Pharmacy Auditing and Dispensing Job Aid: Billing Other Dosage Forms
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Inhalation Devices: Various Forms of Administration for Therapeutic Optimization
vv ISSN: 2640-8082 DOI: https://dx.doi.org/10.17352/oja CLINICAL GROUP Renata Cristina de Angelo Calsaverini Leal* Review Article Santa Fé do Sul Foundation of Education and Culture, Brazil Inhalation Devices: Various forms Dates: Received: 31 May, 2017; Accepted: 26 June, of administration for Therapeutic 2017; Published: 27 June, 2017 *Corresponding author: Renata Cristina de Angelo Optimization Calsaverini Leal, Santa Fé do Sul Foundation of Education and Culture, Brazil, Tel: 55 (17) 3272-2769, E-mail: Keywords: Inhalation; Aerosol; Nebulizer Summary https://www.peertechz.com Introduction: Aerosol therapy consists of spraying liquid particles suspended for therapeutic purposes in the respiratory tract. With direct absorption and deposition at the lung level, avoiding side effects and presenting fast response time. Several factors infl uence the drug action, such as size, particle movement, ventilatory fl ow, pulmonary expansion, anatomy, respiratory mechanics and the nebulizer and patient interface. The therapeutic optimization depends on the type of nebulizer differentiating itself by the physical principle that generates the mist. Objectives: Check advantages and disadvantages of different inhalation devices. Methodology. This is a review of the PubMed database using descriptors: ultrasonic and jet nebulizer, aerosol deposition in the lung, metered dose inhaler and dry, inhaler therapy. Results: Different devices are mentioned in the literature: pneumatic and ultrasonic nebulizers (administering solutions), metered pressurized inhalers - pMDI used with or without expander chamber (administering suspensions) and dry powder inhalers - DPI (administering powder). Discussion and Conclusion: The US has advantages: quiet, does not require coordinating abilities, without propellant gases and quick nebulization with small amount of solution. Disadvantages: change in the active principle of thermosensitive drugs, deposition in the oropharynx and VAI of 2% of inhaled particles. -

Ophthalmic Adverse Effects of Nasal Decongestants on an Experimental
A RQUIVOS B RASILEIROS DE ORIGINAL ARTICLE Ophthalmic adverse effects of nasal decongestants on an experimental rat model Efeitos oftálmicos adversos de descongestionantes nasais em modelo experimental com ratos Ayse Ipek Akyuz Unsal1, Yesim Basal2, Serap Birincioglu3, Tolga Kocaturk1, Harun Cakmak1, Alparslan Unsal4, Gizem Cakiroz5, Nüket Eliyatkın6, Ozden Yukselen7, Buket Demirci5 1. Department of Ophthalmology, Medical Faculty, Adnan Menderes University, Aydin, Turkey. 2. Department of Otorhinolaringology, Medical Faculty, Adnan Menderes University, Aydin, Turkey. 3. Department of Pathology, Veterinary Faculty, Adnan Menderes University, Aydin, Turkey. 4. Department of Radiology, Medical Faculty, Adnan Menderes University, Aydin, Turkey. 5. Department of Medical Pharmacology, Medical Faculty, Adnan Menderes University, Aydin, Turkey. 6. Department of Medical Pathology, Medical Faculty, Adnan Menderes University, Aydin, Turkey. 7. Department of Pathology, Aydin State Hospital, Aydin, Turkey. ABSTRACT | Purpose: To investigate the potential effects of cause ophthalmic problems such as dry eyes, corneal edema, chronic exposure to a nasal decongestant and its excipients cataracts, retinal nerve fiber layer, and vascular damage in on ocular tissues using an experimental rat model. Methods: rats. Although these results were obtained from experimental Sixty adult male Wistar rats were randomized into six groups. animals, ophthalmologists should keep in mind the potential The first two groups were control (serum physiologic) and ophthalmic adverse effects of this medicine and/or its excipients Otrivine® groups. The remaining four groups received the and exercise caution with drugs containing xylometazoline, Otrivine excipients xylometazoline, benzalkonium chloride, ethylene diamine tetra acetic acid, benzalkonium chloride and sorbitol, and ethylene diamine tetra acetic acid. Medications sorbitol for patients with underlying ocular problems. -

