you can exchange serotypes. The serotype your body has adapted to may not be causing your body any trouble, but if you acquire a different strain from someone else through respiratory droplets, then this organism is not adapted to your body and it may cause disease. This is why it’s a significant condition because it has a fairly high mortality. c. Not every case goes on to spinal fluid. This organism rarely may cause sore throat, it can get into the lungs, the respiratory tract. Sometimes we see it in the blood stream without meningitis. But the most significant thing is the meningitis. VIII. N. meningitis Serotypes a. There’s 13 different immunological types – or serogroups – based on the different polysaccharide capsule antigens. This is analogous to what we saw in other organisms like Streptococcus pneumoniae, which has multiple serogroups. b. The serogroups A, B, and C are the most common in terms of causing most of the cases of meningococcal disease. c. A is particularly important as a cause of epidemics. B, C, and Y - sometimes they cause sporadic disease and outbreaks in developed countries. In the US, serogroup A is the predominant one. IX. Colony Morphology a. This is what the organisms look like. On chocolate agar, you can see them as yellowish/gray mucoid- like, fairly translucent nice-sized colonies. We’ll actually see some of these in the lab next week; we’ll have a demonstration of neisseria colonies. X. Oxidase Positive a. One of the key features to help you identify this bacteria is the oxidase test. This is something else you’ll do in the lab next week. To do an oxidase test, you take some of your bacterial colonies on a swab and add the oxidase reagent to it. If the organism possesses the enzyme cytochrome oxidase, you’ll see a vivid purple color develop very soon on the swab. XI. N. meningitidis Carbohydrate Metabolism a. The other way to distinguish N. meningitidis from other neisseria is through carbohydrate oxidations. N. meningitidis uses glucose and maltose. So that distinguishes it from organisms such as Neisseria gonorrhoeae that use only glucose. This is important to differentiate which one is which this way, and it’s the basis of how we can identify it in the microbiology lab looking at the different metabolic substrates that it uses. XII. N. meningitidis Epidemiology a. As far as the diseases that this organism causes, this is a leading cause of bacertial meningitis, and especially in older children and young adults. Sporatic in the community but in institutions with a lot of people crowded together, it can cause outbreaks when you have several people who can get the organism together. b. About 2,800 people in the US get this disease every year. We see a few cases each year at UAB that mainly come through our hospital emergency department. But the significant thing is, meningococcal meningitis has about a 10-15% mortality. And among the survivors, many people have permanent neurologic sequelae because the inflammation of the brain can permanently damage some of the neurological structures. You can get visual, hearing, speech, motor, and cognitive defects as a result of damage to the brain this way. Invasive disease can be fatal within hours. So it’s very important that anyone who has manifestations of meningitis – such as photophobia, headache, stiff neck, change in cognition or sensorium – you would suspect meningitis and have them appropriately evaluated. A lumbar puncture to examine the spinal fluid is important, because you can do a gram stain on the spinal fluid and if you see the organisms (like a gram negative intercellular diplococci) you’ve made the diagnosis just by seeing the organism on the gram stain and seeing the inflammation. But you would also culture it. c. This is the only type of meningitis that causes epidemics, because it is very contagious. Streptococcus pneumoniae can also meningitis that will appear similar to this. But this is the one that produces the outbreaks, several cases together, and this one is actually worse than pneumococcal meningitis because the organism has the endotoxin and that can cause hypotension, shock, and cardiovascular collapse more so than the pneumococcus can. Fundamentals: 10:00 - 11:00 Scribe: Myra Dennis
