A Guide to Implementing the NYU Caregiver Intervention
Alzheimer’s Disease Support Services Program October 2009
Authors Mary Mittelman Dr.PH Cynthia Epstein LCSW
This project is supported, in part, by grant number 90AZ2809/01 from the Administration on Aging, Department of Health and Human Services, Washington DC 20201 and the Minnesota Board on Aging, St Paul, MN 55155. Grantees undertaking projects under government sponsorship are encouraged to express freely their findings and conclusions. Points of view or opinions do not, therefore, necessarily represent official Administration on Aging or Minnesota Board on Aging policy.
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 1 Executive Summary
This manual is a guide to translating the NYU Caregiver Intervention (The NYUCI) and a description of the Minnesota experience of its implementation in four sites. In the original study at NYU, which was a randomized controlled trial, spouse caregivers who received the intervention experienced improved social support, which led to significantly fewer symptoms of depression, improved physical health and less severe reactions to behavioral symptoms of dementia than those who received usual care. As a result, they were able to avoid premature or inappropriate nursing home placement of their ill spouses for an average of approximately one and a half years longer than those in the control group (Mittelman, et. al. 2006*).
When implementing this intervention in your state, it is important to make every effort to maintain fidelity to the original NYUCI. Therefore it may be useful to be aware of the issues that came up during the translation from research to practice in Minnesota. The discussion of translational issues from the perspectives of the researchers and the community service providers in Minnesota illuminate the issues.
This manual provides resources and tools to support your work. Throughout the manual, there are comments from the Minnesota coaches about their experiences, which illustrate situations that arose in the course of providing this intervention.
Section 1 of this manual is a description of the original NYUCI and has been written by Mary Mittelman, Dr.PH and Cynthia Epstein LCSW. The text summarizes the intervention and its components. Included with the manual is a copy of Counseling the Alzheimer’s Caregiver: A Resource for Health Care Professionals (AMA Press, Chicago, 2003) which describes the intervention in more detail. This section also includes a summary of the issues involved in translation of the intervention from the perspective of the researchers.
Section 2 describes Minnesota’s experience with this caregiver intervention, and has been written by Deborah Paone, Evaluator, and Donna Walberg, Project Director. In Minnesota, the intervention was called the “Family Memory Care Program.” This section uses the RE-AIM framework (Reach, Effectiveness, Adoption, Implementation, and Maintenance) to walk through the components of
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 2 implementing the intervention in Minnesota and compares this experience with the New York experience.
There are two “special focus” chapters: (1) the experiences of caregivers, and (2) a cost analysis conducted in Minnesota for the first four implementation sites. You will find material in the Appendix corresponding to these chapters, including the Caregiver Experience Survey instrument and the Cost Analysis Workbook, which may be helpful in the process of implementation. In the concluding section of this manual, we provide lessons learned from Minnesota’s experience, based on implementation from 2007-2009.
This manual will help you to implement the intervention with fidelity. While modifications may be desirable in different settings as new issues arise, it is essential to maintain the essence of the intervention. Key elements include involving the family in support of the spouse caregiver, and offering counseling and support to all participating family members throughout the course of the disease. In order to assure that the modifications you are considering are consonant with the original evidence- based intervention, consult with Mary Mittelman, Dr.PH, who conducted the original research at the NYU, Langone Medical Center. Any agreed-upon changes should be documented, and the reasons for them should be explained in writing. The Administration on Aging has developed a formal approval process for any modifications to the original intervention. Modifications to the intervention cannot be made without prior approval of Dr Mittelman and the Federal Administration on Aging. The guidelines and modification request submission form is included in Appendix 1 Intervention Modifications Guide.
Always keep in mind that the purpose of this intervention is to maintain or improve the well-being of a spouse caring for a partner with Alzheimer’s disease and his or her family members.
* Mittelman, Mary S., Epstein, Cynthia, Pierzchala, Alicia. Counseling the Alzheimer’s Caregiver: A Resource for Health Care Professionals. AMA Press, Chicago, 2003.
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 3 Section 1: The Original NYU Caregiver Intervention Mary Mittelman and Cynthia Epstein
History
This intervention evolved from the informal counseling and support that four clinicians were offering to families at New York University in the early 1980s. These family members were accompanying relatives who went to what has now become the NYU Alzheimer’s Disease Center for a comprehensive diagnostic evaluation because changes in their memory and cognitive function had become a concern. The intervention was formalized by Mary Mittelman, Dr.PH, who applied for funding to the National Institutes of Health to rigorously test its value in improving the well-being of family caregivers and their relatives with Alzheimer’s disease.
The unifying theme of the intervention is that enhancing social support and minimizing family conflict will improve the ability of the family caregiver to withstand the difficulties of caregiving and thereby reduce or defer the need for institutionalization of the person with Alzheimer’s disease. The counseling focuses on each individual caregiver’s needs and improving interactions among the family members to be more constructive. A priority is to strike a balance between increasing the caregiver’s satisfaction with social support and what family members could realistically be expected to provide.
The efficacy of the intervention was evaluated in a longitudinal randomized controlled trial that began in 1987 and has been conducted for more than 20 years at the NYU-ADC (R01 MH42216 and R01 AG14634). The study enrolled 406 spouse caregivers over an 11-year period. This is the largest, longest running study of a counseling and support intervention for spouse caregivers that has ever been conducted. The study had an unusually high retention rate. Only 4.7% of caregivers refused to continue in the study while the patient was still living at home.
Overview of Program The NYU Caregiver Intervention creates a supportive network for the caregiver, building on the strengths of the family. The NYUCI includes assessment, individual and family counseling sessions, support group participation, and ad hoc counseling (counseling as needed on the telephone). It should be noted that prior to enrolling, caregivers should be interviewed (screened) to be sure that there is no serious pathology or physical impediment to participating in the program.
