Report on Communities Interviews
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
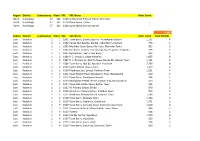
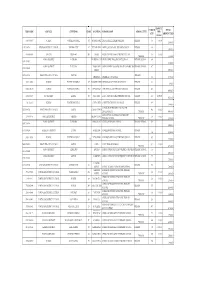
Region District Constituency Ward VRC VRC Name Voter Count North
Region District Constituency Ward VRC VRC Name Voter Count North Koinadugu 47 162 6169 Al-Harrakan Primary School, Woredala - North Koinadugu 47 162 6179 Open Space 2,Kabo - North Koinadugu 47 162 6180 Open Space, Kamayortortor - 9,493 Region District Constituency Ward VRC VRC Name Voter Count Total PS(100) East Kailahun 1 1 1001 Town Barry, Baoma, Baoma - Kunywahun Section 1,192 4 East Kailahun 1 1 1002 Palava Hut, Baoma, Baoma - Gborgborma Section 478 2 East Kailahun 1 1 1003 Mofindor Court Barry, Mofindor, Mofindor Town 835 3 East Kailahun 1 1 1004 Methodist primary school yengema, Yengama, Yengema 629 2 East Kailahun 1 1 1005 Nyanyahun Town, Town Barry 449 2 East Kailahun 1 2 1006 R. C. School 1, Upper Masanta 1,855 6 East Kailahun 1 2 1007 R. C. Primary 11, Gbomo Town, Buedu RD, Gbomo Town 1,121 4 East Kailahun 1 2 1008 Town Barry, Ngitibu, Ngitibu 1-Kailahum 2,209 8 East Kailahun 1 2 1009 KLDEC School, new London 1,259 4 East Kailahun 1 2 1010 Methodist Sec. School, Kailahun Town 1,031 4 East Kailahun 1 2 1011 Town Market Place, Bandajuma Town, Bandajuma 640 2 East Kailahun 1 2 1012 Town Barry, Bandajuma Sinneh 294 1 East Kailahun 1 2 1013 Bandajuma Health Centre, Luawa Foiya, Bandajuma Si 473 2 East Kailahun 1 2 1014 Town Hall, Borbu-Town, Borbu- Town 315 1 East Kailahun 1 2 1015 RC Primary School, Borbu 870 3 East Kailahun 1 2 1016 Amadiyya Primary School, Kailahun Town 973 3 East Kailahun 1 2 1017 Methodist Primary School, kailahun Town 1,266 4 East Kailahun 1 3 1018 Town Barry, Sandialu Town 1,260 4 East Kailahun 1 3 1019 Town -

G U I N E a Liberia Sierra Leone
The boundaries and names shown and the designations Mamou used on this map do not imply official endorsement or er acceptance by the United Nations. Nig K o L le n o G UINEA t l e a SIERRA Kindia LEONEFaranah Médina Dula Falaba Tabili ba o s a g Dubréka K n ie c o r M Musaia Gberia a c S Fotombu Coyah Bafodia t a e r G Kabala Banian Konta Fandié Kamakwie Koinadugu Bendugu Forécariah li Kukuna Kamalu Fadugu Se Bagbe r Madina e Bambaya g Jct. i ies NORTHERN N arc Sc Kurubonla e Karina tl it Mateboi Alikalia L Yombiro Kambia M Pendembu Bumbuna Batkanu a Bendugu b Rokupr o l e Binkolo M Mange Gbinti e Kortimaw Is. Kayima l Mambolo Makeni i Bendou Bodou Port Loko Magburaka Tefeya Yomadu Lunsar Koidu-Sefadu li Masingbi Koundou e a Lungi Pepel S n Int'l Airport or a Matotoka Yengema R el p ok m Freetown a Njaiama Ferry Masiaka Mile 91 P Njaiama- Wellington a Yele Sewafe Tongo Gandorhun o Hastings Yonibana Tungie M Koindu WESTERN Songo Bradford EAS T E R N AREA Waterloo Mongeri York Rotifunk Falla Bomi Kailahun Buedu a i Panguma Moyamba a Taiama Manowa Giehun Bauya T Boajibu Njala Dambara Pendembu Yawri Bendu Banana Is. Bay Mano Lago Bo Segbwema Daru Shenge Sembehun SOUTHE R N Gerihun Plantain Is. Sieromco Mokanje Kenema Tikonko Bumpe a Blama Gbangbatok Sew Tokpombu ro Kpetewoma o Sh Koribundu M erb Nitti ro River a o i Turtle Is. o M h Sumbuya a Sherbro I. -

Sierra Leone Unamsil