Friday, October 30, 2009 Proof: Hillary Carney Dr. Waites Neisseria and Chlamydia Page 3 of 9 d. If you were to look in the eyes of someone with meningitis with an ophthalmoscope – and important part of the physical exam because you’re looking for elevated areas of intracranial pressure. If you have acute swelling of the brain because of meningitis and the inflammation and swelling of the tissures it produces, this can put pressure on the optic nerves. With the ophthalmoscope you would see papilledema, a swollen optic disc. That’s an important clue in the diagnosis of meningitis – swelling of the brain that’s caused increased intracranial pressure. XIII. Incidence of Culture Confirmed Meningococcal Disease a. This is fairly old data, but the point we’re making hasn’t changed. The occurrence of meningitis has a spike in the teenage and early adulthood years. This is noted because it’s about the time people are in high school, college, and living in dorms close together. XIV. N. meningitidis Epidemiology a. Only present in humans, it doesn’t have an animal reservoir. It is spread by the respiratory tract. About 10-15% of people may actually be colonized on a long-term basis with the organism. XV. N. meningitis Risk Factors a. So who gets the meningitis and why do they get it there? If you live in the household of someone with meningistis, you’re at risk for it. This is why you have to take prophylactic antibiotics if someone you’re in close contact with develops meningococcal meningitis. Boarding schools/military camps. b. They do vaccinate college students and military recruits for this. [a lot of the class raised their hand and said they’d had the vaccine] A lot of you have, because this is routinely offered now when people go to college, because you are at risk if you’re living in crowded conditions and dorms. It makes good sense to get the vaccine. c. Lower socio-economic status, exposure to tobacco smoke, recent upper respiratory infections. If you don’t have a spleen (asplenia), you’re at risk. This is an encapsulated microorganism, and the spleen’s an important part of the reticulo-endothelial system that protects us from infections with invasive, encapsulated bacteria. If you were in a car accident and you’re spleen was damaged and you had to have it removed, or if you’re a sickle cell anemia patient and you’ve infarcted you’re spleen because of the abnormality of the blood cells. If you don’t have a functional spleen you’re at risk for it. d. If you have any type of complement deficiency, especially terminal complement deficiency, you’re at risk for invasive meningococcal disease. These are genetic defects in the complement system. This is really waving a red flag. Anyone who has more than one case of invasive meningococcal disease, you always have to see if they have a complement deficiency since that’s very closely associated with it. XVI. Meningococcal Disease a. The most serious disease from it you can get is meningitis. You can also get bacteremia, bloodstream infection. Meningococcemia (sepsis) is where you get petiqei and perfura (not sure what these two words were). XVII. Meningococcal Meningitis – Clinical Symptoms a. The effect of the endotoxin, the lipopolysaccharide on the circulatory system causes significant drops in blood pressure and bleeding throughout the body, and this is why you get petechia and purpura. It’s important you look at the skin of someone you suspect has meningitis to see if you can see any red spots on the skin (petechia) that won’t blanch when you press them or if they begin to have large bruise-like areas (ecomoses). That means you have initiated the disseminated intravascular coagulation, the blood clotting problem you get because of the endotoxin effects. In some cases you get the Waterhouse-Friderichsen Syndrome, where you have bleeding into internal organs, particularly the adrenal gland. Another effect of the endotoxin. b. Occasionally you can get respiratory infections with the organism. Usually it’s an acute situation but in some cases you can get more prolonged periods with it. c. As I said before: headache, stiff neck, photophobia, altered mental status, fever, nausea, vomiting, rash, and in some cases pneumonia may be the way some patients present with meningococcal disease. XVIII. Petechiae and Purpura a. This is a patient with meningococcal sepsis. You see the petechiae on the skin that in some cases have coalesced to purpura. This can progress in a matter of a few hours from the time someone is healthy till they develop this severe syndrome of disseminated disease. XIX. Waterhouse-Friderichsen Syndrome Fundamentals: 10:00 - 11:00 Scribe: Myra Dennis
