Social Isolation in Bristol 2013. Initial Findings Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Impacts of Mayoral Governance in Bristol
The Bristol Civic Leadership Project The Impacts of Mayoral Governance in Bristol Robin Hambleton and David Sweeting September 2015 The Bristol Civic Leadership Project The Impacts of Mayoral Governance in Bristol Robin Hambleton and David Sweeting September 2015 Contents List of tables 4 List of figures 5 Executive summary 6 1 Introduction: what this report is about 8 2 Context: the debate about directly elected mayors in the UK 11 3 The Bristol Civic Leadership Project 15 4 Leadership in the community 21 5 Effective representation of the citizen 26 6 Legitimacy and accountability 31 7 Effectiveness in decision-making and implementation 34 8 Effective scrutiny of policy and performance 39 9 Responsiveness to local people 43 10 Strategic choices for urban governance in Bristol in 2025 45 Notes 50 Appendix 1: Survey research methods 51 Appendix 2: Socio-economic geography of Bristol 54 Appendix 3: Citizens’ Panel survey, 2012 and 2014, percent agree, by 56 ward socio-economic category Appendix 4: Civic Leaders’ survey, 2012 and 2014, percent agree, by 59 realm of leadership About the authors 61 Acknowledgements 62 3 List of tables 1 Bristol wards by socio-economic category 17 2 Citizens’ Panel survey, 2012 and 2014, leadership in the community, 21 percent agree 3 Civic Leaders’ survey, 2012 and 2014, leadership in the community, 23 percent agree 4 Citizens’ Panel survey, 2012 and 2014, effective representation of the 26 citizen, percent agree 5 Civic Leaders’ survey, 2012 and 2014, effective representation of the 28 citizen, percent agree, -

Plan Your Journey, Find Bus Stops Nearby and Track Your Bus Using
10 • Thornbury • Bristol Parkway • Southmead • Lawrence Weston • Avonmouth 11 • Bristol Parkway • Southmead • Shirehampton • Avonmouth 10 11 MONDAY TO FRIDAY (excluding Bank Holidays) 10 11 10 11 10 11 10 ● 11 10 11 10 ◆ 11 11 10 11 Thornbury Health Centre –––– 0718 ––– 0928 – 28 – – 1428 – Thornbury Easton Hill Road –––– 0725 – 0835 – 0935 – 35 – – 1435 – Thornbury Rock Street –––– 0733 – 0843 – 0943 – 43 – – 1443 – Thornbury Tesco –––––––– 0946 – 46 – – 1446 – Thornbury Bockenham Close – – – – 0738 – 0848 – 0950 – Then 50 – – 1450 – Hortham Viburnum Road –––– 0754 – 0904 – 1004 – at 04 – – 1504 – Aztec West Roundabout [C] – 0551 0711 – 0806 – 0911 – 1011 – 11 – – 1511 – these Bristol Parkway Station .Arr – 0601 0721 – 0818 – 0923 – 1023 – 23 – – 1523 – mins until Bristol Parkway Station Dep 0433 0603 0723 0753 0823 0853 0928 0958 1028 1058 28 58 1458 1528 1603 UWE Frenchay Campus 0440 0610 0733 0803 0833 0903 0938 1008 1038 1108 past 38 08 1508 1538 1615 Southmead Hospital 0455 0625 0753 0823 0853 0923 0955 1025 1055 1125 each 55 25 1525 1555 1635 Westbury–on–Trym Co–op 0505 0630 0807 0837 0907 0937 1007 1037 1107 1137 hour 07 37 1537 1610 1650 Shirehampton Green – 0639 – 0847 – 0947 – 1047 – 1147 – 47 1547 – 1700 Lawrence Weston Moor Grove 0514 – 0817 – 0917 – 1017 – 1117 – 17 – – 1620 – Avonmouth Mclaren Road 0522 0647 0827 0857 0927 0957 1027 1057 1127 1157 27 57 1557 1630 1710 Severn Beach Govier Way 0537 ––––––––– –– ––– Key ● on Schooldays bus runs via Castle School [0828]; – Stop not served on School Holidays via Health Centre -