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 4 A comprehensive assessment is implemented at intake and at 4 month intervals during the first year of the program and every six months after that. After the initial assessment interview, there are a total of six counseling sessions within four months of enrolling in the program. First there is one individual session with the spouse caregiver followed by 4 sessions with the spouse caregiver and other family members. There is then a second individual session with the spouse caregiver. Caregivers are encouraged to join a support group after the last counseling session if they have not done so already. During the entire course of the program all participants are encouraged to call the counselor for additional counseling and support, referrals or resources – ad hoc counseling
Spouse caregivers remain in the program even after placement of the person with Alzheimer’s disease (AD) in a nursing home and until 2 years after the death of the person with AD. When the person with AD is no longer living at home with the caregiver, the assessment will be changed to reflect changes in the residence of the person with AD, or his or her death. Ongoing support is an essential part of the intervention, and is available to the spouse caregiver until two years after the death of the patient.
Summary of Intervention Components The intervention components are summarized below and described in greater detail later in this chapter: Initial Contact The Initial Contact in person, by phone or mail sets the stage for the engagement of the participant.
Initial Screening The Initial Screening determines if the spouse caregiver and family are eligible to participate in the intervention and interested in enrolling.
Initial Assessment The Initial Assessment provides information about the caregiver, care receiver and the family and provides the data against which subsequent data can be compared so that changes in the caregiver can be identified and documented.
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 5 First Individual Session In the first individual session the caregiver is encouraged to discuss what he or she expects to achieve during family counseling. With the benefit of information developed in the assessment the caregiver and counselor identify family members to be invited to the family sessions, how they will be contacted and the time and place for the first meeting. The counselor can help the caregiver to begin to formulate realistic expectations of family members and to be prepared to accept their contributions.
Family Sessions The four Family Sessions provide a forum for everyone to share their understanding of the impact of AD on the spouse-caregiver, the person with the illness and the rest of the family and to develop a support system for the caregiving spouse, the person with AD and for each other.
Final Individual Session The Final Individual Session is the time to review with the caregiver how he or she will integrate the experience of the family meetings for mutual support in the future.
Ad Hoc Contacts Ad Hoc Contacts offer the spouse caregiver and other participating family members the opportunity to contact the counselor as needed for counseling and support.
Alzheimer’s Caregiver Support Groups Support group participation provides ongoing support and contact with peers after formal individual and family sessions have ended.
The Second Assessment The Second Assessment of the spouse caregiver should be conducted after the 6 individual and family sessions have been completed, which should be 4 months after the initial assessment.
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 6 Going Forward The next phase of the program includes scheduled additional follow-up assessments at 4 month intervals for the first year and six month intervals thereafter, and ad hoc counseling as requested by the caregiver or other family members.
NYU Spouse Caregiver Intervention Study Design After a comprehensive baseline assessment, study participants were randomized by lottery to an enhanced treatment group or to a control group that received usual care. All caregivers were interviewed at regular intervals following entry into the study, every four months during the first year and every six months thereafter. Interviews were conducted by family counselors by telephone or in person, on the basis of the respondent's preference. Written consent to participate in the project was obtained from each caregiver, as well as from any other relatives who came to the family counseling sessions. Spouse caregivers were able to remain in the program after placement of the person with AD in a nursing home and until 2 years after the death of the person with AD.
Eligibility criteria for the original study All study participants were caring for a spouse with a clinical diagnosis of Alzheimer’s disease (AD) and had the primary responsibility for their care. All people with Alzheimer’s disease were living at home with their spouses when they enrolled in the study. An additional requirement for participation was that, in each family, the person with Alzheimer’s disease or the caregiver had to have at least one relative living in the New York City metropolitan area. The caregiver had to be emotionally and physically capable of participating.
Treatment and Control Groups The treatment group received all components of the intervention – a total of 6 individual and family counseling sessions within a fixed period of time after enrollment, and ongoing support through participation in a support group and additional counseling as needed, called “ad hoc” counseling. Control participants were provided with the normal counseling services offered to all families of participants at the NYU-ADC, which included information about resources and advice when it was requested, but they did not participate in the formal counseling sessions provided to enhanced treatment participants. They were free to seek additional assistance and support elsewhere.
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 7 Outcome Measures There was a large battery of structured written instruments that provided a detailed assessment of the characteristics, background and social network of the caregiver and the stage of dementia of the ill spouse. The instruments included measures of social support satisfaction; symptoms of depression, reaction to behavior caused by the illness and self-reported health of the caregiver and time to nursing home placement of the person with dementia, all of which were improved by the NYU Caregiver Intervention, compared to the usual care control participants. Other outcomes, such as details of the physical health of the caregiver and the person with dementia were measured in order to provide information that would inform the counseling. When the person with AD was no longer living at home with the caregiver, the assessment was modified; scales that were no longer appropriate were deleted.
Base of Evidence The NYU Caregiver Intervention is listed on the Substance Abuse and Mental Health Services Administration’s National Registry of Evidence Based Programs and Practices (NREPP) website as evidence-based (www.samhsa.nrepp.gov), where the major results of the study are documented. The study has demonstrated that improving social support for spouse caregivers can have major benefits to their well-being, reducing caregiver depression (Mittelman, et al., 1995, 2004a), the effects of caregiving on physical health (Mittelman, et al., 2007) and reactions to problem behaviors caused by Alzheimer’s disease (Mittelman, et al., 2004b), while postponing institutionalization of the person with dementia (Mittelman, et al., 1993, 1996, 2006). The major mediator of these outcomes is improved support from family and friends (Roth et al., 2006).