13o 30' 13o 00' 12o 30' 12o 00' 11o 30' 11o 00' 10o 30' Mamou The boundaries and names shown and the designations used on this map do not imply ger GUINEA official endorsemenNt ior acceptance by the UNAMSIL K L United Nations. o l o e l n a Deployment as of t e AugustKindia 2005 Faranah o o 10 00' Médina 10 00' National capital Dula Provincial capital Tabili s a Falaba ie ab o c K g Dubréka Town, village r n a o c M S Musaia International boundary t Gberia Coyah a Bafodia UNMO TS-11 e Provincial boundary r Fotombu G Kabala Banian Konta Bendugu 9o 30' Fandié Kamakwie Koinadugu 9o 30' Forécariah Kamalu li Kukuna Fadugu Se s ie agbe c B Madina r r a e c SIERRA LEONE g Jct. e S i tl N Bambaya Lit Ribia Karina Alikalia Kurubonla Mateboi HQ UNAMSIL Kambia M Pendembu Yombiro ab Batkanuo Bendugu l e Bumbuna o UNMO TS-1 o UNMO9 00' HQ Rokupr a 9 00' UNMO TS-4 n Mamuka a NIGERIA 19 Gbinti p Binkolo m Kayima KortimawNIGERIA Is. 19 Mange a Mambolo Makeni P RUSSIA Port Baibunda Loko JORDAN Magburaka Bendou Mape Lungi Tefeya UNMO TS-2 Bodou Lol Rogberi Yomadu UNMO TS-5 Lunsar Matotoka Rokel Bridge Masingbi Koundou Lungi Koidu-Sefadu Pepel Yengema li Njaiama- e Freetown M o 8o 30' Masiaka Sewafe Njaiama 8 30' Goderich Wellington a Yonibana Mile 91 Tungie o Magbuntuso Makite Yele Gandorhun M Koindu Hastings Songo Buedu WESTERN Waterloo Mongeri Falla York Bradford UNMO TS-9 AREA Tongo Giehun Kailahun Tolobo ia Boajibu Rotifunk a T GHANA 11 Taiama Panguma Manowa Banana Is. -

District Summary Bombali
DISTRICT SUMMARY FixingFIXING HEALTH Health POSTS PostsBOMBALITO SAVE toLIVES Save LivesADVANCING PARTNERS & COMMUNITIES, SIERRA LEONE STRENGTHENING REPRODUCTIVE, MATERNAL, NEWBORN, AND CHILD HEALTH SERVICES AS PART OF THE POST-EBOLA TRANSITION JUNE 2017 INTRODUCTION Bombali District’s 111 primary health facilities serve an (284 on government payroll, 255 volunteers). Of these, 78 estimated 606,544 people (Statistics Sierra Leone and are state-enrolled community health nurses (SECHN); 335 Government of Sierra Leone, 2016). The primary health are maternal and child health aides (MCH aides); 16 are facilities include 9 maternal and child health posts (MCHP); community health officers (CHOs); 1 a state-registered 71 community health posts (CHPs); 20 community health nurse (SRN); 87 are regular trained nurses; 8 are community centers (CHCs); and 11 private clinics (faith-based and health assistants (CHA); and 14 are midwives (Ministry of others) (Sierra Leone Ministry of Health and Sanitation, Health and Sanitation, Sierra Leone, Directorate of Human WHO, Service Availability and Readiness Assessment [SARA], Resources for Health). 2017). The services are provided by 539 health care workers Table 1. Volume of Selected Health Services Provided in Bombali, 2016 DELIVERIES ANC4 FULLY IMMUNIZED* MALARIA DIARRHEA CASES TOTAL FP U5 TREATED OPD TREATED PHU COMMUNITY PHU OUT-REACH PHU OUTREACH AT THE PHU WITH ACT 14,838 288 10,049 4,226 12,002 6,556 58,915 139,390 12,012 318,226 * Indicates child has received bacillus Calmette-Guérine, oral poliovirus, all 3 doses of pneumococcal conjugate, pentavalent, rotavirus, measles, and yellow fever vaccines according to schedule. ACT: artemisinin-based combination therapy. ANC4: antenatal care 4th visit. -

Kailahun District Constituencies And