Area Green Space Plan - Henbury and Southmead
Area Green Space Plan - Henbury and Southmead Consideration of the value of Brentry Hill Open Space prior to identifying it in the Area Green Space Plan for potential disposal for development. Notes to support interpretation of assessment carried out in July 2009. Introduction • The Parks and Green Space Strategy was adopted by Bristol City Council in February 2008 with a clear aim to improve the city's accessible green spaces - providing new facilities, providing them where they are needed across the city and arresting the decline resulting from decades of under investment. • One of the funding methods adopted by the Strategy was to sell some green space and reinvest 70% of money raised back in to improving more important spaces. • Area Green Space Plan ideas and options papers, currently out for consultation until October 29th 2010, identify where potential disposal spaces are. How were potential disposal spaces identified: • The Parks and Green Space Strategy set out how potential disposal spaces should be identified. The minimum open space provision standards adopted by the Strategy were applied and a range of value criteria also considered. • The value criteria, as set out in the Strategy are given below: Community value This is an assessment of a site’s value to the local community based on both feedback from local people and knowledge of changes taking place in the area. Factor Example of type of considerations Level of use Current use and potential for improved use Community views of the Does the community think it’s important and why? space Views of different groups will be considered. -

Step 1: What Is the Proposal? Please Explain Your Proposal in Plain English, Avoiding Acronyms and Jargon
Bristol City Council Equality Impact Assessment Form – St Werburgh’s Primary School Input (Please refer to the Equality Impact Assessment guidance when completing this form) Name of proposal Draft Model Risk Assessment for Schools Re- Opening after Covid-19 Closure Directorate and Service Area People , Education Services Name of Lead Officer Christina Czarkowski Crouch Step 1: What is the proposal? Please explain your proposal in Plain English, avoiding acronyms and jargon. This section should explain how the proposal will impact service users, staff and/or the wider community. 1.1 What is the proposal? The model risk assessment for School Re-Opening, has been prepared to assist Schools negotiate the various Public Health England guidance in relation to the risks associated with the COVID 19 virus. The assessment has been prepared to help Schools instigate suitable control measures to help protect the School’s Staff / Pupils and Visitors. The risk assessment has been fully completed for the planned wider opening of St Werburgh’s Primary School to children in Reception, Year 1 and Year 6. The proposal is to open for small groups of pupils in Reception, Year 1 and Year 6 initially on a part time basis form Monday 8th June if the government and Bristol City Council advise that it is safe for us to do so. This will ensure that children can be in a familiar setting with familiar staff and come back into school in a phased way. Each group of children will operate as a ‘bubble’ which will not come into contact with or interact with other ‘bubbles’ of children. -

505 Bus Service
y a W s r e i l l o C E VAL ASHTON ASHTON LONG LONG L o n P&R g A s Long Ashton Long h t o n d a B o R y r e P d e a e s F s A 3 A s h t o 7 n 0 R o a d Centre B 3 Fitness Fitness 1 2 8 Lloyd David David 9 2 0 Street 3 A Parson Parson d a Ground o R Ashton Recreation e k o Gores Marsh Gores The t s r e t n i Road W ASHTON Winterstoke B l a A L c BOWER s a k h t m n o e n o l R o C o m r a a s h M n d w Stadium o R a r (Faculty of Art, Media & Design) & Media Art, of (Faculty Ashton Gate Ashton s h The West of England of West The R Mansion o a Lane University of of University d Ashton Court Ashton Blackmoors d A a o s R h r t o o o n m k c Park u D R o Smyth Smyth a d Greville Greville 9 6 3 A d a o R BEDMINSTER Factory e g Estate Court Ashton The Tobacco The C a l i f t n H o a u s l e R C o a d B r C u o n Record Office Record r o e n l CREATE & Bristol Bristol & CREATE a Bridge t W i m u o von A C b n e a r l a R y n o d a d R Yard o A a 3 d 7 0 Underfall Bridge Park SOUTHVILLE Plimsoll Basin Caravan Cumberland B a s i n R d Brunel Lock Brunel R o d w n n h a l a m r e H i b l l m M u C e B Artspace r r c i d h g a Spike Island Spike e n Merchants Road Merchants R t o C o r o n s a t a i o n R o a d d A 3 7 0 R d River Avon River n C u m o b e d r l a n Marina d v t w o e R H l l o R o a a a H d d o p e C h a l p l e i l A H o Institute Bristol R r Square e l l H v & The Brunel Brunel The & C i o e A Dowry t l R w m i w Trinity Church Trinity e f t SS Great Britain Great SS b t l r b o a N u r H g n i o r t l a o l F o o a R r H t Matthew -