1. Change in social support as a result of the NYU Caregiver Intervention. Those who provide care at home for a spouse with Alzheimer's disease (AD) endure considerable challenges, including social isolation and increasing caregiving responsibilities. We demonstrated the specific effects of the NYU caregiver intervention on social support from family and friends, which occurred within a few months of enrolling in the study (Mittelman et al., 1997). We found that individuals in the enhanced treatment group reported higher levels of satisfaction with their social support network over the first 5 years of the intervention than those in the usual care control group. Higher levels of emotional support, more visits, and having more network members to whom they felt close predicted improvement in satisfaction with social support (Drentea et al., 2006).
While the number of support network members does not increase, the number to whom the caregiver feels close does increase, as do satisfaction with assistance and emotional support (Roth et al,
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 8 2005). Most recently, in more detailed analyses of social support information collected from 200 spouse-caregivers, using random effects regression models, we found that higher levels of emotional support, more visits, and having more network members to whom they felt close were all individually predictive of longitudinal changes in social support network satisfaction (Drentea et al., 2006).
2. Changes in depression and reaction to problem behavior. Of particular interest and clinical utility is the finding that the intervention has significant effects on caregiver depression for more than 3 years after enrollment in the study (Mittelman et al., 2004a). These effects are significant for both male and female caregivers. Further analyses reveal that while neuroticism is a risk factor for increased caregiver depression over time, it does not preclude successful caregiver intervention with a highly individualized intervention like ours (Yang et al., 2004). The intervention has a marked effect on caregiver reaction to problem behavior, despite having no effect on the behavior itself (Mittelman et al., 2004b).
3. The effects of the NYU Caregiver Intervention on the physical health of caregivers We found that individuals in the enhanced treatment group had significantly better self-rated health than those in the usual care control group and this significant difference was maintained for two years (Mittelman et al., 2007). Similar benefits of intervention were found for number of illnesses. These findings provide evidence that counseling and support can preserve health of vulnerable caregivers.
4. The long-term effects of the NYU caregiver intervention on time to nursing home placement. People with dementia whose spouses received the intervention experienced a 28.3% reduction in the rate of nursing home placement compared with usual care controls. The difference in predicted median time to placement was 557 days. Improvements in caregivers’ satisfaction with social support, response to problem behaviors, and symptoms of depression collectively accounted for 61.2% of the intervention’s beneficial impact on placement (Mittelman et al., 2006). These results extend the findings of earlier reports (Mittelman et al., 1993, 1996).
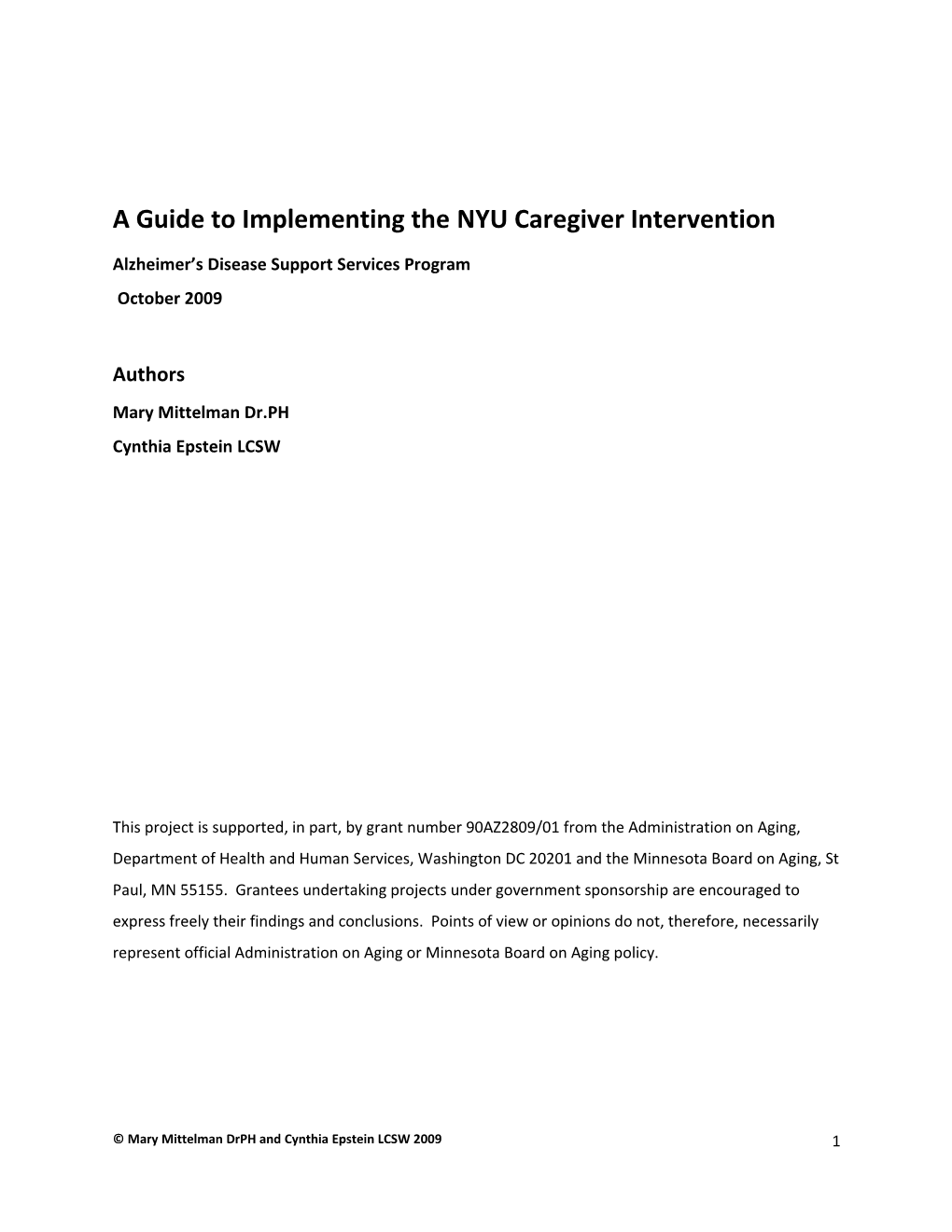
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 9 Fewer caregiver symptoms of depression
Improved social Delayed support for the nursing NYU Caregiver caregiver home placement Intervention Less severe caregiver reaction to patient Improved caregiver behavior physical health*
Figure 1: Demonstrated effects of the NYU Caregiver Intervention. The earliest effects are on the left. They in turn have effects which are portrayed further to t he right. * Note: While the intervention improved caregiver physical healt h, its effects on physical health were insufficient to influence nursing home placement of the per son with dementia
5. The effects of counseling and support on the burden and depressive symptoms of spouse caregivers of people with Alzheimer’s disease during the transition to nursing homes. We found that burden and depressive symptoms were significantly lower for caregivers in the enhanced treatment group when compared to usual care controls at the time of and after institutionalization but that nursing home admission itself significantly reduced burden and depressive symptoms in both groups (Gaugler et al., 2008). These results demonstrate that while institutionalization alone can reduce caregiver burden and depressive symptoms, enhanced counseling provides additional long-term benefits.
