Acinetobacter Baumannii
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Pneumonia Types
Pneumonia Jodi Grandominico , MD Assistant Professor of Clinical Medicine Department of Internal Medicine Division of General Medicine and Geriatrics The Ohio State University Wexner Medical Center Pneumonia types • CAP- limited or no contact with health care institutions or settings • HAP: hospital-acquired pneumonia – occurs 48 hours or more after admission • VAP: ventilator-associated pneumonia – develops more than 48 to 72 hours after endotracheal intubation • HCAP: healthcare-associated pneumonia – occurs in non-hospitalized patient with extensive healthcare contact 2005 IDSA/ATS HAP, VAP and HCAP Guidelines Am J Respir Crit Care Med 2005; 171:388–416 1 Objectives-CAP • Epidemiology • Review cases: ‒ Diagnostic techniques ‒ Risk stratification for site of care decisions ‒ Use of biomarkers ‒ Type and length of treatment • Prevention Pneumonia Sarah Tapyrik, MD Assistant Professor – Clinical Division of Pulmonary, Allergy, Critical Care and Sleep Medicine The Ohio State University Wexner Medical Center 2 Epidemiology American lung association epidemiology and statistics unit research and health education division. November 2015 3 Who is at Risk? • Children <5 yo • Immunosuppressed: • Adults >65 yo ‒ HIV • Comorbid conditions: ‒ Cancer ‒ CKD ‒ Splenectomy ‒ CHF • Cigarette Smokers ‒ DM • Alcoholics ‒ Chronic Liver Disease ‒ COPD Clinical Presentation • Fever • Elderly and • Chills Immunocompromised • Cough w/ purulent ‒ Confusion sputum ‒ Lethargy • Dyspnea ‒ Poor PO intake • Pleuritic pain ‒ Falls • Night sweats ‒ Decompensation of -
Infrastructure for a Phage Reference Database: Identification of Large-Scale Biases in The
bioRxiv preprint doi: https://doi.org/10.1101/2021.05.01.442102; this version posted May 1, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. 1 INfrastructure for a PHAge REference Database: Identification of large-scale biases in the 2 current collection of phage genomes 3 4 Ryan Cook1, Nathan Brown2, Tamsin Redgwell3, Branko Rihtman4, Megan Barnes2, Martha 5 Clokie2, Dov J. Stekel5, Jon Hobman5, Michael A. Jones1, Andrew Millard2* 6 7 1 School of Veterinary Medicine and Science, University of Nottingham, Sutton Bonington 8 Campus, College Road, Loughborough, Leicestershire, LE12 5RD, UK 9 2 Dept Genetics and Genome Biology, University of Leicester, University Road, Leicester, 10 Leicestershire, LE1 7RH, UK 11 3 COPSAC, Copenhagen Prospective Studies on Asthma in Childhood, Herlev and Gentofte 12 Hospital, University of Copenhagen, Copenhagen, Denmark 13 4 University of Warwick, School of Life Sciences, Coventry, UK 14 5 School of Biosciences, University of Nottingham, Sutton Bonington Campus, College Road, 15 Loughborough, Leicestershire, LE12 5RD, 16 17 Corresponding author: [email protected] bioRxiv preprint doi: https://doi.org/10.1101/2021.05.01.442102; this version posted May 1, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC 4.0 International license. -