NEC: Report on Electoral Constituency Boundaries Delimitation Process Process Delimitation Boundaries Constituency Electoral on Report NEC: 4.1.1 KAILAHUN DISTRICT CONSTITUENCIES AND POPULATION Eastern Region Constituency Maps 1103 a 43,427 m i a g g n K n e i o s T s T i i i s Penguia s K is is Yawei K K Luawa 1101 e 49,499 r 1104 1108 g n 33,457 54,363 o B Kpeje je e Upper West p K Bambara 1102 44,439 1107 Chiefdom Boundary 37,484 Constituency Code Njaluahun Mandu – 1101 Constituency 1 August 2006 August Dea 1102 Constituency 2 Jawie 1103 Constituency 3 1106 Malema 1104 Constituency 4 42,639 1105 Constituency 5 1105 1106 Constituency 6 52,882 1107 Constituency 7 1108 Constituency 8 42,639 Constituency Population PREPARED BY STATISTICS SIERRA LEONE KENEMA DISTRICT CONSTITUENCIES AND POPULATION Gorama Mende 1207 49,953 Wandor 1206 48,429 n u h Simbaru o g Lower le 1208 Dodo Bambara a M 54,312 1205 42,184 Kandu Leppiama 1204 51,486 1202 1201 42,262 Nongowa 43,308 # Small Bo # Kenema # 1203 1209 Town 42,832 44,045 Dama 1210 Niawa 36341 Gaura Langrama Koya 1211 Nomo 42,796 Chiefdom Boundary Constituency Code Tunkia 1201 Constituency 1 1202 Constituency 2 1203 Constituency 3 1204 Constituency 4 1205 Constituency 5 1206 Constituency 6 1207 Constituency 7 1208 Constituency 8 1209 Constituency 9 1210 Constituency 10 1211 Constituency 11 42,796 Constituency Population PREPARED BY STATISTICS SIERRA LEONE NEC: Report on Electoral Constituency Boundaries Delimitation Process – August 2006 NEC: Report on Electoral Constituency Boundaries Delimitation -
Continuous Results Monitoring and Support System
Continuous Results Monitoring and Support System Bombali/Sierra Leone First Bimonthly Report September 2016 Continuous Results Monitoring and Support System Report—SIAPS/Sierra Leone, September 2016 This report is made possible by the generous support of the American people through the US Agency for International Development (USAID), under the terms of cooperative agreement number AID-OAA-A-11-00021. The contents are the responsibility of Management Sciences for Health and do not necessarily reflect the views of USAID or the United States Government. About SIAPS The goal of the Systems for Improved Access to Pharmaceuticals and Services (SIAPS) Program is to ensure the availability of quality pharmaceutical products and effective pharmaceutical services to achieve desired health outcomes. Toward this end, the SIAPS results areas include improving governance, building capacity for pharmaceutical management and services, addressing information needed for decision-making in the pharmaceutical sector, strengthening financing strategies and mechanisms to improve access to medicines, and increasing quality pharmaceutical services. Recommended Citation This report may be reproduced if credit is given to SIAPS. Please use the following citation. Continuous Results Monitoring and Support System Report Bombali/ Sierra Leone, September 2016. Submitted to the US Agency for International Development by the Systems for Improved Access to Pharmaceuticals and Services (SIAPS) Program. Arlington, VA: Management Sciences for Health. Key Words Sierra Leone, Bombali, Continuous Results Monitoring and Support System (CRMS) Report Systems for Improved Access to Pharmaceuticals and Services Pharmaceuticals and Health Technologies Group Management Sciences for Health 4301 North Fairfax Drive, Suite 400 Arlington, VA 22203 USA Telephone: 703.524.6575 Fax: 703.524.7898 E-mail: [email protected] Website: www.siapsprogram.org ii CONTENTS Acronyms ...................................................................................................................................... -