6. The effects of the NYU caregiver intervention on caregiver depressive symptoms at the time of bereavement. The death of the care recipient led to reductions in depressive symptoms for both caregiving groups but the counseling and support intervention led to lower depressive symptoms compared with controls both before and after bereavement (Haley et al., 2008). Post-bereavement group differences were stronger for caregivers of spouses who did not previously experience a nursing home placement. For these caregivers, differences were maintained for more than one year after bereavement. Caregivers in the treatment group were more likely to show long term patterns of fewer depressive symptoms before and after bereavement suggesting resilience, while control caregivers were more likely to show chronic depressive symptoms before and after the death of their spouse.
These results attest to the long-term effectiveness of psychosocial intervention for caregivers of people with AD, and the importance of the kind of counseling provided through the NYU Caregiver Intervention. Enhancing support from family members and friends is the mechanism through which the intervention achieves its effects on the well-being of caregivers and their relatives with dementia.
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 10 References cited Mittelman MS, Ferris SH, Shulman E, Steinberg G, Ambinder A & Mackell J (1997). The effects of a multicomponent support program on spouse-caregivers of Alzheimer's disease patients: Results of a treatment/control study. In L.L. Heston (Ed.), Progress in Alzheimer's Disease and Similar Conditions. Washington (DC): American Psychiatric Press. Mittelman M, Ferris S, Shulman E, Steinberg G, Ambinder A, Mackell J, & Cohen J (1995). A comprehensive support program: Effect on depression in spouse-caregivers of AD patients. Gerontologist, 35, 792-802. Mittelman MS, Ferris SH, Shulman E, Steinberg G & Levin B (1996). A family intervention to delay nursing home placement of patients with Alzheimer disease. Journal of the American Medical Association, 276, 1725-1731. Mittelman MS, Roth DL, Coon DW and Haley WE (2004a). Sustained benefit of supportive intervention for depressive symptoms in Alzheimer’s caregivers. American Journal of Psychiatry, 161(5), 850- 856. Mittelman MS, Roth DL, Haley WE & Zarit, SH (2004b). Effects of a caregiver intervention on negative caregiver appraisals of behavior problems in patients with Alzheimer’s disease: Results of a randomized trial. Journals of Gerontology, Psychological Sciences, 59B(1), P27-P34. Roth DR., Mittelman MS, Clay OJ, Madan A & Haley, WE (2005). Changes in social support as mediators of the impact of a psychosocial intervention for spouse caregivers of persons with Alzheimer’s disease. Psychology and Aging, 20(4), 634-644. Drentea P, Clay OJ, Roth DL, Mittelman MS (2006). Predictors of improvement in social support: Five- year effects of a structured intervention for caregivers of spouses with Alzheimer’s disease. Social Science & Medicine, 63, 957-967. Mittelman MS, Haley WE, Clay, O, Roth, DL (2006). Improving caregiver well-being delays nursing home placement of patients with Alzheimer disease. Neurology, 67, 1592-1599. Mittelman MS, Roth DL, Clay OJ, Haley WE (2007). Preserving health of Alzheimer’s caregivers: impact of a spouse caregiver intervention. American Journal of Geriatric Psychiatry, 15, 780-789. Gaugler JG, Roth DL Haley WE & Mittelman MS (2008). Can counseling and support reduce Alzheimer’s caregivers’ burden and depressive symptoms during the transition to institutionalization? Results from the NYU Intervention Study. Journal of the American Geriatric Society, 56:421–42. NIHMSID: NIHMS 113868.
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 11 Haley W E, Bergman EJ, Roth DL, McVie T, Gaugler J E, & Mittelman MS (2008). Long-term effects of bereavement and caregiver intervention on dementia caregiver depressive symptoms. The Gerontologist, 48: 732-740. NIHMSID:NIHMS114864.
© Mary Mittelman DrPH and Cynthia Epstein LCSW 2009 12 Implementation Process for the NYUCI
In the sections that follow, we provide guidelines for implementing the NYUCI. It is important to always keep in mind that at the heart of this intervention is an appreciation of the uniqueness of each caregiver and family and the way they respond to the illness. A sensitive clinical approach will reflect your understanding of the issues, strengths and needs of each family. Your skill and humanity, and the relationship you develop with the family will enable you to help them navigate their caregiving journey and bring the manual to life.
Initial Contact Potential participants may already be known to the agency, may be referred by another agency or may respond to brochures and other outreach mechanisms. They may make the initial contact by phone, mail, email or in person. You should record the referral source and method of contact in your records. The main purpose of tracking the many aspects of implementing the intervention is to learn as much as possible about how to most effectively offer the service.