Acinetobacter Baumannii Resistance: a Real Challenge for Clinicians
antibiotics Review Acinetobacter baumannii Resistance: A Real Challenge for Clinicians Rosalino Vázquez-López 1,* , Sandra Georgina Solano-Gálvez 2, Juan José Juárez Vignon-Whaley 1 , Jorge Andrés Abello Vaamonde 1 , Luis Andrés Padró Alonzo 1, Andrés Rivera Reséndiz 1, Mauricio Muleiro Álvarez 1, Eunice Nabil Vega López 3, Giorgio Franyuti-Kelly 3 , Diego Abelardo Álvarez-Hernández 1 , Valentina Moncaleano Guzmán 1, Jorge Ernesto Juárez Bañuelos 1, José Marcos Felix 4, Juan Antonio González Barrios 5 and Tomás Barrientos Fortes 6 1 Departamento de Microbiología del Centro de Investigación en Ciencias de la Salud (CICSA), FCS, Universidad Anáhuac México Norte, Huixquilucan 52786, Mexico; [email protected] (J.J.J.V.-W.); [email protected] (J.A.A.V.); [email protected] (L.A.P.A.); [email protected] (A.R.R.); [email protected] (M.M.Á.); [email protected] (D.A.Á.-H.); [email protected] (V.M.G.); [email protected] (J.E.J.B.) 2 Departamento de Microbiología y Parasitología, Facultad de Medicina, Universidad Nacional Autónoma de México, Ciudad de Mexico 04510, Mexico; [email protected] 3 Medical IMPACT, Infectious Diseases Department, Mexico City 53900, Mexico; [email protected] (E.N.V.L.); [email protected] (G.F.-K.) 4 Coordinación Ciclos Clínicos Medicina, FCS, Universidad Anáhuac México Norte, Huixquilucan 52786, Mexico; [email protected] 5 Laboratorio de Medicina Genómica, Hospital Regional “1º de Octubre”, ISSSTE, Av. Instituto Politécnico Nacional 1669, Lindavista, Gustavo A. Madero, Ciudad de Mexico 07300, Mexico; [email protected] 6 Dirección Sistema Universitario de Salud de la Universidad Anáhuac México (SUSA), Huixquilucan 52786, Mexico; [email protected] * Correspondence: [email protected] or [email protected]; Tel.: +52-56-270210 (ext. -

Detection of ESKAPE Pathogens and Clostridioides Difficile in Simulated
bioRxiv preprint doi: https://doi.org/10.1101/2021.03.04.433847; this version posted March 4, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 1 Detection of ESKAPE pathogens and Clostridioides difficile in 2 Simulated Skin Transmission Events with Metagenomic and 3 Metatranscriptomic Sequencing 4 5 Krista L. Ternusa#, Nicolette C. Keplingera, Anthony D. Kappella, Gene D. Godboldb, Veena 6 Palsikara, Carlos A. Acevedoa, Katharina L. Webera, Danielle S. LeSassiera, Kathleen Q. 7 Schultea, Nicole M. Westfalla, and F. Curtis Hewitta 8 9 aSignature Science, LLC, 8329 North Mopac Expressway, Austin, Texas, USA 10 bSignature Science, LLC, 1670 Discovery Drive, Charlottesville, VA, USA 11 12 #Address correspondence to Krista L. Ternus, [email protected] 13 14 1 bioRxiv preprint doi: https://doi.org/10.1101/2021.03.04.433847; this version posted March 4, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 15 1 Abstract 16 Background: Antimicrobial resistance is a significant global threat, posing major public health 17 risks and economic costs to healthcare systems. Bacterial cultures are typically used to diagnose 18 healthcare-acquired infections (HAI); however, culture-dependent methods provide limited 19 presence/absence information and are not applicable to all pathogens. -

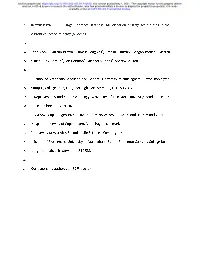
Carbapenem-Resistant Acinetobacter Threat Level Urgent
CARBAPENEM-RESISTANT ACINETOBACTER THREAT LEVEL URGENT 8,500 700 $281M Estimated cases Estimated Estimated attributable in hospitalized deaths in 2017 healthcare costs in 2017 patients in 2017 Acinetobacter bacteria can survive a long time on surfaces. Nearly all carbapenem-resistant Acinetobacter infections happen in patients who recently received care in a healthcare facility. WHAT YOU NEED TO KNOW CASES OVER TIME ■ Carbapenem-resistant Acinetobacter cause pneumonia Continued infection control and appropriate antibiotic use and wound, bloodstream, and urinary tract infections. are important to maintain decreases in carbapenem-resistant These infections tend to occur in patients in intensive Acinetobacter infections. care units. ■ Carbapenem-resistant Acinetobacter can carry mobile genetic elements that are easily shared between bacteria. Some can make a carbapenemase enzyme, which makes carbapenem antibiotics ineffective and rapidly spreads resistance that destroys these important drugs. ■ Some Acinetobacter are resistant to nearly all antibiotics and few new drugs are in development. CARBAPENEM-RESISTANT ACINETOBACTER A THREAT IN HEALTHCARE TREATMENT OVER TIME Acinetobacter is a challenging threat to hospitalized Treatment options for infections caused by carbapenem- patients because it frequently contaminates healthcare resistant Acinetobacter baumannii are extremely limited. facility surfaces and shared medical equipment. If not There are few new drugs in development. addressed through infection control measures, including rigorous -