Inhaled Steroids in Asthma a Patient's Guide
I I v v v v d v v Patient advice and liaison service (PALS) Actions r v If you have a compliment, complaint or It is sensible to ensure you make the r concern please contact our PALS team on following steps now you have a new r 020 7288 5551 or inhaler d [email protected] d d Pick up our guide on inhalers and If you need a large print, audio or spacers to complement this leaflet translated copy of this leaflet please Inhaled Steroids in Agree on a personalised asthma contact us on 020 7288 3182. We will try plan (this is done with your doctor or our best to meet your needs. Asthma nurse and usually written down for future reference) Remember to take your medicines A patient’s guide as advised Should your inhalers fail to relieve your symptoms, go straight to Accident and Emergency Need Help? Whittington Paediatric Asthma Nurse Tel: 020 7288 5527 Whittington Health Community Nurse Magdala Avenue Islington 020 3316 1950 (8am-6pm) London N19 5NF Haringey 020 8887 3301 (9am – 5pm) Phone: 020 7272 3070 www.whittington.nhs.uk Asthma UK 0300 222 5800 Date published: 25/09/2018 www.asthma.org.uk Review date: 25/09/2020 Ref: C&YP/Paed/ISA/03 © Whittington Health Please recycle Tel: 020 7272 3070 Asthma There are many types of preventer Side Effects Asthma is a common condition affecting inhaler. There are simple steroids like Parents worry about children and young the airway. Usually a trigger (such as dust beclomethasone, and then there are also adults taking inhaled steroids because of or pollen) irritates the airways which combined inhalers, called seretide or side effects they’ve heard about. -

Member List 2016
To help make the use of prescription drugs safer and more affordable, our plan is now using a Drug Quantity Management program. That is, for certain medications, you can receive an amount to last you a certain number of days. This gives you the right amount to take the daily dose considered safe and effective, according to the recommendations of the U.S. Food and Drug Administration (FDA). Based on the FDA’s guidelines and other medical information, our plan developed this program together with Express Scripts, the company chosen to manage our prescription drug benefit. The following limits are based on a 30-day supply. If your plan allows for additional days supply, your limits may be higher. For instance, you may be able to get a 90-day supply of your medication through mail order service. Your doctor could also request a prior authorization. If this request is approved, a prior authorization would let you receive more than the recommended quantity. Drug Target Maximum Quantity ABSTRAL 100 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 200 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 300 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 400 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 600 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 800 MCG TAB SUBLINGUAL 90 units per 30 days ACTIQ 1,200 MCG LOZENGE 90 units per 30 days ACTIQ 1,600 MCG LOZENGE 90 units per 30 days ACTIQ 200 MCG LOZENGE 90 units per 30 days ACTIQ 400 MCG LOZENGE 90 units per 30 days ACTIQ 600 MCG LOZENGE 90 units per 30 days ACTIQ 800 MCG LOZENGE 90 units per -