Rural Transport Survey Report – Batkanu-Makoth
Rural Transport Survey Report Batkanu‐Makoth, Bombali District, Sierra Leone Shamsu Mustapha1, Krijn Peters2 and Nabeela Tunis3 1. Ecofin Consultants, Sierra Leone. 2. Swansea University, UK. 3. Independent Consultant, Sierra Leone. AfCAP/SLE2108A October 2017 Rural Transport Survey Report – Batkanu‐Makoth, Bombali District, Sierra Leone The views in this document are those of the authors and they do not necessarily reflect the views of the Research for Community Access Partnership (ReCAP), or Cardno Emerging Markets (UK) Ltd for whom the document was prepared. Cover Photo: Broken‐down truck on the Batkanu‐Makoth road. This picture and all other pictures in the report by Krijn Peters© Quality assurance and review table Version Author(s) Reviewer(s) Date 1. Mustapha S, Peters K and Tunis, N Nite Tanzarn 09 January 2018 2. AfCAP Database Details: Rural Transport Diagnostic Study in Sierra Leone Reference No: SLE2108A Location Sierra Leone Procurement Source of Proposal ReCAP website Individual Contract Method Rural Transport Rural Transport Survey Report Theme Diagnostic Study in Sierra Sub-Theme for the coastal plains Leone Lead Ecofin Consultants, Sierra Partner Swansea University, UK Implementation Organisation Organisation Leone Total Approved Total Used Budget Budget Start Date End Date Report Due Date Date Received ReCAP Project Management Unit Cardno Emerging Market (UK) Ltd Oxford House, Oxford Road Thame OX9 2AH United Kingdom Page 1 Rural Transport Survey Report – Batkanu‐Makoth, Bombali District, Sierra Leone Abstract This study was carried out in the interior zone in Sierra Leone, focusing on the Batkanu‐ Makoth rural road in Bombali District in the Northern Province. The study sought to understand the existing transport services for the rural communities along and within the road’s catchment area. -

Guinea Liberia
Syke Street Connaught Hospital Ola During EPI Dental Hospital Marie Stopes ĝ EPI Hospital ĝ ĝ PCMH Freetown ĝ ĝ King Harman ĝ Kissy Mental Road Hospital ĝ Hospital 10°N ĝ ĝ Dembelia 34 Military ĝ Hospital ĝ Rokupr Govt. 12.8 km Hospital - Sink ĝ Prisons Hospital Lumley Govt. Hospital Gbindi Bindi 7 km 12.2 km Port Loko 2.2 ĝ km Western Sinkunia Falaba 0.7 km Goderich Heart & Hands Emergency Hospital Folosaba Surgical Hospital Area Dembel Sinkunia Falaba ĝ ĝ Mongo Sierra Leone ĝ Friendship 54.5 km Sulima Lakka 6.8 km Hospital Jui Govt Urban 11 km Hospital Gberia Musaia CHC Wara Wara Timbako Bafod Tambakha 55.1 km Dogoloya 27.1 km 9.5 km 47.7 km Fintonia CHC 15.2 km Bafodia Rural Renewable Energy Project Western Little Scarcies Bafodia Area Guinea Karene Rural Koinadugu 3.6 km 26.1 km Kathantha Yagala Kabala Yimboi CHC Koinadugu Wara Wara 2 CHC 7.4 km Bendugu 54 Community Health Centres Sella Limba Yagal 11.1 km 17.3 km Sengbe Mongo Bendugu (! Kasunko 9°30'N Kamakwie Kamakwie Town Falaba Seria (Work package 1) 15.4 km Bramaia 43.2 km Kamasasa CHC Sanda Loko Bumbuna 2 Moyamba Kukuna CHC Kamalo Great Scarcies (! Kondembaia 41.7 km (! Firawa 6.5 km Fadugu 50 Mini Grids (Work Package 1+) 63.6 km Rokel or Seli Tonko Limba Kamaron 44.6 km Kamaranka CHC Magbaimba Madina Madina Ndorh Junction Gbanti Kamarank Diang Bagbe Biriwa 40 Mini Grids (Work Package 2) 38.7 km Kagbere CHC 30.7 km Gbalamuya CHC 7.7 km Kambia Karina 5.6 km Sanda Sanda Kamabai Alikalia Alikalia 5.7 km Magbolont Tendaran 3.2 (! Kalansogoia Nieni km Kambia 23.5 km 8.1 km Neya Gbinle Kambia Masungbala 19.1 km Gbendembu Pendembu Batkanu CHC Bumbuna 1 Yiffin Dixing Baimoi Munu Sendugu CHC Bendugu 78.5 km Wulalu Magbema 34.9 km Bumbuna Town(! Bumbuna Legend 22.9 km 51.5 km 36.7 km 21.7 km (! Rokupr 24.9 km Kamankay Libeisaygahun !. -