Friday, October 30, 2009 Proof: Hillary Carney Dr. Waites Neisseria and Chlamydia Page 4 of 9 a. These are the adrenal glands collected at autopsy showing widespread hemorrhage and necrosis as a result of the endotoxin effects from the meningococcemia in the adrenal gland, in the Waterhouse- Friderichsen Syndrome. XX. N. meningitis a. This is the brain of someone with meningococcal meningitis. The skull has been opened from the top. This is the dura mater, the outer part of the meniges. The brain is covered with pus. See very large numbers of neutrophils in spinal fluid and the bacteria that are there. XXI. Meningococcal Meningitis Prognosis a. People that have shock, a severe rash, a low white count (a poor immune response to the organism), older people, and people that development coma are all people that have a poor outcome. And then remember what I mentioned earlier about the sequelae of the survivors. XXII. Prevention of Meningococcal Disease a. So what can you do to keep from getting it? If you’re exposed to it, there’s antibiotics you can take to prevent it. If you’re a healthcare worker and someone comes in with meningitis and you’re exposed to it, an antibiotic is used. XXIII. Meningococcal Vaccine a. And then of course there’s the vaccine. There’s a new conjugate vaccine that was licensed in 2005. The vaccine is recommended for people in high risk categories. People going into the military, children in their teenage years. Can also vaccinate people during an outbreak, because you’ll get a fairly brisk immune response. If you’ve got several cases in a school, go ahead and vaccinate everyone else that’s close. If you’re traveling into an area that’s known to have an outbreak. College students, complement deficiencies, people who don’t have a spleen. Also lab workers. A few years ago a tech in Huntsville, AL acquired an infection and died. So this is why all people working in microbiology labs that may work with the organism should get vaccinated. XXIV. Vaccine Limitations a. This is a vaccine based on the polysaccharide, the capsule antigens. It does not provide protection against serogroup B, because that particular capsule is not immunogenic in the vaccine. Since it’s a polysaccharide vaccine, the original vaccine is not good for children under 2 years of age because very young children don’t respond very well to polysaccharide antigens. We do have a new conjugate vaccine that may work better now because it’s conjugated to a protein to stimulate a better immune response. b. So we have 2 different vaccines, one we can use in younger children (2-10 years) and those over 55. And then another to use for teenagers and middle-aged people. Studies are being done to see how long this vaccine will work. Since this is not a permanent vaccine, if you’re exposed to menigococcus over and over, you have to repeat the vaccine every few years so you can get a booster effect and longer lasting immunity. So it’s not something you take once in your life and have protection forever. c. So that’s N. menigitidis. XXV. Epidemiology of Major STDs in USA a. The other organism we’ll mention is Neisseria gonorrhea. This graph talks about several of the organisms we’re talking about today. These are some of the major sexually transmitted diseases in the US and the number of people that have them. The most common one - Chylamidia trachomatis, followed closely by N. gonorrhea, human papilloma virus, herpes virus, syphilis, hepatis B virus, trichamonis, chancroid, LGV and GI (these are much less common). But the big one’s we’ll talk bout are chlamydia, gonorrhea, and syphilis. These are important STDs. They’re very different organisms, but all can be transmitted venerealy. For many years, Birmingham has been famous as being the STD capital of the country. It’s very common. XXVI. Neisseria gonorrhoeae a. N. gonorrhoeae is similar in many ways to N. meningitidis. It looks just like it. Just look at a gram stain. This is the gram stain of a penile urethral discharge in a man that had gonorrhea. It looks just like the spinal fluid of N. meningitidis. XXVII.Neisseria gonorrhoeae - Characteristics a. They’re very different organisms and have different epidemiological associations, but they look the same and have a lot of the same characteristics. This one is more fastidious, it will not grow on regular Fundamentals: 10:00 - 11:00 Scribe: Myra Dennis