Gel-Syn™ Product Information Caution
GEL-SYN™ PRODUCT INFORMATION CAUTION: Federal law restricts this device to sale by or on the order of a physician (or properly licensed practitioner). CONTENT Each 1 mL of Gel-Syn contains: Sodium Hyaluronate: 8.4 mg Sodium Chloride: 8.5 mg Sodium Phosphate, Dibasic: 0.16 mg Sodium Phosphate, Monobasic: 0.045 mg Water for Injection: q.s. to 1.0 mL DESCRIPTION Gel-Syn is a sterile, buffered solution of highly purified sodium hyaluronate with a molecular weight of approximately 1100 kDa, obtained through fermentation of Streptococci of Lancefield groups A and C and chemically unmodified. INDICATION Gel-Syn is indicated for the treatment of pain in osteoarthritis (OA) of the knee in patients who have failed to respond adequately to conservative non-pharmacologic therapy and simple analgesics (e.g., acetaminophen). CONTRAINDICATIONS • Do not administer to patients with known hypersensitivity (allergy) to sodium hyaluronate preparations. • Do not inject Gel-Syn into the knees of patients having knee joint infections or skin diseases or infections in the area of the injection site. WARNINGS • Do not concomitantly use disinfectants containing quaternary ammonium salts for skin preparation because sodium hyaluronate can precipitate in their presence. • Inject into the synovial space only. Do not inject by intravascular route. • Do not inject outside the synovial space or into the synovial tissue or capsule. An extra- articular injection of the product can cause local adverse events. PRECAUTIONS General • The safety and effectiveness of Gel-Syn in locations other than the knee, and for conditions other than osteoarthritis, have not been established. • Strict aseptic administration technique must be followed. -
Pricing Sheet
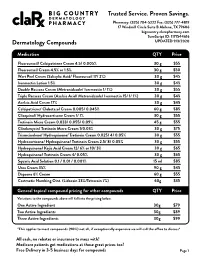
Trusted Service. Proven Savings. Pharmacy: (325) 704-5222 Fax: (325) 777-4819 17 Windmill Circle Suite B Abilene, TX 79606 bigcountry.clarxpharmacy.com SureScript ID: 1171544616 Dermatology Compounds UPDATED 9/3/2020 Medication QTY Price Fluorouracil/ Calcipotriene Cream 4.5/ 0.005% 30 g $55 Fluorouracil Cream 4.5% or 1.5% 30 g $50 Wart Peel Cream (Salicylic Acid/ Fluorouracil 17/ 2%) 30 g $45 Ivermectin Lotion 1.5% 30 g $45 Double Rosacea Cream (Metronidazole/ Ivermectin 1/ 1%) 30 g $55 Triple Rosacea Cream (Azelaic Acid/ Metronidazole/ Ivermectin 15/ 1/ 1%) 30 g $45 Azelaic Acid Cream 17% 30 g $45 Calcipotriene/ Clobetasol Cream 0.005/ 0.045% 60 g $85 Clioquinol/ Hydrocortisone Cream 1/ 1% 30 g $55 Tretinoin Micro Cream 0.033/ 0.055/ 0.09% 45 g $55 Clindamycin/ Tretinoin Micro Cream 1/0.03% 30 g $75 Triamcinolone/ Hydroquinone/ Tretinoin Cream 0.025/ 4/ 0.05% 30 g $55 Hydrocortisone/ Hydroquinone/ Tretinoin Cream 2.5/ 8/ 0.05% 30 g $55 Hydroquinone/ Kojic Acid Cream 12/ 6% or 10/ 3% 30 g $65 Hydroquinone/ Tretinoin Cream 4/ 0.05% 30 g $65 Squaric Acid Solution 0.1 / 0.01 / 0.001% 15 ml $85 Urea Cream 35% 90 g $45 Dapsone 6% Cream 60 g $55 Costmetic Numbing Oint. (Lidocain 23%/Tetracain 7%) 60g $35 General topical compound pricing for other compounds QTY Price Variations to the compounds above will fall into the pricing below. One Active Ingredient 30g $79 Two Active Ingredients 30g $89 Three Active Ingredients 30g $99 *This applies to most compounds (90%) not all, if exceptionally expensive we will call the office to discuss* All cash, no rebates or insurance to mess with! Medicare patients get medications at these great prices too! Free Delivery in 3-5 business days for compounds Page 1 Trusted Service. -

Physical-Chemical Characteristics of Whitening Toothpaste and Evaluation of Its Effects on Enamel Roughness
Dental materials Physical-chemical characteristics of whitening toothpaste and evaluation of its effects on enamel roughness Sérgio Paulo Hilgenberg(a) Abstract: This in vitro study evaluated the physical-chemical characteris- (a) Shelon Cristina Souza Pinto tics of whitening toothpastes and their effect on bovine enamel after ap- Paulo Vitor Farago(b) Fábio André Santos(a) plication of a bleaching agent (16% carbamide peroxide). Physical-chem- Denise Stadler Wambier(a) ical analysis was made considering mass loss by desiccation, ash content and pH of the toothpastes. Thirty bovine dental enamel fragments were prepared for roughness measurements. The samples were subjected to (a) Department of Dentistry, School of Dentistry, Ponta Grossa State University, bleaching treatments and simulated brushing: G1. Sorriso Dentes Brancos Ponta Grossa, PR, Brazil. (Conventional toothpaste), G2. Close-UP Whitening (Whitening tooth- (b) Department of Pharmacy, School of paste), and G3. Sensodyne Branqueador (Whitening toothpaste). The av- Dentistry, Ponta Grossa State University, erage roughness (Ra) was evaluated prior to the bleaching treatment and Ponta Grossa, PR, Brazil. after brushing. The results revealed differences in the physical-chemical characteristics of the toothpastes (p < 0.0001). The final Ra had higher values (p < 0.05) following the procedures. The mean of the Ra did not show significant differences, considering toothpaste groups and bleach- ing treatment. Interaction (toothpaste and bleaching treatment) showed significant difference -

