RADIOLOGY CASE REPORT
Student: Rami Abdelshaheed Student #: 4338639
Patient ID: OH# 04182754 Date of Study: May 4, 2007
Type of Study: Chest X Ray
1. Clinical Indication:
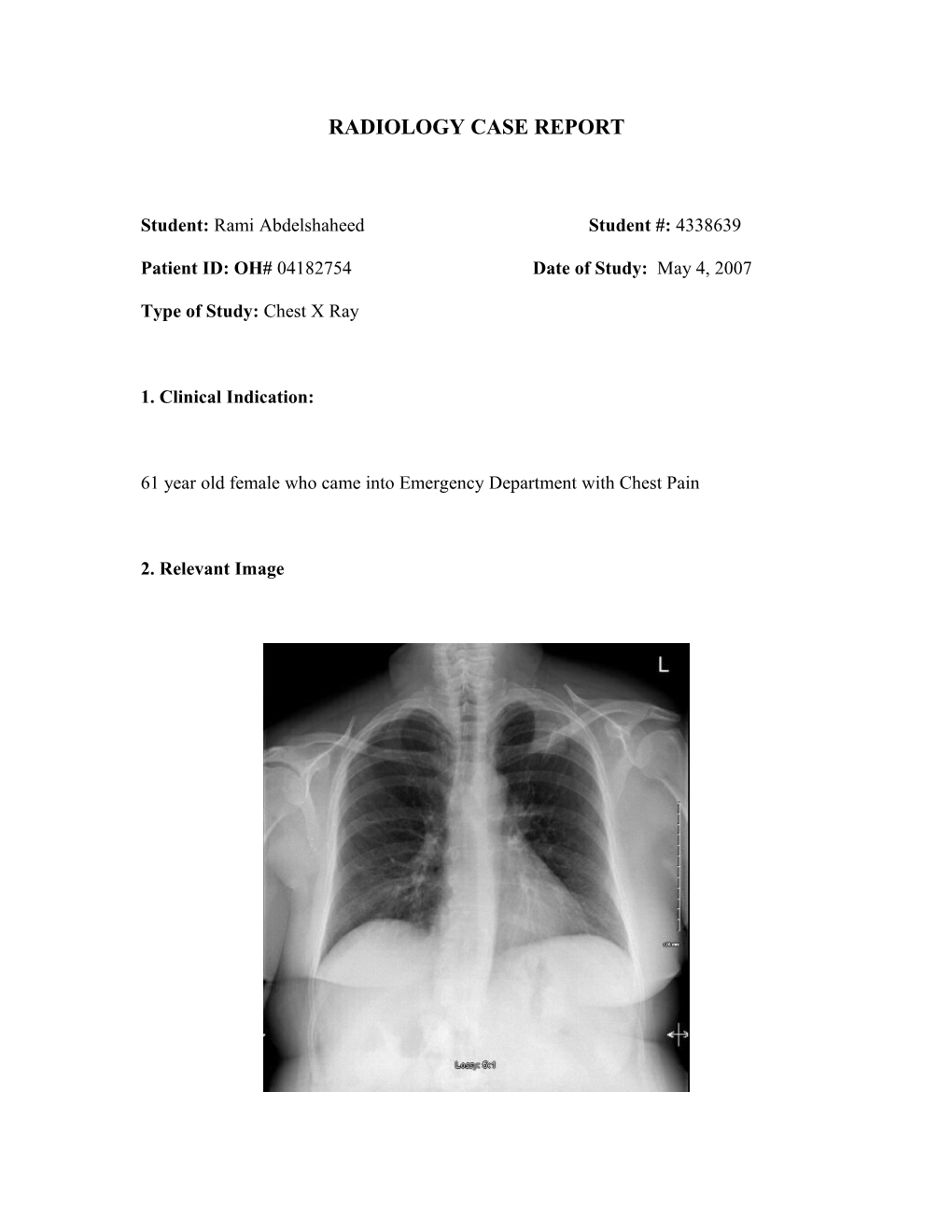
61 year old female who came into Emergency Department with Chest Pain
2. Relevant Image 2. Describe the radiological findings:
There is a triangular opacity in the apical segment of the Left Upper Lobe.
The right breast shadow appears smaller than the left in keeping with a previous right mastectomy with right axillary lymph node dissection.
The bony thorax demonstrated no bony metastases.
The cardiomediastinal silhouette appears unremarkable.
No hilar lymph nodes are noted.
The lungs are otherwise clear.
3. Provide possible diagnosis(es):
Bronchogenic carcinoma
o Maybe Pancoast tumor
Metastatic Malignancies given the history of Right breast mastectomy
Mesothelioma
Fungal Infection
Tuberculosis
Lung abscess
Atypical pneumonia
4. What would you recommend next for this patient?
The next logical step would be to compare the Chest X ray with a previous chest X ray. If this mass was not present on a recent previous Chest X ray then a diagnosis of cancer would be less likely as the mass would not have grown at such a rapid pace. Rapid progression would support an infectious cause. CT Scan is the next logical step for this patient. This will enable the physician to assess the nodular opacity and evaluate its consistency and contents in order to characterize the lesion.
If it is truly a tumor, CT will also be able to assess the size and volume of the tumor, mediastinal involvement, pathologically enlarged lymph nodes, and vascular invasion.
Also, a biopsy would have to be planned in the near future.
If clinically the patient presented with signs and symptoms consistent with a pancoast tumor (Shoulder pain, Weakness/atrophy and paresthesias of the hand/arm/forearm or
Horner syndrome - ptosis, miosis, and anhidrosis) then MRI would be the modality of choice as it is more accurate in the evaluation of extension to the vertebral body, spinal canal, brachial plexus, and subclavian artery. This is clinically relevant as invasion may be a contraindication to surgical resection.
5. Is the use of this test/procedure appropriate?
Yes the use of this test is appropriate. Characterization of the opacity is a critical step in the diagnosis of this lesion. If the lesion is felt to be a tumor, CT will also enable the clinician to accurately stage the tumor and therefore will also guide management decisions.
6. Is(are) there any alternate test(s)?
MRI is an alternate imaging modality which may be used. Generally it is not used as an initial imaging tool however maybe very useful in secondary evaluation. As mentioned above, MRI is has several advantages over CT which can be useful including its ability to better image the vertebral body, spinal canal, brachial plexus, and subclavian artery.
Another advantage is the lack of ionizing radiation exposure to the patient.
7. How would you explain to the patient about the possible risks and benefits of this test?
CT scanning is associated with low level radiation exposure. Radiation is a necessary part of a CT. Although low, there has been some research that has shown some correlation with low level radiation exposure and increased risk of cancer. The risk of this is very low and the potential benefits from this examination far out weigh the risks. The information provided from the CT in necessary in order to make an appropriate diagnosis and therefore assist the physician in determining the correct course of action in this case.
8. What is the cost of this test?
A CT will cost approximately $700 (American source).