Friday, October 30, 2009 Proof: Hillary Carney Dr. Waites Neisseria and Chlamydia Page 5 of 9 blood agar, you have to grow it on chocolate agar, blood agar that’s been heated to open the red blood
cells and release the factors the bacteria need to grow. And you have to give it CO2. Very susceptible to drying, so have to keep it warm and moist. XXVIII. N. Gonorrhoeae Pathogenesis a. It can be transmitted sexually or vertically (from mother to her baby at time of vaginal birth – the baby can get severe infections of the eyes. Can get ophthalmia neonatorum because of the eye infection). b. The organism has pilli, structure that allow it to attach to cells. It also has the opacity proteins in the outer membrane that facilitate cell invasion. Since it’s gram negative it has endotoxin. It also has tissue toxin in form of peptidoglycan. It lives inside cells so it’s protected from the immune system to some degree. Like menigococcus it has an IgA protease. c. You can get N. gonorrhoeae over and over. It has evolved a very sophisticated means of varying its surface antigens. It can change the proteins it expresses on the surface of its cell. This keeps the immune system guessing. Even though you may develop antibodies against a neisseria strain you have, the next time you encounter a strain of gonorrhoeae it will have different antigens. So you’re immune system won’t recognize it and you start all over again. d. Has multiple antibiotic resistance. Resistant penicillin – so this is a very adept organism at outwitting the things we try to do to control it. Because it’s so genetically unstable, there’s no vaccine because of the problems with antigenic variation. We do have a nice vaccine for menigococcus. XXIX. N. Gonorrhoeae Detection a. Here you see it growing on chocolate agar. When we grow it from genital tract of women we have to put antibiotics in there because there’s the nonpathogenic neisseria that can cause problems. b. We have several species in our mouth as a part of normal flora. Sometime when you suspect neisseria, you do have to do the appropriate biochemical, phenotypic tests to see which neisseria it is – whether it’s one of the commensal organisms or a pathogen. If man has penile discharge and you see gram negative intracellular diplococci on a gram stain, that’s sufficient for a diagnosis. But a culture is necessary in women, because do have some normal flora present in lower genital tract. So need to do culture or PCR. We’re almost stopped doing cultures because we have PCR-based test we can do on urine species (men or women) that will detect N. gonorrhoeae as well as Chlamydia trachomatis. That makes it so easy to do the test – get the result right away and don’t have to do a culture. Because these
are very fastidious, and very susceptible to cold, stress, and require CO2, so have to be very careful when trying to grow them. XXX. N. Gonorrhoeae Diseases a. Male urethritis. If the urethra is squeezed, pus will be expressed from the urethra. That will send a man to the doctor more quickly than just about anything you can think of! There’s about a 20-30% chance of transmission. The problem is that many women may have asymptomatic gonorrhoeae. It’s much less likely for a man to be asymptomatic than it is for a woman. Women can carry the organism and have minimal symptoms. They can spread it to multiple sexual partners even though they don’t realize they have it themselves. b. Complications in men or women include arthritis. The organism can get into the bloodstream and the joints. A very common cause of septic arthritis. c. Pelvic inflammatory disease - in women it’s transmitted to cervical area. It can go up into the uterus and get into the fallopian tubes. It’s very pyrogenic, a lot of pus is produced. It can get into the fallopian tubes and cause an inflammatory reaction, then it causes scarring after it heals. If have multiple gonorrhea infections and it goes up into the upper reproductive tract, the scarring can give a completely blocked fallopian tube. This can make you infertile, or it can cause a tubal pregnancy because if you partially block the tube from scarring (fertilization occurs in the fallopian tube and the it implants in the uterus) and the sperm makes it up there to undergo fertilization in the fallopian tube, the embryo may be blocked from getting to the uterus so the embryo implants in the tube. It gets larger, you have a ruptured tube, and it can kill you if you don’t seek medical attention right away. So those are big complications of gonorrhoeae as well as chlamydia that can cause the same kind of thing. d. And depending on sexual habits you can get gonorrheal disease in other parts of the body. Men with men can get proctitis. You can get a sore throat from pharyngeal sex. e. Also, can get ophthalmia neonatorum. Fundamentals: 10:00 - 11:00 Scribe: Myra Dennis