Mission Report – Internship on HHWT
Mission report – Internship on HHWT Aurelie MOY – December 2016 Inter Aide Sierra Leone Executive summary In 2011, Inter Aide Sierra Leone launched a pilot program of Household Water treatment as part of a WASH project in North Bombali district. An internship has been conducted between September 2016 and February 2017 in order to improve the follow-up of the HHWT program with the objective to scale-up its coverage. The main conclusions drawn from this mission are presented in this report, as well as a SWOT1 analysis of the HHWT approach and a hand- over with final recommendations to continue developing the HHWT project. The results of the research part of the mission, as well as the methodology used, are more detailed in the report called HHWT – assessment of acceptance and impact. The functioning of bleach communities and bleach storekeepers is also described precisely in the Report on communities’ interviews and Report on shops’ interviews. 1 Strength / Weaknesses / Opportunities / Threats analysis Mission report – Internship on HHWT Feb 2017 Page 1/37 Contents I] Main conclusions ....................................................................................................................................................... 3 1. Current status of the HHWT project .................................................................................................................... 4 1.1 IA North ........................................................................................................................................................ -
Emis Code Council Chiefdom Ward Location School Name
AMOUNT ENROLM TOTAL EMIS CODE COUNCIL CHIEFDOM WARD LOCATION SCHOOL NAME SCHOOL LEVEL PER ENT AMOUNT PAID CHILD 5103-2-09037 WARDC WATERLOO RURAL 391 ROGBANGBA ABDUL JALIL ACADEMY PRIMARY PRIMARY 369 10,000 3,690,000 1291-2-00714 KENEMA DISTRICT COUNCIL KENEMA CITY 67 FULAWAHUN ABDUL JALIL ISLAMIC PRIMARY SCHOOL PRIMARY 380 3,800,000 4114-2-06856 BO CITY TIKONKO 289 SAMIE ABDUL TAWAB HAIKAL PRIMARY SCHOOL 610 10,000 PRIMARY 6,100,000 KONO DISTRICT TANKORO DOWN BALLOP ABDULAI IBN ABASS PRIMARY SCHOOL PRIMARY SCHOOL 694 1391-2-02007 6,940,000 KONO DISTRICT TANKORO TAMBA ABU ABDULAI IBNU MASSOUD ANSARUL ISLAMIC MISPRIMARY SCHOOL 407 1391-2-02009 STREET 4,070,000 5208-2-10866 FREETOWN CITY COUNCIL WEST III PRIMARY ABERDEEN ABERDEEN MUNICIPAL 366 3,660,000 5103-2-09002 WARDC WATERLOO RURAL 397 KOSSOH TOWN ABIDING GRACE PRIMARY SCHOOL PRIMARY 62 620,000 5103-2-08963 WARDC WATERLOO RURAL 373 BENGUEMA ABNAWEE ISLAMIC PRIMARY SCHOOOL PRIMARY 405 4,050,000 4109-2-06695 BO DISTRICT KAKUA 303 KPETEMA ACEF / MOUNT HORED PRIMARY SCHOOL PRIMARY 411 10,000.00 4,110,000 Not found WARDC WATERLOO RURAL COLE TOWN ACHIEVERS PRIMARY TUTORAGE PRIMARY 388 3,880,000 ACTION FOR CHILDREN AND YOUTH 5205-2-09766 FREETOWN CITY COUNCIL EAST III CALABA TOWN 460 10,000 DEVELOPMENT PRIMARY 4,600,000 ADA GORVIE MEMORIAL PREPARATORY 320401214 BONTHE DISTRICT IMPERRI MORIBA TOWN 320 10,000 PRIMARY SCHOOL PRIMARY 3,200,000 KONO DISTRICT TANKORO BONGALOW ADULLAM PRIMARY SCHOOL PRIMARY SCHOOL 323 1391-2-01954 3,230,000 1109-2-00266 KAILAHUN DISTRICT LUAWA KAILAHUN ADULLAM PRIMARY -