Bristol and B&NES FOOD Clubs March 2021
Bristol and B&NES FOOD Clubs March 2021 Day Club Status Contact Tuesday Stockwood Children’s Centre Spaces Helen Richards 0117 353 3503 9.15-11.15am Whittock Rd, Bristol BS14 8DQ available [email protected] Tuesday Lockleaze The Vench, FULL Amy Walsh 0117 910 3930 9.30-11.30am Romney Ave, Lockleaze, Bristol BS7 9TB [email protected] Tuesday Broomhill, St Peter’s Methodist Church, Spaces Claire Bowen 0117 353 4276 12.30-2.30pm 170 Allison Rd, Brislington. available [email protected] Tuesday Knowle West Children’s Centre Spaces Janet Nawrocki 07910833689 2.30-4.30pm Leinster Avenue, Knowle West, Bristol, available [email protected] United Kingdom BS4 1NN Wednesday St Pauls Children’s Centre FULL Yvonne Young 07467335706 9.30-11.30am Family Hub, Little Bishop Street [email protected] BS2 9JF Wednesday Redcliffe Children’s Centre Spaces Sharon/Fatuma 0117 9030334 12.30-2.30pm Freeling house, Prewett street, available [email protected] BS1 6RE Wednesday Barton Hill Wellspring Settlement Spaces Gabrielle Lobb 0117 9556971 1-3pm 43 Ducie Rd BS5 0AX available [email protected] Wednesday Lawrence Weston Spaces Sadie Fox 07410898062 1.30-3.30pm Oasis Hub House – 98B Long Cross, Available [email protected] Lawrence Weston, BS11 Wednesday Patchway Spaces Jayne Anstis 01454 868470 1.30-3.30pm Coniston Café, Coniston Rd, Patchway, Available [email protected] Bristol BS34 5LP Thursday Southmead Children’s Centre Spaces Emily -

Situation of Polling Stations
SITUATION OF POLLING STATIONS Election of the Mayor for West of England Combined Authority Hours of Poll:- 7:00 am to 10:00 pm Notice is hereby given that: The situation of Polling Stations and the description of persons entitled to vote thereat are as follows: Ranges of electoral register Station Situation of Polling Station numbers of persons entitled Number to vote thereat St Bartholomew's Church - Upper Hall, Sommerville 1-WEST ASHA-1 to ASHA-1610 Road, Bristol Sefton Park Infant & Junior School, St Bartholomew's 2-WEST ASHB-1 to ASHB-1195 Road, Bristol St Bartholomew's Church - Upper Hall, Sommerville 3-WEST ASHC-1 to ASHC-1256 Road, Bristol Salvation Army Citadel, 6 Ashley Road, Bristol 4-WEST ASHD-1 to ASHD-1182/1 Ivy Pentecostal Church, Assemblies of God, Ashley 5-WEST ASHE-1 to ASHE-1216 Hill, Montpelier Ivy Pentecostal Church, Assemblies of God, Ashley 6-WEST ASHF-2 to ASHF-1440 Hill, Montpelier St Werburgh's Community Centre, Horley Road, St 7-WEST ASHG-1 to ASHG-1562 Werburghs Salvation Army Citadel, 6 Ashley Road, Bristol 8-WEST ASHH-1 to ASHH-1467 Malcolm X Community Centre, 141 City Road, St 9-WEST ASHJ-1 to ASHJ-1663 Pauls St Paul`s Community Sports Academy, Newfoundland 10- ASHK-1 to ASHK-966 Road, Bristol WEST St Paul`s Community Sports Academy, Newfoundland 11- ASHL-1 to ASHL-1067 Road, Bristol WEST Avonmouth Community Centre, Avonmouth Road, 12-NW AVLA-3 to AVLA-1688 Bristol Nova Primary School, Barracks Lane, Shirehampton 13-NW AVLB-1 to AVLB-1839 Hope Cafe and Church, 117 - 119 Long Cross, 14-NW AVLC-1 to AVLC-1673 -