Acinetobacter Baumannii Biofilm Formation
Structural basis for Acinetobacter baumannii biofilm formation Natalia Pakharukovaa, Minna Tuittilaa, Sari Paavilainena, Henri Malmia, Olena Parilovaa, Susann Tenebergb, Stefan D. Knightc, and Anton V. Zavialova,1 aDepartment of Chemistry, University of Turku, Joint Biotechnology Laboratory, Arcanum, 20500 Turku, Finland; bInstitute of Biomedicine, Department of Medical Biochemistry and Cell Biology, The Sahlgrenska Academy, University of Gothenburg, 40530 Göteborg, Sweden; and cDepartment of Cell and Molecular Biology, Biomedical Centre, Uppsala University, 75124 Uppsala, Sweden Edited by Scott J. Hultgren, Washington University School of Medicine, St. Louis, MO, and approved April 11, 2018 (received for review January 19, 2018) Acinetobacter baumannii—a leading cause of nosocomial infec- donor sequence, this subunit is predicted to contain an additional tions—has a remarkable capacity to persist in hospital environ- domain (7). This implies that CsuE is located at the pilus tip. Since ments and medical devices due to its ability to form biofilms. many two-domain tip subunits in classical systems have been Biofilm formation is mediated by Csu pili, assembled via the “ar- shown to act as host cell binding adhesins (TDAs) (13–16), CsuE chaic” chaperone–usher pathway. The X-ray structure of the CsuC- could also play a role in bacterial attachment to biotic and abiotic CsuE chaperone–adhesin preassembly complex reveals the basis substrates. However, adhesion properties of Csu subunits are not for bacterial attachment to abiotic surfaces. CsuE exposes three known, and the mechanism of archaic pili-mediated biofilm for- hydrophobic finger-like loops at the tip of the pilus. Decreasing mation remains enigmatic. Here, we report the crystal structure of the hydrophobicity of these abolishes bacterial attachment, sug- the CsuE subunit complexed with the CsuC chaperone. -

Section 4. Guidance Document on Horizontal Gene Transfer Between Bacteria
306 - PART 2. DOCUMENTS ON MICRO-ORGANISMS Section 4. Guidance document on horizontal gene transfer between bacteria 1. Introduction Horizontal gene transfer (HGT) 1 refers to the stable transfer of genetic material from one organism to another without reproduction. The significance of horizontal gene transfer was first recognised when evidence was found for ‘infectious heredity’ of multiple antibiotic resistance to pathogens (Watanabe, 1963). The assumed importance of HGT has changed several times (Doolittle et al., 2003) but there is general agreement now that HGT is a major, if not the dominant, force in bacterial evolution. Massive gene exchanges in completely sequenced genomes were discovered by deviant composition, anomalous phylogenetic distribution, great similarity of genes from distantly related species, and incongruent phylogenetic trees (Ochman et al., 2000; Koonin et al., 2001; Jain et al., 2002; Doolittle et al., 2003; Kurland et al., 2003; Philippe and Douady, 2003). There is also much evidence now for HGT by mobile genetic elements (MGEs) being an ongoing process that plays a primary role in the ecological adaptation of prokaryotes. Well documented is the example of the dissemination of antibiotic resistance genes by HGT that allowed bacterial populations to rapidly adapt to a strong selective pressure by agronomically and medically used antibiotics (Tschäpe, 1994; Witte, 1998; Mazel and Davies, 1999). MGEs shape bacterial genomes, promote intra-species variability and distribute genes between distantly related bacterial genera. Horizontal gene transfer (HGT) between bacteria is driven by three major processes: transformation (the uptake of free DNA), transduction (gene transfer mediated by bacteriophages) and conjugation (gene transfer by means of plasmids or conjugative and integrated elements). -

