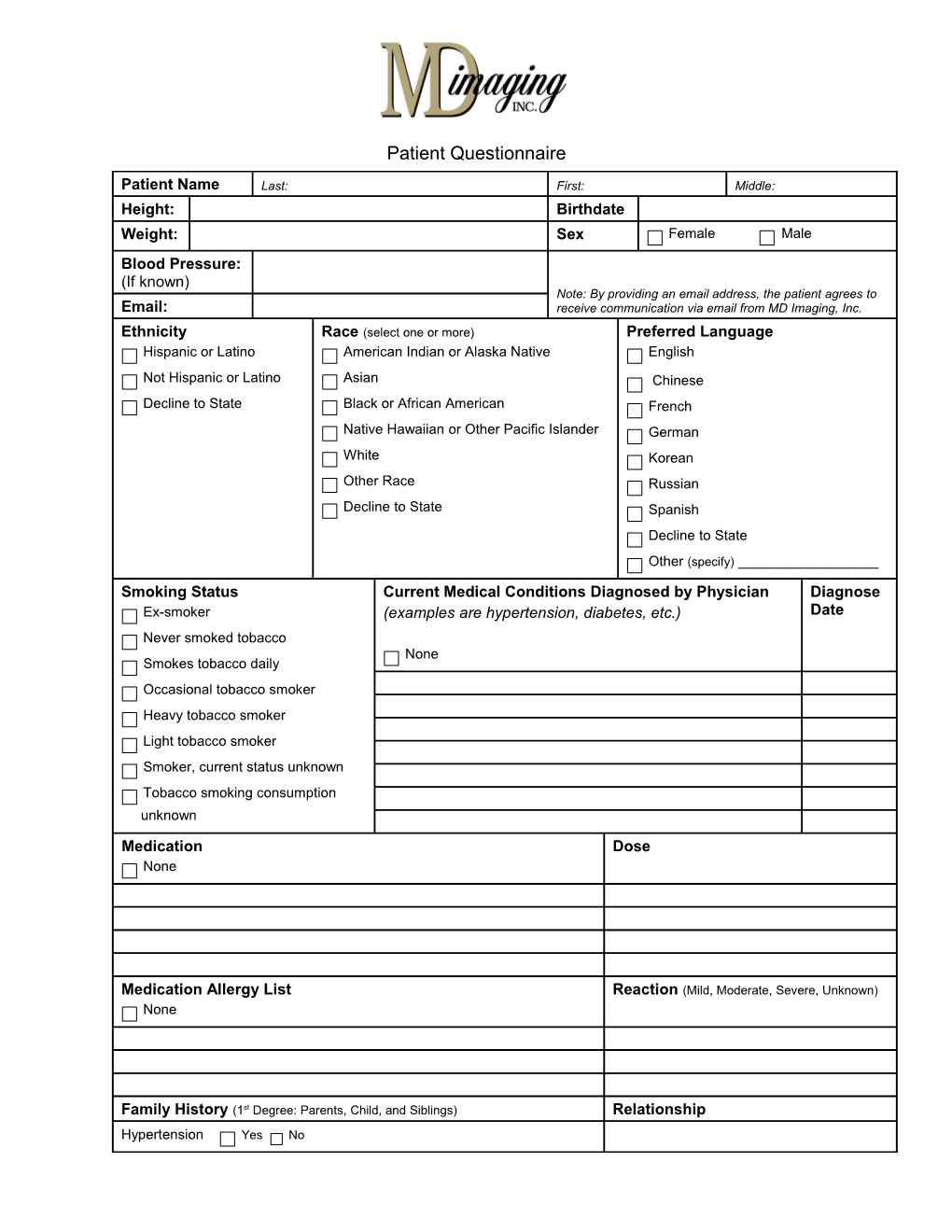
Patient Questionnaire
Patient Name Last: First: Middle: Height: Birthdate Female Male Weight: Sex Blood Pressure: (If known) Note: By providing an email address, the patient agrees to Email: receive communication via email from MD Imaging, Inc. Ethnicity Race (select one or more) Preferred Language Hispanic or Latino American Indian or Alaska Native English Not Hispanic or Latino Asian Chinese Decline to State Black or African American French Native Hawaiian or Other Pacific Islander German White Korean Other Race Russian Decline to State Spanish Decline to State Other (specify) ______Smoking Status Current Medical Conditions Diagnosed by Physician Diagnose Ex-smoker (examples are hypertension, diabetes, etc.) Date Never smoked tobacco None Smokes tobacco daily Occasional tobacco smoker Heavy tobacco smoker Light tobacco smoker Smoker, current status unknown Tobacco smoking consumption unknown
Medication Dose None
Medication Allergy List Reaction (Mild, Moderate, Severe, Unknown) None
Family History (1st Degree: Parents, Child, and Siblings) Relationship Hypertension Yes No Diabetes Yes No
Error! No text of specified style in document.