Friday, October 30, 2009 Proof: Hillary Carney Dr. Waites Neisseria and Chlamydia Page 6 of 9 XXXI. Ophthalmia Neonatorum a. Eyelid of a new born baby. See the conjunctiva here, the pyrulates on here. This is neonatal ophthalmia. This can occur due to gonorrhoeae or chlamydia if the mother is infected at time of delivery and the organism is inoculated on the baby’s eyes. This is why all newborns get antibiotic eye drops at birth because of the possibility there might be undiagnosed gonorrhoeae in the mother that could cause this infection. It can cause permanent damage to the ocular tissues if not treated appropriately. XXXII. Neisseria gonorrhoeae Prevention a. We don’t have a vaccine for gonorrhoeae. The best thing is to use condoms to help prevent the transmission. Education about the disease. For the baby, can use silver nitrate or antimicrobial drops in neonatal eyes at birth. Antibiotics are preferred over the silver nitrate, because silver nitrate is somewhat toxin and causes somewhat of a chemical conjunctivitis in the eyes too. b. Student question: Would there be any problems with the development of the eye because of this? i. Answer: This happens when the baby is born and passes through an infected birth canal, then it manifests itself within a couple of days. So it comes fairly quickly once it happens. Don’t see too much of it because babies get antibiotic drops in their eyes to prevent it. Because many women may not know they have because they’re often asymptomatic. XXXIII. Chlamydia trachomatis a. Much of what he said about N. gonorrhea in terms of the disease it produces is true of Chlamydia trachomatis. Some differences as we go along – the organisms are really extremely different. XXXIV. Chlamydia trachomatis Characteristics a. Chlamydia is the first one we’ve talked about that’s an obligate intracellular bacteria. All the others we’ve been hearing about are very evolved organisms that can cultivated in vitro in a lab if have the right kind of agar plate you can get them to grow. Don’t have to give them cells or anything else, because given an energy source they’re able to live independently. Chlamydia are intracellular parasites. They are unable to generate ATP for their metabolite reactions, so they have to use (somewhat like a virus) the ATP from host cells. So that’s why they’re obligate intracellular organisms. Chlamydia and rickettsiae (in next lecture) most fall into that category. b. They don’t have peptidoglycan in cell wall – they do have a cell wall and are essentially a gram negative bacterium. Have a very unique intracytoplasmic groth cycle. They grow inside cells and make inclusions inside the cells (see image). Their growth inside the cells is possible because have mechanisms by which they prevent phagolysosome fusion, so this allows them to grow and proliferate inside host cells. Can stain with microbiological stains such as giemsa stain, but not a gram stain because they don’t have peptidoglycan. c. There are 15 different serological types of it. XXXV. Chlamydia Life Cycle a. This is the life cycle of chlamydia – common to all chlamydial species. You have an infectious particle called an elementary body, which is what is transmitted from person to person. If these elementary bodies are encountered through sexual activity or respiratory droplets (in the case of the respiratory chlamydias), they then encounter the host epithelial cells in the lower urogenital tract. They’re taken up by pinocytosis into the host cell and establish a phagosome there. Then, inside the phagosome where they’re allowed to live because they prevent the lysosomal enzyme activity there, they become metabolically active and turn into reticulate bodies. Then the reticulate bodies start reproducing the elementary bodies, and over about a 3 day period the elementary bodies start developing more and more and finally the cell ruptures and dies to release the elementary bodies which