ESKAPE Pathogens in Animals and Their Antimicrobial Drug Resistance Pattern
Journal of Dairy & Veterinary Sciences ISSN: 2573-2196 Research Article Dairy and Vet Sci J Volume 7 Issue 3 - August 2018 Copyright © All rights are reserved by Bhoj R Singh DOI: 10.19080/JDVS.2018.07.555715 ESKAPE Pathogens in Animals and their Antimicrobial Drug Resistance Pattern Bhoj R Singh* Division of Epidemiology, ICAR-Indian Veterinary Research Institute, India Submission: July 27, 2018; Published: August 24, 2018 *Corresponding author: Bhoj R Singh, Head, Division of Epidemiology, ICAR-Indian Veterinary Research Institute, Izatnagar-243122, Bareilly, UP, India. Phone: +91-8449033222, Email: Abstract The analytical study, of 3240 bacterial isolates from veterinary clinical cases and related sources since 2011 to 2017, aimed to understand the extent of infections in animals associated with ESKAPE group (439) of pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter species) and to map their antimicrobial sensitivity pattern. All the six ESKAPE pathogens caused infection in animals, the most common being Enterobacter species followed by K. pneumoniae, P. aeruginosa S. aureus, E. faecium and A. baumannii. None of the antibiotics was effective on all the ESKAPE bacterial isolates however, carbapenems (80.4%), tigecycline (76.8%), chloramphenicol (75.8%) and cefepimes (74.6%) inhibited majority of the isolates. More than 76% ESKAPE bacteria had E. faceium (87.5%) and P. aeruginosa multiple drug resistance (MDR), significantly (p, <=0.05) more P. aeruginosa common isolates in but cinnamaldehyde could inhibit (94.5%)almost 98% isolates. of P. aeruginosaMetallo-β- andlactamase >90% (MBL)isolates and of otherextended ESKAPE spectrum-β-lactamase bacteria (except E. (ESBL)faecium production). -

High Prevalence of Carbapenemase-Producing Acinetobacter Baumannii in Wound Infections, Ghana, 2017/2018
microorganisms Communication High Prevalence of Carbapenemase-Producing Acinetobacter baumannii in Wound Infections, Ghana, 2017/2018 Mathieu Monnheimer 1 , Paul Cooper 2, Harold K. Amegbletor 2, Theresia Pellio 2, Uwe Groß 1, Yvonne Pfeifer 3,† and Marco H. Schulze 1,4,*,† 1 Institute for Medical Microbiology and Göttingen International Health Network, University Medical Center Göttingen, Kreuzbergring 57, 37075 Göttingen, Germany; [email protected] (M.M.); [email protected] (U.G.) 2 St. Martin de Porres Hospital, Post Office Box 06, Eikwe via Axim, Ghana; cpaulkofi@yahoo.co.uk (P.C.); [email protected] (H.K.A.); [email protected] (T.P.) 3 Nosocomial Pathogens and Antibiotic Resistance, Robert Koch Institute, Burgstrasse 37, 38855 Wernigerode, Germany; [email protected] 4 Institute of Infection Control and Infectious Diseases, University Medical Centre Göttingen, Robert-Koch-Strasse 40, 37075 Göttingen, Germany * Correspondence: [email protected]; Tel.: +49-551-39-62286; Fax: +49-551-39-62093 † These authors contributed equally to this work. Abstract: Three years after a prospective study on wound infections in a rural hospital in Ghana revealed no emergence of carbapenem-resistant bacteria we initiated a new study to assess the prevalence of multidrug-resistant pathogens. Three hundred and one samples of patients with wound infections were analysed for the presence of resistant bacteria in the period August 2017 Citation: Monnheimer, M.; Cooper, till March 2018. Carbapenem-resistant Acinetobacter (A.) baumannii were further characterized by P.; Amegbletor, H.K.; Pellio, T.; Groß, resistance gene sequencing, PCR-based bacterial strain typing, pulsed-field gel electrophoresis (PFGE) U.; Pfeifer, Y.; Schulze, M.H. -

Acinetobacter Pollinis Sp
TAXONOMIC DESCRIPTION Alvarez- Perez et al., Int. J. Syst. Evol. Microbiol. 2021;71:004783 DOI 10.1099/ijsem.0.004783 Acinetobacter pollinis sp. nov., Acinetobacter baretiae sp. nov. and Acinetobacter rathckeae sp. nov., isolated from floral nectar and honey bees Sergio Alvarez- Perez1,2†, Lydia J. Baker3†, Megan M. Morris4, Kaoru Tsuji5, Vivianna A. Sanchez3, Tadashi Fukami6, Rachel L. Vannette7, Bart Lievens1 and Tory A. Hendry3,* Abstract A detailed evaluation of eight bacterial isolates from floral nectar and animal visitors to flowers shows evidence that they rep- resent three novel species in the genus Acinetobacter. Phylogenomic analysis shows the closest relatives of these new isolates are Acinetobacter apis, Acinetobacter boissieri and Acinetobacter nectaris, previously described species associated with floral nectar and bees, but high genome- wide sequence divergence defines these isolates as novel species. Pairwise comparisons of the average nucleotide identity of the new isolates compared to known species is extremely low (<83 %), thus confirming that these samples are representative of three novel Acinetobacter species, for which the names Acinetobacter pollinis sp. nov., Aci- netobacter baretiae sp. nov. and Acinetobacter rathckeae sp. nov. are proposed. The respective type strains are SCC477T (=TSD- 214T=LMG 31655T), B10AT (=TSD-213T=LMG 31702T) and EC24T (=TSD-215T=LMG 31703T=DSM 111781T). The genus Acinetobacter (Gammaproteobacteria) is a physi- gene trees, but was nevertheless identified and described as ologically and metabolically diverse group of bacteria cur- a new species with the name Acinetobacter apis. However, rently including 65 validly published and correct names, plus several other tentative designations and effectively but not the diversity of acinetobacters associated with flowering validly published species names (https:// lpsn. -