Hotwells and Cliftonwood Community Association – Newsletter July 2021
Hotwells and Cliftonwood Community Association – Newsletter July 2021 Dear Neighbour Welcome to the Bulletin for July 2021. Hot air balloons have begun to dot Bristol’s blue skies and open-air theatre productions are in full swing. You could be forgiven for having missed these if you’ve been busy following the Euros, Wimbledon or maybe Love Island, a show which Alan Bennett said, reminded him of the Bloomsbury set! Personally, it was a month of firsts. I had my first vaccine jab and visited a cinema and barbershop for the first time in a year. I hope the rest of the year can continue to be as thrilling. Picture Credit: Neha Goel HCCA Newsletter – July 2021 Page 1 of 14 Should you wish to raise any local issues/matters of interest, we can always be contacted at the following: [email protected] or leave a message on 01179 291 833. If there is anything you have written and would like to add to the next Bulletin – please send it to this email [email protected] HCCA Newsletter – July 2021 Page 2 of 14 In this issue: 1. Come rain, come shine. ......................................................................................... 4 2. Hotwells Skate Spot- The ramps are arriving! ........................................................ 5 3. Cumberland Basin/Western Harbour ...................................................................... 6 4. Heritage Assessment – The River Avon ................................................................. 6 5. Ashton Gate development ..................................................................................... -

Bristol City Council Polling Districts
Bristol City Council Polling districts AVONMOUTH A SOUTHMEAD A HENBURY D HENBURY C HENBURY A HENBURY B KINGSWESTON A SOUTHMEAD B SOUTHMEAD D KINGSWESTON B SOUTHMEAD C HORFIELD A WESTBURY ON TRYM A HORFIELD B AVONMOUTH C AVONMOUTH B KINGSWESTON C WESTBURY ON TRYM D LOCKLEAZE A WESTBURY ON TRYM B HORFIELD D HORFIELD C LOCKLEAZE B AVONMOUTH D FROME VALE A AVONMOUTH E FROME VALE C HENLEAZE A HORFIELD E HENLEAZE B STOKE LOCKLEAZE A KINGSWESTON D BISHOP A WESTBURY ON TRYM C AVONMOUTH F FROME VALE B BISHOPSTON D LOCKLEAZE C BISHOPSTON A EASTVILLE A FROME VALE D HENLEAZE C STOKE BISHOP B STOKE BISHOP C REDLAND A HILLFIELDS B BISHOPSTON B BISHOPSTON C EASTVILLE B LOCKLEAZE D HILLFIELDS A REDLAND B REDLAND C EASTVILLE C REDLAND D ASHLEY A HILLFIELDS C ASHLEY C STOKE BISHOP D COTHAM A HILLFIELDS E HILLFIELDS D CLIFTON EAST A ASHLEY B EASTVILLE D EASTON A COTHAM D COTHAM B COTHAM C CLIFTON EAST B ST GEORGE WEST D EASTON D EASTON B ASHLEY D LAWRENCE HILL A ASHLEY E ST GEORGE EAST D ST GEORGE WEST A CABOT B ST GEORGE WEST C CABOT C ST GEORGE EAST A CLIFTON A CLIFTON EAST C LAWRENCE HILL B CABOT A LAWRENCE HILL C ST GEORGE WEST B CLIFTON C EASTON C CLIFTON B LAWRENCE HILL E CABOT G ST GEORGE EAST B CABOT D ST GEORGE EAST C CLIFTON E CLIFTON D LAWRENCE HILL D BRISLINGTON EAST A LAWRENCE HILL F BRISLINGTON EAST B CABOT E CABOT F BRISLINGTON WEST A WINDMILL HILL A SOUTHVILLE A SOUTHVILLE B SOUTHVILLE C SOUTHVILLE D BRISLINGTON EAST C WINDMILL HILL C BRISLINGTON WEST C WINDMILL HILL D WINDMILL HILL B BRISLINGTON WEST B BEDMINSTER E BEDMINSTER C BRISLINGTON EAST D KNOWLE B BEDMINSTER B KNOWLE A BEDMINSTER A WINDMILL HILL E BEDMINSTER D FILWOOD B BRISLINGTON WEST D KNOWLE C FILWOOD A KNOWLE D BISHOPSWORTH B STOCKWOOD A BRISLINGTON WEST E BISHOPSWORTH A FILWOOD D STOCKWOOD C HENGROVE A FILWOOD C HARTCLIFFE A STOCKWOOD B STOCKWOOD E BISHOPSWORTH C HENGROVE C HENGROVE B STOCKWOOD D STOCKWOOD F HARTCLIFFE C BISHOPSWORTH D WHITCHURCH PARK B HARTCLIFFE B HENGROVE D WHITCHURCH PARK C WHITCHURCH PARK D WHITCHURCH PARK A WHITCHURCH PARK E. -