When there is no prior relationship between the caregiver and the counselor, the initial contact sets the stage for the engagement of the participant. The counselor should convey the idea that the intention of the program is to be supportive and be sure that the potential participant understands what is being offered.
The counselor should explain that the program includes individual and family meetings as well as periodic formal evaluations of the participants and of the program itself. Thus, from the start, participation involves a collaboration in which we will be offering services not usually available and in turn, requesting that caregivers provide us with feedback about their experience and whether the program met their needs. We begin with an assessment of eligibility of potential participants and a clear explanation of what will occur.
A candid, approach that is neither defensive nor overly eager, but rather open to questions and concerns may be most effective in helping caregivers to move at their own pace towards a decision about whether to participate in the program. The need to recruit participants should not create a pressure on either the counselor or the caregiver. The description of the program should include the
13 eligibility criteria so that that the listener will know whether he or she qualifies or if the person on whose behalf the inquiry is made will qualify. In all cases the option to receive usual care if the person decides not to participate in the program should be made clear.
I have learned to offer the intervention, and then give an agreed upon amount of time to think about it all for the caregiver. I do not work to get them to sign on the first day we talk about it all. Minnesota Coach
Note: In Minnesota, professionals trained as coaches provided the NYUCI.
The counselor should respond to e-mail or telephone inquiries with an offer to send written informational materials and to discuss the program further in person if after reviewing the information the caregiver is interested and appears to be eligible for the program. An important aspect of this intervention is the supportive relationship with the counselor so the ability to engage in face to face is essential.
One never knows where a referral source may come from! I have had several people come to me through initially contacting me about a caregiver support group. One family was referred by Ag Star, their farm insurance provider. The agent was concerned about caregiver stress and looked up a support group in the area for the caregiver to consider attending. Minnesota Coach
Initial Screening During screening: Explain the purpose of the intervention, focusing on the importance of family involvement. Ask the screening questions (Appendix 2 Screening Tools ), Describe the process of the intervention: An assessment meeting that will last about two hours, 6 counseling sessions (2 individual sessions one prior to the family sessions and one after and four sessions with family members); able to call the counselor at any time for issues or concerns;
14 opportunity to participate in support group; contacts by the caregiver counselor every four months to check in. Assure the caregiver that her/his privacy is important to the project and all information will be private and used for evaluation of the program only.
Eligibility: In order to be eligible for the program, potential participants must be caring for a spouse or partner with Alzheimer’s disease. They must be living together in the community when they enter the program and have at least one family member living in the area who can participate in family meetings. In addition, the caregiver must be emotionally and physically able to participate in sessions. When the demands of caregiving far exceed the ability of the spouse and family to meet them or if serious pathology precedes or is activated by caregiving, treatment beyond the scope of this intervention may be called for and appropriate referrals should be made. Use the screening questionnaire flexibly to determine eligibility. For example, it is not necessary to ask questions if you already know the answers to them. However, fill out the whole screening questionnaire for your records.
I learned through a hard experience that the requirements to participate in this program (family, spouse/partner living with person, no serious persistent mental illness of care partner, diagnosis of AD) are important. I started to work with one woman (before I knew about her mental illness) and the intervention clearly would not have worked for her and her family due to her paranoia and personality disorder. Minnesota Coach
It may be difficult to obtain a formal diagnosis of Alzheimer’s disease in some areas. In order for a caregiver to participate, at minimum a medical determination of chronic dementia should have been made and common alternative causes of the memory problems ruled out. If there has not yet been a diagnostic evaluation, the caregiver should be encouraged to seek a medical evaluation prior to enrollment in the program. This situation may require a case-by-case determination in consultation with the program coordinator.
If they enroll in the program, all caregivers will be expected to invite family members to join in family sessions with them. This is an essential component of the program, not one option among many, and
15 should be explained to the caregiver prior to enrollment. Other referrals and resources may also be offered but family meetings are at the core of the success of this intervention.
I found it helpful to ask these two questions before I spent a lot of time with the caregiver. First I ask, “Are you the primary caregiver of the person with Alzheimer’s?” and then I ask “Would you be the first person called if the person with dementia needed help because of an accident or illness?” If the caregiver answers no to either one, they are not eligible. I save time, by getting clarity on these questions up front. Minnesota Coach In my eagerness to recruit caregivers, I was too quick to sign up anyone who qualified and did not look at the complete picture. I had one caregiver who I was especially eager to work with as he seemed to be falling through the cracks in the service system. The person with Alzheimer's was an alcoholic, but had stopped Drinking. We went through the assessment and one family meeting, and then lost momentum as the spouse resumed Drinking and issues revolved around the alcoholism. This couple was referred for in depth counseling to deal with the alcohol issues and is continuing to receive regular care. This intervention focuses on dementia and people who have more pressing issues may need a different intervention. Minnesota Coach
Informed consent: Before the intake assessment can be implemented the caregiver has to sign HIPPA and informed consent forms. These documents can look intimidating. Their purpose is to clarify the elements of the program, its risks and benefits, describe the information that will be collected and to reassure the participants that their confidentiality will be protected. This should be explained and caregivers should be given copies of the forms for their own records. If potential participants do not want to sign these documents, they cannot participate in this intervention, but can be offered usual care.
Arranging for the initial assessment: There may be a number of details to consider in planning for your meeting with the caregiver. These include the comfort and convenience of the caregiver, the safety of the person with AD and your own availability. Thus, the assessment should be at a time and place that is easiest for all concerned.
16 The Initial Assessment (Counseling the Alzheimer’s Caregiver p31-49) A detailed caregiver assessment is essential. The purpose of the initial assessment is to gather information about the caregiver and his or her family that will help you to understand and be helpful to him or her. By doing the assessment, you will learn about the caregiving environment, the cognitive status of the ill spouse, and problems that require immediate or subsequent attention. Severe depression, for example may require a referral to other services before the caregiver enrolls in the program. The initial assessment also provides the data against which data obtained in follow-up assessments can be compared so that changes in the caregiver can be identified, documented and if necessary, addressed.