then go on to find a new cell and the infection spreads. b. So it’s a fairly complicated life cycle, all of which takes place inside the host cells of the organ that the chlamydia are infecting. XXXVI. Chlamydia trachomatis - Pathogenesis a. The way the organism produces disease is that it does stimulate the inflammatory response. You can get infection in different parts of the body. We normally think of genital infections. The organism attaches to the mucosal epithelium. It’s chemotactic for neutrophils, so do get an inflammatory response. Don’t usually see the pus as much as you do with the gonorrhea, it’s not as strongly a Fundamentals: 10:00 - 11:00 Scribe: Myra Dennis
Friday, October 30, 2009 Proof: Hillary Carney Dr. Waites Neisseria and Chlamydia Page 7 of 9 pyrogenic organism as N. gonorrhea. So the discharge you would see with chlamydia urethritis (non- gonococcal urethritis) would be more watery and not as pyralous. b. Chlamydia trachomatis is also a pathogen of the eye. It causes a condition known as trachoma that can be transmitted from person to person through hand contact. You’re eyes itch, you rub your hands, then touch someone else. See this in crowded conditions, poor hygiene, in developing countries primarily. Ultimately get fibrosis and scarring of the eyelid and conjunctiva because of the infection. This is a condition called inclusion conjunctivitis because you can do scrapings of the conjunctiva and stain it, and can see chlamydia inclusions inside the cells. That’s why it’s called inclusion conjunctivitis. XXXVII. Chlamydia trachomatis – Detection a. Since these are very fastidious and obligate intracellular organisms, we can’t just put on agar plate and grow them. Can do cell cultures like how we grow viruses, and stain the inclusions with monoclonal antibodies and see them under a fluorescent microscope. That’s what we still have to do for eye infections. But for genital infections, the urethritis, the PCR, the nuclear acid amplification test, is now the method of choice. There are still non-amplified antigen detection tests but they’re hardly used anymore because they’re not as sensitive as the PCR test, which detects smaller numbers. XXXVIII. Ocular Trachoma a. Here’s a patient with inclusion conjunctivitis. A cobblestone, lumpy appearance of the conjunctiva. This is ocular trachoma. We don’t see this too much in the more well-developed, higher socioeconomic areas in the US. But worldwide, especially in poorer countries with poorer hygiene and crowded conditions, it’s estimated to cause infections in 400 million people. 4 of them - A, B, Ba, and C - are most likely to cause ocular trachoma. b. This is the keratoconjunctivitis you get. The organism is having the same life cycle here (the elementary and reticulate bodies) except it’s doing all this in the conjunctiva cells when it invades the tissues of the eye. XXXIX. Neonatal Infections due to C. trachomatis a. Just like the gonorrhea, you can get the same type thing in babies if the organism is transmitted into the ocular tissues at birth. Unlike gonorrhea, in addition to the ocular conditions, chlamydia is also known to produce pneumonitis. Because when the baby comes through the birth canal, covered with the mother’s secretions, the first thing the baby does is cries, takes a depth breath. When it inhales, any of the secretions from the mother that’s on the face, nose, and mouth can be inhaled. If you’ve got chlamydia in them, you’ve got a nice new place to grow and do your life cycle down in the respiratory tract. Several days later, the baby starts having shortness of breath, wheezing, and requires oxygen, and can get pneumonitis as a result of chlamydia pneumonitis. XL. C. trachomatis Genital Disease in Adults a. In men, it’s a non-gonococcal urethritis. b. In women it’s inflammatory cervicitis. It’s one of the most common sexually transmitted infections. You can get all the same complications with this organism that you can get with gonorrhea in women. Like the gonorrhea, many women are asymptomatic, don’t know they have it, so they can spread it around to their sexual partners. XLI. Lymphogranuloma Venereum a. Lymphogranuloma Venereum is a variant of chlamydia diseases that’s caused by 3 particular serotypes of chlamydia. It’s much less common than the urethritis. You get the organism spreading to the lymph nodes and the inguinal region, and produces big, swollen, sore lymph