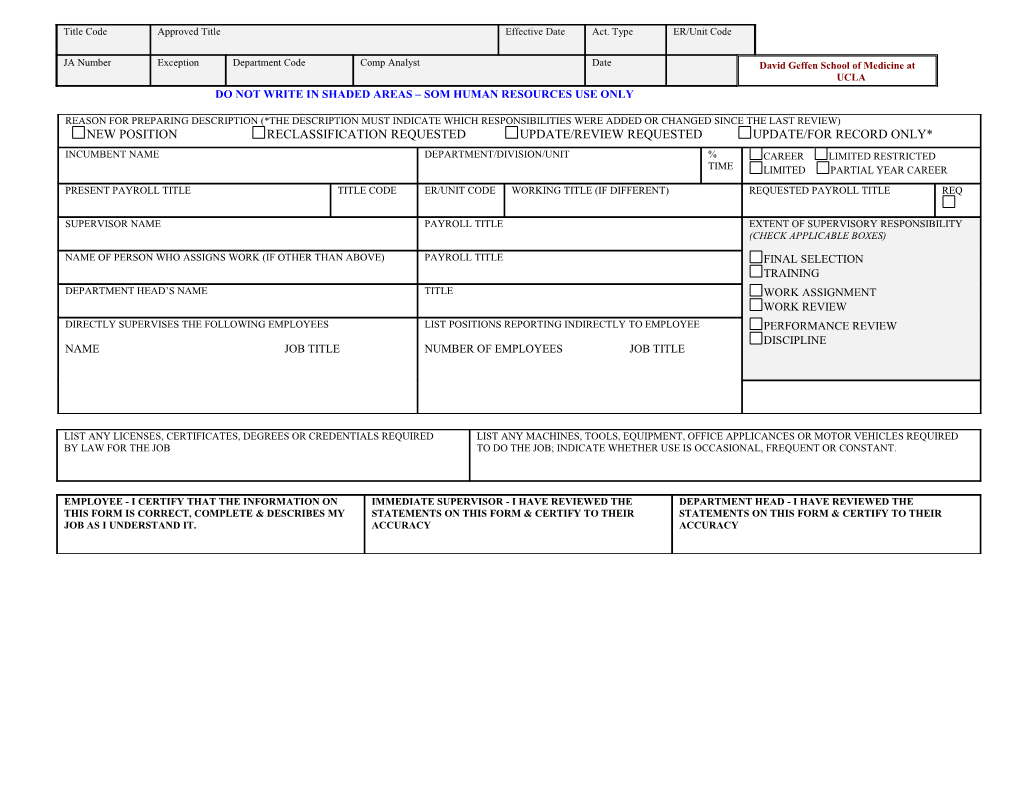
Title Code Approved Title Effective Date Act. Type ER/Unit Code
JA Number Exception Department Code Comp Analyst Date David Geffen School of Medicine at UCLA DO NOT WRITE IN SHADED AREAS – SOM HUMAN RESOURCES USE ONLY
REASON FOR PREPARING DESCRIPTION (*THE DESCRIPTION MUST INDICATE WHICH RESPONSIBILITIES WERE ADDED OR CHANGED SINCE THE LAST REVIEW) NEW POSITION RECLASSIFICATION REQUESTED UPDATE/REVIEW REQUESTED UPDATE/FOR RECORD ONLY*
INCUMBENT NAME DEPARTMENT/DIVISION/UNIT % CAREER LIMITED RESTRICTED TIME LIMITED PARTIAL YEAR CAREER
PRESENT PAYROLL TITLE TITLE CODE ER/UNIT CODE WORKING TITLE (IF DIFFERENT) REQUESTED PAYROLL TITLE REQ
SUPERVISOR NAME PAYROLL TITLE EXTENT OF SUPERVISORY RESPONSIBILITY (CHECK APPLICABLE BOXES)
NAME OF PERSON WHO ASSIGNS WORK (IF OTHER THAN ABOVE) PAYROLL TITLE FINAL SELECTION TRAINING DEPARTMENT HEAD’S NAME TITLE WORK ASSIGNMENT WORK REVIEW DIRECTLY SUPERVISES THE FOLLOWING EMPLOYEES LIST POSITIONS REPORTING INDIRECTLY TO EMPLOYEE PERFORMANCE REVIEW DISCIPLINE NAME JOB TITLE NUMBER OF EMPLOYEES JOB TITLE
LIST ANY LICENSES, CERTIFICATES, DEGREES OR CREDENTIALS REQUIRED LIST ANY MACHINES, TOOLS, EQUIPMENT, OFFICE APPLICANCES OR MOTOR VEHICLES REQUIRED BY LAW FOR THE JOB TO DO THE JOB; INDICATE WHETHER USE IS OCCASIONAL, FREQUENT OR CONSTANT.
EMPLOYEE - I CERTIFY THAT THE INFORMATION ON IMMEDIATE SUPERVISOR - I HAVE REVIEWED THE DEPARTMENT HEAD - I HAVE REVIEWED THE THIS FORM IS CORRECT, COMPLETE & DESCRIBES MY STATEMENTS ON THIS FORM & CERTIFY TO THEIR STATEMENTS ON THIS FORM & CERTIFY TO THEIR JOB AS I UNDERSTAND IT. ACCURACY ACCURACY
SUMMARY STATEMENT
TYPE OF SUPERVISION RECEIVED
HOW LONG HAVE THE DUTIES & DISTRIBUTION OF ATTACH A COPY OF MOST RECENT ORGANIZATION TIME BEEN SUBSTANTIALLY AS BELOW? CHART AMOUNT OF TIME DUTIES AND TASKS
SKILLS, KNOWLEDGE AND ABILITIES TASK IMPORTANCE REFERENCE