The original assessment used by the NYUCI is provided in Appendix 3 Assessment Tools. These scales provide the information needed about the caregiver, the person with Alzheimer’s disease and the family needed to engage in the intervention. Organizations may already have components of this assessment in other assessments tools that they use. For the purpose of the intervention the components needed for documentation of outcomes are the demographic questions, caregiver health, Revised Memory and Problem Behavior Checklist, the Geriatric Depression scale, the Stokes Social Network scale and the Global Deterioration Scale.
The assessment can be conducted in a variety of ways depending on what is most comfortable for the caregiver. Some ways that we have used successfully include reading the assessment with the caregiver or simply asking the questions. Some caregivers may prefer to complete portions of the interview on their own. Some caregivers may even prefer to complete the entire assessment on their own and later discuss it with the counselor.
The sections that are often completed by caregivers alone are: Time Expenditure Caregiver Physical Health Social Support
If the caregiver will complete portions of the assessment her/himself, review the instructions carefully and review the sections to be sure the items are completed appropriately.
17 In order to be helpful to the caregiver and family, the counselor should know whether the person with dementia is in the early, middle or late stage. This is determined by using the Global Deterioration Scale. The stage of the illness is a sensitive issue for many caregivers. Discussion of the meaning of the symptoms during the initial assessment should be handled carefully, with the caregiver’s perspective in mind. It is possible that the counselor will have met the person with dementia previously and so will have first hand information. The person with dementia should not be present at the assessment interview so that the caregiver can speak freely and candidly.
The assessment process can provide some very valuable insight into the caregiver’s thinking as well as opportunities for pertinent education. I was doing the initial assessment with a caregiver and we came to a question about “I feel my spouse is taking advantage of me”. The caregiver mentioned that he was frustrated with his wife in that she would not help him with operating the stove. She looked at it like she had never seen it before, and she had been cooking on it for years. He also asked her to help him learn how to use the timer, and she “would not”. This opened up discussion and education on how the disease affects the brain and that she is not just yanking his chain or trying to make him do things that she is capable of. She really does not remember how to do this any more. Minnesota Coach
First Individual Session (Counseling the Alzheimer’s Caregiver p51-70) The first session has many functions, but its primary purpose is to identify family members who are potential participants in family counseling. It also includes feedback to the caregiver on the assessment and provides an opportunity for clarifying the caregiver’s goals for the sessions. If necessary, the counselor can reinforce the rationale for including additional family members – that they too are affected by the illness and can learn how best to support each other, the spouse caregiver and the person with AD. Family members listed by the caregiver in the Social Network questionnaire are strong candidates to be considered for the subsequent family sessions. The process of selecting and contacting these family members and working out the logistics of the family meetings is an interactive process, with the counselor providing support where needed and working with any reluctance or ambivalence on the part of the caregiver to initiate these contacts. If necessary the counselor can offer to contact some
18 family members on behalf of the caregiver but it is preferable to support the caregiver in reaching out to them him or herself. Family Sessions (Counseling the Alzheimer’s Caregiver p71-98) The family sessions provide a forum for concerned relatives to come together to share their understanding of their relative with AD, and to develop a support system for the caregiving spouse, for the person with AD and for each other. Ideally the same people will attend all four meetings but this may not be possible. Creative use of telephone conferencing and e-mail may serve to link family members who cannot always attend in person or who live too far away to be present. Even those at a distance can lend support, and need support, and can be a part of the support team. In the final family session a plan for ongoing collaboration is established.
These sessions are meant to give participants the experience of working together effectively for the benefit of the family, with deference to the needs and perspective of the spouse (the front line care provider), even when its members are not in complete agreement on all issues other than the stated purpose of the meetings. Based on understanding gained from the initial assessment (which includes the caregiver’s perception of the person with dementia and family dynamics), as well as the individual meeting, the counselor will offer help that builds on the strengths and motivation of the participants.
The process will include: (a) identifying caregiving needs, (b) providing mutual emotional support (c) developing strategies for problem solving, (d) allocating tasks, and (e) maintaining communication.
The content of the session may include: (a) education about Alzheimer’s disease (b) suggestions to enhance caregiving methods (c) resources and referrals. Throughout the session, the counselor will be mindful of the level of tension, anxiety, depression, and mutuality in individuals and in the family as a whole, and intervene accordingly.
19 The first family session: In the first session the counselor will seek to create a safe atmosphere in which family members can share their understanding of Alzheimer’s disease, its impact on their relative, and their vision for mutual support with no fear of ridicule or attack. The family sessions can provide a model for constructive future interactions among family members, if this initial meeting is not progressing satisfactorily, it is essential to immediately address what changes need to be made to ensure a better and more productive experience in the next session.
I have to say I was a bit apprehensive about family sessions, even though I had led so many support groups and parent education groups that I could do it without any trepidation. There is something intimidating in imagining the possibilities that can occur when a family gets together! Minnesota Coach
The content of the first session will also reflect the stage of the person with dementia, the degree of aptitude and experience of the caregivers, and specific caregiving challenges.
