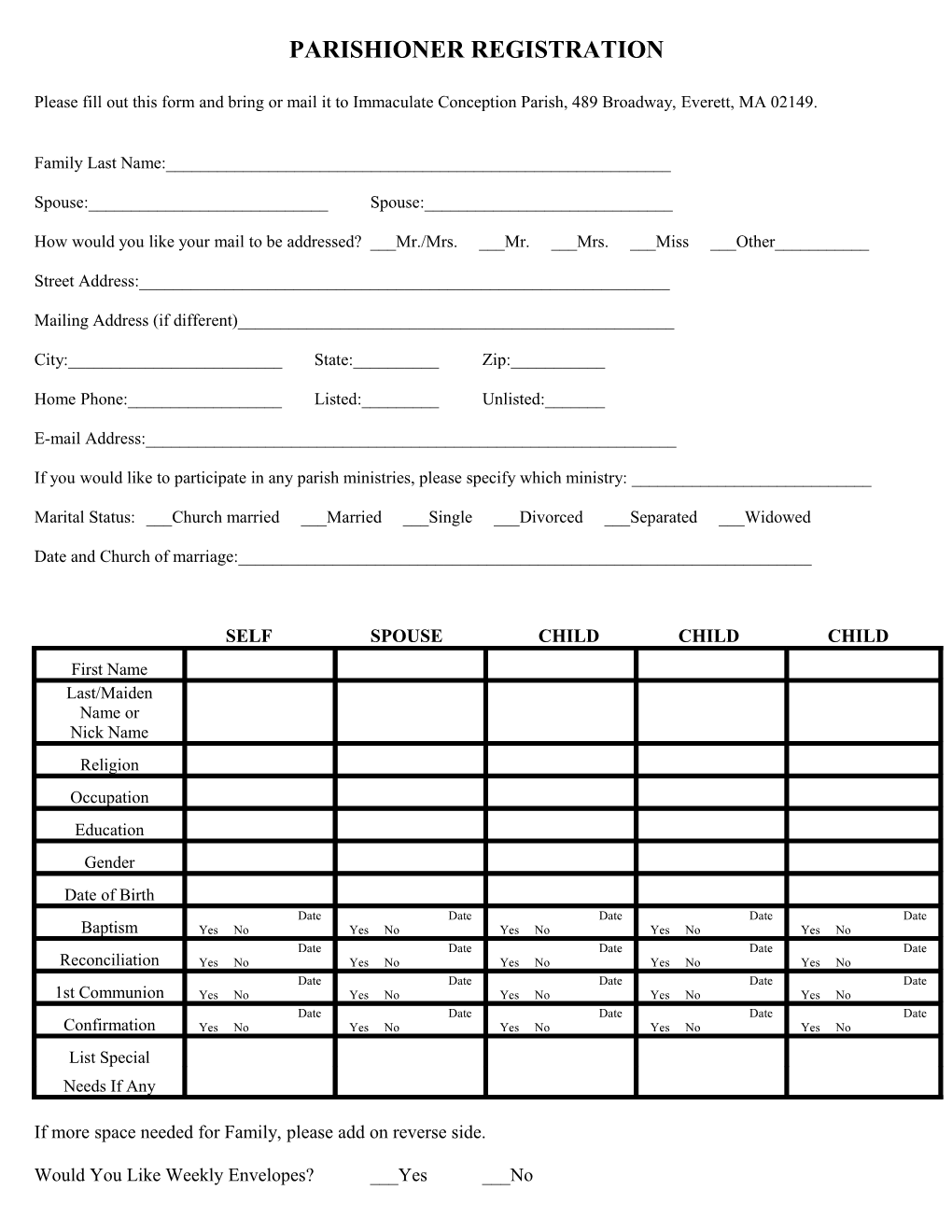
PARISHIONER REGISTRATION
Please fill out this form and bring or mail it to Immaculate Conception Parish, 489 Broadway, Everett, MA 02149.
Family Last Name:______
Spouse:______Spouse:______
How would you like your mail to be addressed? ___Mr./Mrs. ___Mr. ___Mrs. ___Miss ___Other______
Street Address:______
Mailing Address (if different)______
City:______State:______Zip:______
Home Phone:______Listed:______Unlisted:______
E-mail Address:______
If you would like to participate in any parish ministries, please specify which ministry: ______
Marital Status: ___Church married ___Married ___Single ___Divorced ___Separated ___Widowed
Date and Church of marriage:______
SELF SPOUSE CHILD CHILD CHILD First Name Last/Maiden Name or Nick Name Religion Occupation Education Gender Date of Birth Date Date Date Date Date Baptism Yes No Yes No Yes No Yes No Yes No Date Date Date Date Date Reconciliation Yes No Yes No Yes No Yes No Yes No Date Date Date Date Date 1st Communion Yes No Yes No Yes No Yes No Yes No Date Date Date Date Date Confirmation Yes No Yes No Yes No Yes No Yes No List Special Needs If Any
If more space needed for Family, please add on reverse side.
Would You Like Weekly Envelopes? ___Yes ___No FAITH FORMATION REGISTRATION
Please fill out this form and bring or mail it to Immaculate Conception Parish, 489 Broadway, Everett, MA 02149.
Family Last Name:______
Spouse:______Spouse:______
How would you like your mail to be addressed? ___Mr./Mrs. ___Mr. ___Mrs. ___Miss ___Other______
Street Address:______
Mailing Address (if different)______
City:______State:______Zip:______
Home Phone:______Listed:______Unlisted:______
E-mail Address:______
If you would like to participate in any parish ministries, please specify which ministry: ______
Marital Status: ___Church married ___Married ___Single ___Divorced ___Separated ___Widowed
Date and Church of marriage:______
SELF SPOUSE CHILD CHILD CHILD First Name Last/Maiden Name or Nick Name Religion Occupation Education Gender Date of Birth Date Date Date Date Date Baptism Yes No Yes No Yes No Yes No Yes No Date Date Date Date Date Reconciliation Yes No Yes No Yes No Yes No Yes No Date Date Date Date Date 1st Communion Yes No Yes No Yes No Yes No Yes No Date Date Date Date Date Confirmation Yes No Yes No Yes No Yes No Yes No List Special Needs If Any
If more space needed for Family, please add on reverse side. Would You Like Weekly Envelopes? ___Yes ___No Envelope No.______
This form will be sent to the Parish to update your records.