Fee-For-Service Preferred Drug List
Prescription Drug Program Apple Health Medicaid: Fee-for-Service Preferred Drug List What is new in this version of the preferred drug list? Effective for dates of service on and after October 1, 2018, the Health Care Authority will make the following changes: Change Due to the implementation of the Apple Health Preferred Drug List (PDL), a PDL that applies to fee-for-service (FFS) clients as well as Apple Health managed care enrollees, the following changes have occurred: On the Fee-For-Service only Preferred Drug List • Drug classes that are currently on the Apple Health PDL have been removed. These classes and the drug statuses can be found on the Apple Health Preferred Drug List. On the Apple Health Preferred Drug List • New drug classes have been added. This means drugs not previously on the PDL have been added with preferred and nonpreferred statuses. Some drugs may also have additional prior authorization (PA) requirements. • For existing drug classes, preferred statuses may have changed. Some drugs may have additional PA requirements that did not previously require PA. October 25, 2018 Correction • Two drug classes were erroneously removed and have been added back to the list: Asthma – Leukotriene Modifiers Skeletal Muscle Relaxants (Rev. 10/24/2018) (Eff. 10/1/2018) – 1 – Apple Health Medicaid PDL Prescription Drug Program What is the preferred drug list? The Health Care Authority (the agency) has developed a list of preferred drugs within a chosen therapeutic class that are selected based on clinical evidence of safety, efficacy, and effectiveness. The drugs within a chosen therapeutic class are evaluated by the Drug Use Review Board, which makes recommendations to the agency regarding the selection of the preferred drugs. -

Study Protocol
RESEARCH PROTOCOL Project Title A multicenter, single blind, randomized controlled trial of virucidal effect of Polyvinylpyrrolidone-Iodine on SARS-CoV-2 as well as safety of its application on nasopharynx & oropharynx of COVID-19 positive patients BMRC Reg. No: 38624012021 Page-1/17 Project Title A multicenter, single blind, randomized controlled trial of virucidal effect of Polyvinylpyrrolidone- Iodine on SARS-CoV-2 as well as safety of its application on nasopharynx & oropharynx of COVID- 19 positive patients. Summary Povidone Iodine (Iodine with water soluble polymer Polyvinylpyrolidone) or PVP-I is a proven and time trusted antiseptic agent having best possible (99.99%) virucidal effect in it‟s only 0.23% concentration, against all viruses including SARS-Co, MERS-CoV; even in SARS-COV-2 due to it‟s nonspecific mode of action for virus killing and having no resistance [1,2]. Corona virus is transmitted by/via respiratory droplets or aerosol, produced from sneezing or coughing of infected persons to healthy individual through mouth and nose mainly [5, 6]. The routes of entry of coronavirus in human body are mouth, nose and eye. PVP-I products for gargling the throat and spraying or washing the nose may have a preventive effect on COVID-19 and if it is proved in this study following human trial, this will be a landmark research in COVID-19 pandemic. In line of this, PVP-I containing oro-nasal spray, proposed Bangasafe, which should be regarded as PONS (Povidone Iodine oro-nasal spray) in this protocol, has been developed and proposed to use against corona virus disease. -