Expect a range of emotions from families ...I have witnessed tears to bellyaching laughter in the course of one meeting... They work together on the tough stuff, as well as appreciating the absurd and wonder at what life sends their way. Minnesota Coach
The second and third family meetings If the same people attend all the meetings they may develop a kind of team spirit based on the sharing of their emotional reactions and needs and supported by their efforts to work together. It is not necessary that all participants agree on all the decisions that are made but rather that they bring enough good will to the table to put aside differences in the interest of mutual support. It is to be expected, however, that people may attend only some of the sessions and thus the spouse caregiver, if he or she is able, is the anchor of the sessions and who lives with and has primary responsibility for the care of the person with AD. In the second and third meetings the ability of participants to follow-through on their agreed upon tasks and the reasons they may not have done so, need to be understood, without blame, so that trust in each other can develop. The specific tasks the spouse needs help with will of course depend on the individual situation and may range from gathering information on legal and financial
20 issues, to shopping, staying with the person with AD and talking with the spouse on the phone. Often, the spouse caregiver most desires emotional support, rather than help with specific chores. Thus the meetings address both practical and emotional needs that can enhance the feeling that each family member is not alone. Ideally, the caregiving spouse will feel supported and comforted by the efforts of family members.
The last family session: In the last session the counselor acknowledges the work the family has done, asks family members to share their observations and feelings about what happened in the sessions and what it means to them that this is the last one. If new issues are identified, family members can be encouraged to address them during this session or subsequently on their own, using the strategies they have developed for working together. The goal is to empower the family to continue on its own. The session can conclude by recognizing the progress that has been made, goals still unmet, and encouragement for the future. The counselor should remind participants that ongoing counseling and support is available (ad hoc counseling).
The creativity and resourcefulness of families is exciting to witness. Many have already mapped out emergency plans, and given task assignments. Some of the larger families actually have assigned groups that take care of things. There is the emergency group, the financial management group, etc. One very creative family decided impromptu to have a “funeral Drill” as part of their tasks to accomplish before the next meeting. This of course brought on hilarious laughter, but then turned into an important and practical conversation on where the caregiver had all the vital information located so that the children could find it when needed. At the next family meeting, the caregiver brought along the obituary that they had written for the care receiver, with blank spots for last minute information, and this brought on more conversation about what was important to include. Minnesota Coach
Person with Alzheimer’s Disease Participation in One Session We have agreed that at the discretion of the primary caregiver, if the person with Alzheimer’s disease is in the early stages of the disease and able to participate, he or she can be invited to one session. However it is not appropriate for him/her to attend all sessions. The presence of the person with the disease will in most cases influence the content of the sessions. If they wish to attend more than one session some very sensitive way needs to be found to exclude him or her. Beyond the early stage the
21 needs of the person with the disease may override the needs of other participants and therefore is not encouraged.
Second Individual Session At the conclusion of the family sessions the counselor again meets individually with the spouse caregiver to consolidate the accomplishments of the family meetings, acknowledge issues still outstanding and identify ongoing needs, how to include the family in addressing them, when appropriate, and the ways in which the counselor can continue to lend support. Special attention should be paid to signs of anxiety about this part of the intervention ending, or issues around worries about separation from the counselor. The counselor can reassure the caregiver of his or her ongoing availability through ad hoc counseling (described below), and remind the caregiver that there will be follow-up assessments which can provide opportunity for additional in- person contact. The counselor should encourage the caregiver to join a support group and utilize other supportive resources in the community. (Appendix 4 Individual and Family Session Notes/Logs and Appendix 5 Evaluation Tool)
Ad Hoc Contacts (Counseling the Alzheimer’s Caregiver p99-114) Ad hoc contacts can be made by phone, e-mail, or in person. The spouse caregiver and all family members who have participated in the family sessions should be told that they have the option of contacting the counselor with questions and concerns related to changes in the person with AD, the care of the person with AD, the well-being of the caregiver or family interactions around caregiving and information about community resources. Family members who did not participate in counseling sessions may also call the counselor if they wish. The counselor should let the family members know that as the disease progresses and the cognitive abilities of the person with the disease decline, they are likely to need more information, resources, and support, and that responding to these needs using ad hoc contacts is part of the program. These “as needed” contacts can help families deal with a difficult situation when it arises and anticipate how the progression of the illness will require changes to the care plan. If there has been reluctance to use this service, the counselor can ask the spouse caregiver if it would be acceptable for him/her (the counselor) to initiate contact.
While caregivers and families may not call frequently, we have found that the knowledge that an expert is available is, in itself, very supportive. It is both an emotional and practical safety net. Ad hoc
22 counseling is ideally offered by the counselor who originally worked with the caregiver and family and thus has developed a relationship with them, but in his or her absence another knowledgeable staff member may be able to fill in. The results of the assessments and the counselor’s notes will help remind the original counselor of the caregiving circumstances, and provide information for another counselor who is responding to the call.
It is important that the counselor be mindful of the temptation of family members to use these calls to talk about other family members or to build a special alliance with the counselor and to avoid engaging in such a dialogue.
Because ad hoc counseling is an important component of the NYU Intervention, it is essential that this service be clearly explained early in the program. Families need to know that Ad hoc counseling is available for all family members There is no limit to the number of contacts The counselor will be available to take calls at specific hours or will return them as soon as possible. The protocol requires that all contacts be tracked for frequency and content. This process that can call attention to an increase in contacts that may suggest a potential crisis or that the underlying reason for the calls has not yet emerged and further inquiry is necessary.
“Ad hoc calls tend to occur further into the intervention. There seems to be an “I don’t want to bother you” attitude...Even when caregivers do get into the habit of calling, they still seem to think there is a time limit to obey. If caregivers use email... It works very well to send out notes from family meetings or to send information about local educational programs or family conferences. Sometimes you have to read into things too. I have one caregiver that sends me email regularly. I know that if I have not received any in a week I need to call and check in!” Minnesota Coach
Alzheimer's Caregiver Support Groups (Counseling the Alzheimer’s Caregiver p115-127) The NYU protocol requires the spouse caregiver to participate in a support group after the conclusion of the individual and family counseling component of the intervention (4 months after enrollment). By
23 joining such a group the caregiver can continue to receive emotional support as well as to get practical information from a community resource which includes others who are in a similar situation. Support groups meet on different schedules, ranging from weekly to monthly, and usually are composed of caregivers who have the same relationship to the person with dementia, i.e. spouse, adult child, etc. Some spouses may decide to join support groups at an earlier or later time than is suggested by the protocol. This should be documented in the record. If spouses and other family members are reluctant to join a group, counselors can try to help them work out their issues. However people who continue to feel uncomfortable with the idea of joining a group should not be pressured to join. We have observed that many who were initially unwilling will decide to join a group at a later time.