Characterization of Bacterial Communities Associated
www.nature.com/scientificreports OPEN Characterization of bacterial communities associated with blood‑fed and starved tropical bed bugs, Cimex hemipterus (F.) (Hemiptera): a high throughput metabarcoding analysis Li Lim & Abdul Hafz Ab Majid* With the development of new metagenomic techniques, the microbial community structure of common bed bugs, Cimex lectularius, is well‑studied, while information regarding the constituents of the bacterial communities associated with tropical bed bugs, Cimex hemipterus, is lacking. In this study, the bacteria communities in the blood‑fed and starved tropical bed bugs were analysed and characterized by amplifying the v3‑v4 hypervariable region of the 16S rRNA gene region, followed by MiSeq Illumina sequencing. Across all samples, Proteobacteria made up more than 99% of the microbial community. An alpha‑proteobacterium Wolbachia and gamma‑proteobacterium, including Dickeya chrysanthemi and Pseudomonas, were the dominant OTUs at the genus level. Although the dominant OTUs of bacterial communities of blood‑fed and starved bed bugs were the same, bacterial genera present in lower numbers were varied. The bacteria load in starved bed bugs was also higher than blood‑fed bed bugs. Cimex hemipterus Fabricus (Hemiptera), also known as tropical bed bugs, is an obligate blood-feeding insect throughout their entire developmental cycle, has made a recent resurgence probably due to increased worldwide travel, climate change, and resistance to insecticides1–3. Distribution of tropical bed bugs is inclined to tropical regions, and infestation usually occurs in human dwellings such as dormitories and hotels 1,2. Bed bugs are a nuisance pest to humans as people that are bitten by this insect may experience allergic reactions, iron defciency, and secondary bacterial infection from bite sores4,5. -

Pseudomonas Aeruginosa: an Audacious Pathogen with an Adaptable Arsenal of Virulence Factors
International Journal of Molecular Sciences Review Pseudomonas aeruginosa: An Audacious Pathogen with an Adaptable Arsenal of Virulence Factors Irene Jurado-Martín † , Maite Sainz-Mejías † and Siobhán McClean * School of Biomolecular and Biomedical Sciences, University College Dublin, Belfield, Dublin 4 D04 V1W8, Ireland; [email protected] (I.J.-M.); [email protected] (M.S.-M.) * Correspondence: [email protected] † These authors contributed equally to this review. Abstract: Pseudomonas aeruginosa is a dominant pathogen in people with cystic fibrosis (CF) contribut- ing to morbidity and mortality. Its tremendous ability to adapt greatly facilitates its capacity to cause chronic infections. The adaptability and flexibility of the pathogen are afforded by the extensive number of virulence factors it has at its disposal, providing P. aeruginosa with the facility to tailor its response against the different stressors in the environment. A deep understanding of these virulence mechanisms is crucial for the design of therapeutic strategies and vaccines against this multi-resistant pathogen. Therefore, this review describes the main virulence factors of P. aeruginosa and the adap- tations it undergoes to persist in hostile environments such as the CF respiratory tract. The very large P. aeruginosa genome (5 to 7 MB) contributes considerably to its adaptive capacity; consequently, genomic studies have provided significant insights into elucidating P. aeruginosa evolution and its interactions with the host throughout the course of infection. Citation: Jurado-Martín, I.; Keywords: Pseudomonas aeruginosa; virulence factors; adaptation; cystic fibrosis; diversity; genomics; Sainz-Mejías, M.; McClean, S. lung environment Pseudomonas aeruginosa: An Audacious Pathogen with an Adaptable Arsenal of Virulence Factors.