nodes. This is the inguinal region here – see the large red swollen area. A big swollen lymph node in the groin. Not nearly as common as urethritis. XLII. Prevention of C. trachomatis Infections a. Like gonorrhea, there’s no protective immunity following a chlamydia infection, and there’s no vaccine. The way to prevent it to improve hygiene, use antibiotics on babies, and education on STDs for young people especially to learn where these things come from. XLIII. Chlamydophila psittaci a. Some other Chlamydia diseases, that don’t affect as many people or as seriously, but you should be familiar with the names. A few years ago the genus we refer to as chlamydia was subdivided and the Fundamentals: 10:00 - 11:00 Scribe: Myra Dennis
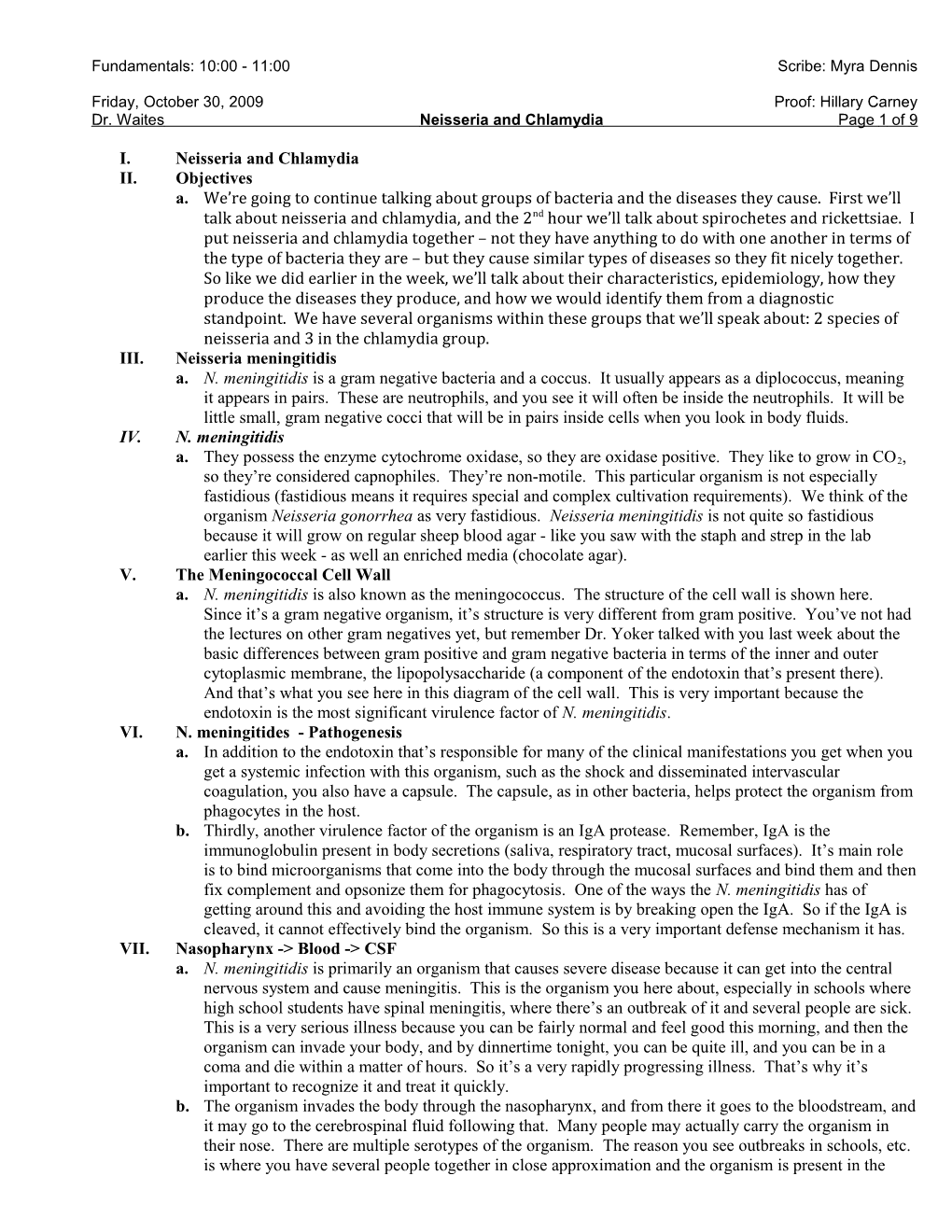
Friday, October 30, 2009 Proof: Hillary Carney Dr. Waites Neisseria and Chlamydia Page 8 of 9 genus name chlamydia was kept for the genital infections and a new genus called chlamydophila was used for the respiratory chlamydia because they weren’t as closely related. b. Chlamydophila psittaci is the agent of parrot fever. Carried by parokets and parrots, that is sometimes transmitted to humans. It almost always an occupational or habit disease – someone who keeps birds. The birds deposit the organisms in their feces. If you’re cleaning the birdcage, you may inhale the organism, and you may get a pneumonitis in the lung because the bacteria life cycle grow in the lung. You get a cough, congestion, mucus. It’s usually not too severe, but you can make the diagnosis usually by looking at an antibody response to the chlamydophila. XLIV. Chlamydophila pneumoniae a. In the mid-1980s, several people were seen that had a respiratory infection. It wasn’t clear what the diagnosis of this was, so doctors thought well maybe they’ve got this “parrot fever.” So they sent them to be tested for an antibody response. Several of them were coming back positive. Yet these patients didn’t have a history of being exposed to birds. b. It was a different species of chlamydophila – same type of life cycle. This is an electron micrograph of it. You see it here in the lung of a patient. This was a different species, not associated with birds, but a cause of community-acquired respiratory disease. Now we know this organism can cause pneumonia, sore throat, sinusitis, bronchitis, very similar to microplasm we’ll talk about on Monday. It’s a very low-grade pathogen and many people are asymptomatic with it. It can affect children, adults, anyone. c. Very seldom diagnosed because it’s such a fastidious organism. Very few places try to culture it. You can detect it by PCR. There are some antibody test available for it, but it’s not widely used and no one’s sure how good they are. Usually it’s just treated symptomatically, and very rarely a diagnosis is made. d. It’s been getting a lot of attention, because it’s a slow-growing indolent organism that can spread throughout the body. Almost every adult has some antibody to it because everyone’s exposed to it. Observations made in the mid-1990s show you could find evidence by PCR or serology of infection in people with coronary atherosclerosis. The antigens of this organism were found in the arterial walls of people with atherosclerosis. So researchers were saying that this is a risk factor for coronary heart disease, so you should be treating people with coronary heart disease with antibiotics. Eventually we’re going to find more and more implications of microorganisms as a cause of a lot of diseases. For example, we know helicobacter causes ulcers, a lot of different kinds of cancers are caused by microorganisms. So it’s not too far-fetched that coronary artery disease might be associated with chlamydophila. There is some data based on detection of antigen. But by no means is this a settled fact. If you get this it’s probably an immunologic reaction to something that occurred over many years, a chronic infection, so a simple course of antibiotics is not going to give you new arteries. e. This also stimulated a lot of intense research to look at other chronic diseases for which there was no clear cut cause, so there’s also been a suggestion that this causes multiple sclerosis. Some people believe it does, but it’s inconclusive.
END 50 MIN. Fundamentals: 10:00 - 11:00 Scribe: Myra Dennis
Friday, October 30, 2009 Proof: Hillary Carney Dr. Waites Neisseria and Chlamydia Page 9 of 9