The First Follow-up Assessment The first follow-up assessment of the spouse caregiver should be scheduled to occur after the individual and family sessions have been completed. It includes the same scales that were in the initial assessment.
According to the protocol, all individual and family sessions should take place within four months of enrollment. On some occasions, travel, illness or other events can interfere, but the first follow-up assessment must occur no later than six months after enrollment. If it has not occurred by then, the first follow-up will be counted as missing, and the next assessment should occur eight months after enrollment.
Going Forward The next phase of the program includes scheduled contact with the caregiver in accordance with the timing of the follow-up assessments, every four months in the first year and every six months thereafter.
A very important thing that you can do is to be available. Just knowing that there is a caring and informed person to reach out to, is an enormous comfort, which may be rarely used but makes a huge difference in the way caregivers feel. We heard this over and over during the course of implementing the NYU spouse program. Of course, for some caregivers who over use this resource, you may have to set some boundaries If people are calling too often, perhaps it is time to recommend additional services.
Cynthia Epstein
24 Assisted Living or Nursing Home Placement (Counseling the Alzheimer’s Caregiver p277-298) Regular assessments and ad hoc contact continue even after the person with AD is placed in an assisted living or nursing home. The date of placement is noted on the caregiver log, and a modified reassessment protocol is implemented according to the regular schedule. See Appendix 6 Placement Tools. This modified tool includes the Cover page, Depression Scale, RMBC, Stokes Social Network Scale and other components that you select to assist your work with the caregiver.
Bereavement: The death of the person with Alzheimer’s disease (Counseling the Alzheimer’s Caregiver p299-323) AD is a terminal disease. That means that the person with dementia will ultimately die from the effects of AD unless he or she dies earlier from some other cause. (Another modified protocol is implemented for two years after the death of the person with dementia See Appendix 6 Bereavement Tools. It is essential that the counselor not assume the way in which the caregiver will be affected or respond to the death but seek to understand the meaning of the event to the caregiver and the family. No matter how much a caregiver may have prepared for life without the person with AD, he or she will have some reaction to the death, which often includes mixed feelings of sadness and relief. Well-meaning people often try to comfort the mourners with sentiments such as “he/she is better off now” which many families find insensitive. Counselors can provide emotional and practical support for caregivers throughout the grieving process, but need to be aware of their own reactions to the death and to keep them separate from those of the family even when they have come to feel almost a part of the family.
Issues to Consider When Undertaking a Translation of the NYUCI Understanding the outcomes The outcomes achieved by the NYUCI have brought it to the attention of many states and funding sources that wish to make these valuable benefits widely available. We share this objective, but would like to offer what may seem a paradoxical caution. Our analysis of the original study data suggests that the family sessions were the catalyst for other outcomes; family members developed ways of providing mutual support for each other and the spouse caregiver felt increased satisfaction with this support of family members.
25 Most spouse caregivers do not want to place their husbands or wives in a nursing home. However, it is not clinically sound, nor do the data substantiate evidence for the interventionist to focus his or her treatment efforts directly towards avoiding nursing home placement. What is important, and backed up by the research, is that if you focus on the building of social support and implement the entire protocol as reliably as possible, then there is a high probability that you will improve the caregiver’s well-being. Caregivers with improved social support will generally experience reduced symptoms of depression and less reactivity to behaviors caused by the illness and better overall physical health, in the absence of other difficult circumstances they will generally be able to utilize resources and cope with the challenges of caregiving for a longer time at home without compromising their wellbeing, and thereby avoid unwanted premature nursing home placement.
Fidelity We understand that no site can replicate or do exactly what was done in New York City as part of a research study. Practical issues in your community may make it necessary to adapt the intervention. The objective of the translation is to strive to remain as close as possible to the original protocol while making adjustments to it as are required by the uniqueness of each setting. These alterations might include changes in the number of sessions, enrolling participants who do not have a formal diagnosis of AD, and adapting to the norms and cultural heritage of the participants. They should be made only after consulting with Dr. Mittelman and documenting the rationale for the change and the approval of the federal Administration on Aging (Appendix 1 Intervention Modification Guide). This process will enhance the relevance of the intervention and provide a living history of its implementation in different settings that can inform future users.
The assessment protocol that was used in the original study may also need to be modified to be more compatible with the procedures in any given setting. However, scales that measure the essential outcomes should be included and any additions, deletions or substitutions should be made in consultation with Dr. Mittelman.
Other considerations The training and clinical approach of the interventionists who will implement this program will probably differ from that of the counselors who originally implemented the research study. Counselors at NYU had varied clinical backgrounds and education, but it is important to note that despite these differences
26 they all achieved similar results. This is likely to be because they all implemented the protocol in the same way and because they all were knowledgeable about Alzheimer’s disease, caregiving, and perhaps most of all, genuinely cared for the families they worked with. Their availability for ongoing counseling and support was mentioned by many participants as being a very real comfort to them.
Data collection and reporting A method of computerized data entry should be put in place before the first participant enrolls. The computer database should include an identifying number for each participant and the date of the assessment. Dates and types of status changes such as dropping out of the study, nursing home placement or death of the person with dementia or caregiver should be included in the database. In addition, the computerized information about individual participants should be accessible to counselors. Regular summary reports of the data should be provided as a routine part of the project, so that progress can be monitored.
27 28