The Chiefdoms of Sierra Leone
The Chiefdoms of Sierra Leone Tristan Reed1 James A. Robinson2 July 15, 2013 1Harvard University, Department of Economics, Littauer Center, 1805 Cambridge Street, Cambridge MA 02138; E-mail: [email protected]. 2Harvard University, Department of Government, IQSS, 1737 Cambridge Street., N309, Cambridge MA 02138; E-mail: [email protected]. Abstract1 In this manuscript, a companion to Acemoglu, Reed and Robinson (2013), we provide a detailed history of Paramount Chieftaincies of Sierra Leone. British colonialism transformed society in the country in 1896 by empowering a set of Paramount Chiefs as the sole authority of local government in the newly created Sierra Leone Protectorate. Only individuals from the designated \ruling families" of a chieftaincy are eligible to become Paramount Chiefs. In 2011, we conducted a survey in of \encyclopedias" (the name given in Sierra Leone to elders who preserve the oral history of the chieftaincy) and the elders in all of the ruling families of all 149 chieftaincies. Contemporary chiefs are current up to May 2011. We used the survey to re- construct the history of the chieftaincy, and each family for as far back as our informants could recall. We then used archives of the Sierra Leone National Archive at Fourah Bay College, as well as Provincial Secretary archives in Kenema, the National Archives in London and available secondary sources to cross-check the results of our survey whenever possible. We are the first to our knowledge to have constructed a comprehensive history of the chieftaincy in Sierra Leone. 1Oral history surveys were conducted by Mohammed C. Bah, Alimamy Bangura, Alieu K. -

Sierra Leone Recovery Strategy for Newly Accessible Areas
Sierra Leone Recovery Strategy for Newly Accessible Areas National Recovery Committee May 2002 Table of Contents GLOSSARY OF ABBREVIATIONS ................................................................................ 4 EXECUTIVE SUMMARY ................................................................................................ 6 1. INTRODUCTION ........................................................................................................ 12 1.1. The National Recovery Structure........................................................................... 12 1.2. A bottom-up approach emphasising local consultations ....................................... 12 1.3. A recovery strategy to promote stability................................................................ 13 2. RESTORATION OF CIVIL AUTHORITY................................................................. 14 2.1. District Administration .......................................................................................... 15 2.2. District Councils .................................................................................................... 16 2.3. Sierra Leone Police................................................................................................ 17 2.4. Courts..................................................................................................................... 19 2.5. Prisons.................................................................................................................... 20 2.6. Paramount Chiefs and Chiefdom