An Introduction to Fast Dissolving Oral Thin Film Drug Delivery Systems: a Review
Muthadi Radhika Reddy /J. Pharm. Sci. & Res. Vol. 12(7), 2020, 925-940 An Introduction to Fast Dissolving Oral Thin Film Drug Delivery Systems: A Review Muthadi Radhika Reddy1* 1School of pharmacy, Gurunanak Institute of Technical Campus, Hyderabad, Telangana, India and Department of Pharmacy, Gandhi Institute of Technology and Management University, Vizag, Andhra Pradesh, India INTRODUCTION 2. Useful in situations where rapid onset of action Fast dissolving drug delivery systems were first developed required such as in motion sickness, allergic attack, in the late 1970s as an alternative to conventional dosage coughing or asthma forms. These systems consist of solid dosage forms that 3. Has wide range of applications in pharmaceuticals, Rx disintegrate and dissolve quickly in the oral cavity without Prescriptions and OTC medications for treating pain, the need of water [1]. Fast dissolving drug delivery cough/cold, gastro-esophageal reflux disease,erectile systems include orally disintegrating tablets (ODTs) and dysfunction, sleep disorders, dietary supplements, etc oral thin films (OTFs). The Centre for Drug Evaluation [4] and Research (CDER) defines ODTs as,“a solid dosage 4. No water is required for the administration and hence form containing medicinal substances which disintegrates suitable during travelling rapidly, usually within a matter of seconds, when placed 5. Some drugs are absorbed from the mouth, pharynx upon the tongue” [2]. USFDA defines OTFs as, “a thin, and esophagus as the saliva passes down into the flexible, non-friable polymeric film strip containing one or stomach, enhancing bioavailability of drugs more dispersed active pharmaceutical ingredients which is 6. May offer improved bioavailability for poorly water intended to be placed on the tongue for rapid soluble drugs by offering large surface area as it disintegration or dissolution in the saliva prior to disintegrates and dissolves rapidly swallowing for delivery into the gastrointestinal tract” [3]. -

Acrylamide Polymerization — a Practical Approach
electrophoresis tech note 1156 Acrylamide Polymerization — A Practical Approach Paul Menter, Bio-Rad Laboratories, 2000 Alfred Nobel Drive, Polyacrylamide Gel Polymerization Hercules, CA 94547 USA AcrylamideBis Polyacrylamide Introduction The unparalleled resolution and flexibility possible with CH2 CH + CH2 CH CH2 CH CH2 CH CH2 CH polyacrylamide gel electrophoresis (PAGE) has led to its CO CO CO CO CO widespread use for the separation of proteins and nucleic NH2 NH NH2 NH2 NH acids. Gel porosity can be varied over a wide range to meet CH2 CH2 specific separation requirements. Electrophoresis gels and NH NH NH NH buffers can be chosen to provide separation on the basis of CO 2 2 CO CO C O charge, size, or a combination of charge and size. CH2 CH CH2 CH CH2 CH CH2 CH The key to mastering this powerful technique lies in the polymerization process itself. By understanding the important Purity of Gel-Forming Reagents parameters, and following a few simple guidelines, the novice Acrylamide can become proficient and the experienced user can optimize Gel-forming reagents include the monomers, acrylamide and bis, separations even further. as well as the initiators, usually ammonium persulfate and TEMED or, occasionally, riboflavin and TEMED. On a molar This bulletin takes a practical approach to the preparation of basis, acrylamide is by far the most abundant component in the polyacrylamide gels. Its purpose is to provide the information monomer solution. As a result, acrylamide may be the primary required to achieve reproducible, controllable polymerization. source of interfering contaminants (Dirksen and Chrambach For those users interested only in the “bare essentials,” the 1972). -

Sucralfate Enemas
Sucralfate Enemas Sucralfate enemas are used to treat inflammation of the rectum (the lower part of the large intestine leading to the anus); most commonly this is for radiation proctitis; bowel inflammation following radiotherapy. This treatment can help treat bleeding due to the inflammation, and can be continued for up to 24 weeks; you can stop when the bleeding stops. This fact sheet explains how you can administer the enema yourself, using a syringe and catheter. The hospital or community pharmacy can provide the Sucralfate enema, and you will need to ask your GP or practise nurse to supply the equipment you will need. Your practise nurse can help you practice preparing the enema, and could help you with administering it at home, if you find this difficult. 1. Using the syringe provided, draw up 10mls of the Sucralfate Suspension (2g) and then draw up 10mls of warm water and mix. Ensure that any excess air is expelled from the syringe. 2. Attach the catheter provided to the syringe tip and lubricate the end of the catheter with lubricating gel provided. 3. Lie on your left side with both knees bent. This position will help the flow of liquid in to the rectum and aid enema retention. 4. Position a towel underneath yourself to catch any leakage of fluid once the enema has been administered. 5. With a steady pressure, gently insert the catheter to a depth of approximately 10cm into the rectum. 6. Press down on the barrel of the syringe slowly, using a steady and even pressure, until the entire contents of the syringe have been administered.