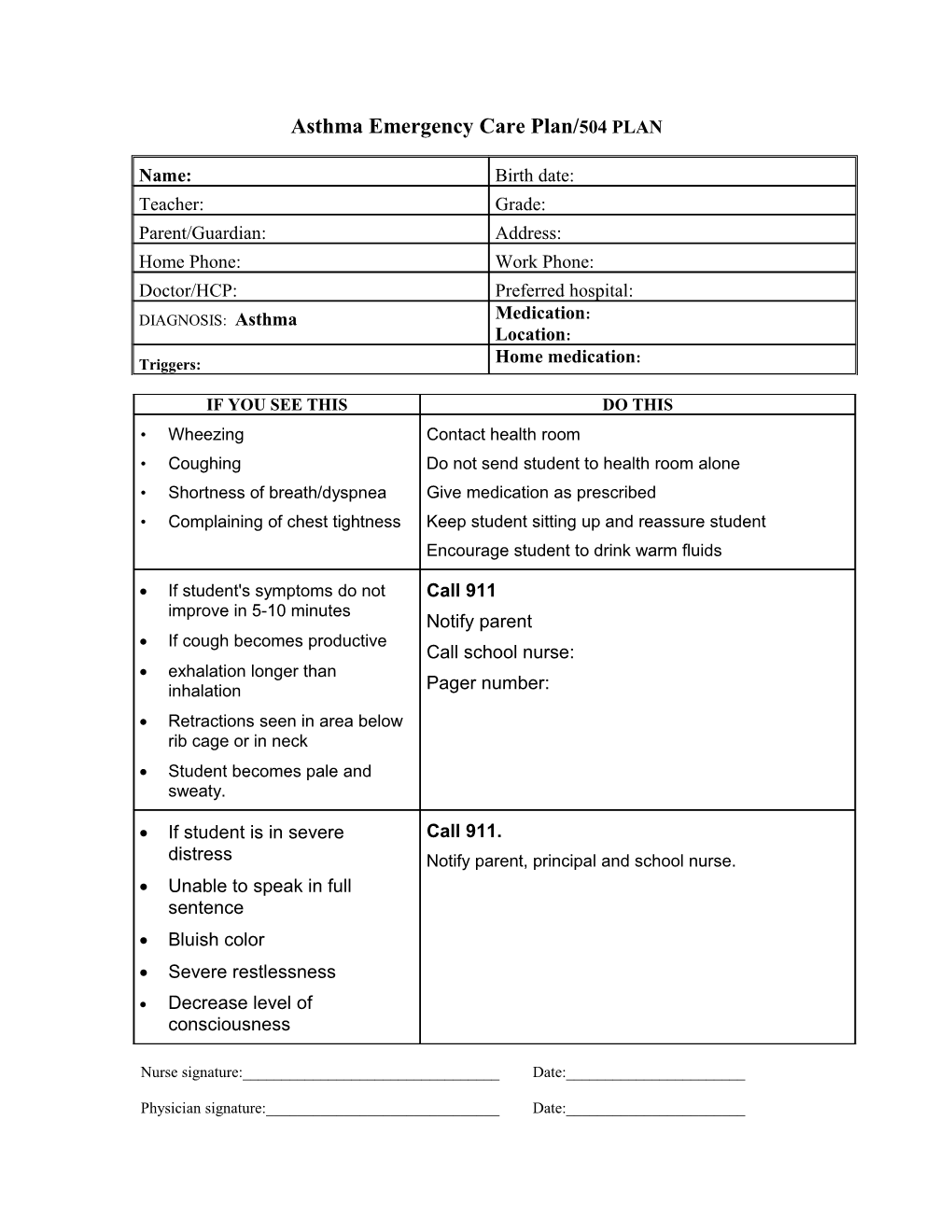
Asthma Emergency Care Plan/504 PLAN
Name: Birth date: Teacher: Grade: Parent/Guardian: Address: Home Phone: Work Phone: Doctor/HCP: Preferred hospital: DIAGNOSIS: Asthma Medication: Location: Triggers: Home medication:
IF YOU SEE THIS DO THIS • Wheezing Contact health room • Coughing Do not send student to health room alone • Shortness of breath/dyspnea Give medication as prescribed • Complaining of chest tightness Keep student sitting up and reassure student Encourage student to drink warm fluids
If student's symptoms do not Call 911 improve in 5-10 minutes Notify parent If cough becomes productive Call school nurse: exhalation longer than inhalation Pager number: Retractions seen in area below rib cage or in neck Student becomes pale and sweaty.
If student is in severe Call 911. distress Notify parent, principal and school nurse. Unable to speak in full sentence Bluish color Severe restlessness Decrease level of consciousness
Nurse signature:______Date:______
Physician signature:______Date:______INDIVIDUAL HEALTH/EMERGENCY CARE PLAN CONTACT INFORMATION
STUDENT:
E-MAIL: ______
NAME/Relationship #1 PHONE (Type) #2 PHONE (Type) #3 PHONE (Type)
Updated:
Parent signature:______Date:______