13 Bus Time Schedule & Line Route
13 bus time schedule & line map 13 Broadmead View In Website Mode The 13 bus line (Broadmead) has 3 routes. For regular weekdays, their operation hours are: (1) Broadmead: 6:35 AM - 5:15 PM (2) Filton: 6:45 PM (3) Shirehampton: 7:30 AM - 5:40 PM Use the Moovit App to ƒnd the closest 13 bus station near you and ƒnd out when is the next 13 bus arriving. Direction: Broadmead 13 bus Time Schedule 70 stops Broadmead Route Timetable: VIEW LINE SCHEDULE Sunday Not Operational Monday 6:35 AM - 5:15 PM Dursley Road, Shirehampton Tuesday 6:35 AM - 5:15 PM Stroud Road, Shirehampton Wednesday 6:35 AM - 5:15 PM Nibley Road, Shirehampton Thursday 6:35 AM - 5:15 PM Nibley Road, Bristol Friday 6:35 AM - 5:15 PM Hung Road, Shirehampton Saturday 7:05 AM - 5:15 PM Pembroke Avenue, Shirehampton 32 Station Road, Bristol Shirehampton Grn, Shirehampton High Street, Bristol 13 bus Info Direction: Broadmead Woodleaze, Sea Mills Stops: 70 Trip Duration: 85 min The Pentagon, Sea Mills Line Summary: Dursley Road, Shirehampton, Stroud The Pentagon, Bristol Road, Shirehampton, Nibley Road, Shirehampton, Hung Road, Shirehampton, Pembroke Avenue, Sea Mills Square, Sea Mills Shirehampton, Shirehampton Grn, Shirehampton, 139 Shirehampton Road, Bristol Woodleaze, Sea Mills, The Pentagon, Sea Mills, Sea Mills Square, Sea Mills, High Grove, Sea Mills, High Grove, Sea Mills Shirehampton Park, Shirehampton, Elberton Road, 204 Shirehampton Road, Bristol Coombe Dingle, Haig Close, Coombe Dingle, Southside Close, Coombe Dingle, Southwood Drive, Shirehampton Park, Shirehampton -

Henbury, Brentry & Southmead Neighbourhood Partnership
Henbury, Brentry & Southmead Neighbourhood Partnership Tuesday 27th September 2016 Report of: Keith Houghton, Neighbourhood Partnership Co-ordinator. Title: Henbury, Brentry & Southmead NP Plan Update Report Contact Telephone Number: 0117 922 2135 Recommendations 1 The NP to note the broad picture of engagement from equalities communities in the NP’s work which emerges from the monitoring conducted in Quarter 1 on 2016/17 and the recommendation to use this information in planning engagement work at the next NP Plan event. Item 1 2. The NP note the updates on actions to deliver the existing NP Plan, in particular a forward look at young people’s provision in the light on the new Henbury Centre and Southmead Youth Centre Item 3.1 c and delivering Parks/Open Spaces consultation to update the detail in the NP Plan (4.1) over the Autumn & new access work in Southmead (4.2); Updates on delivery of Doncaster Road crossing and the crack and seat work on Doncaster Road (5.6) 3. That the NP notes the action to progress the Wellbeing Fund working group Item 4 4. the NP notes the successful presentation on Parks access work by Deana Perry and Cllr Massey at the July Citywide NP meeting. Item 5 1. NP Plan and Governance and Equalities/Engagement Review: 1.1 The NP Plan/Governance event date is being agreed at the 27th September NP meeting. 1.2 Equalities Review 2016: a. Across April, May and June 2016 all NP-related events and activities included an Equalities monitoring element to capture information about the participation levels of different sections of the community by recognised Equalities Communities b. -
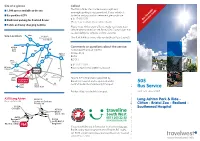
505 Bus Service
.travelwest.info www BD11449 DesignedandprintedonsustainablysourcedmaterialbyBristolDesign,CityCouncil-January2019 on 0117 922 2910 922 0117 on CD-ROM or plain text please contact Bristol City Council Council City Bristol contact please text plain or CD-ROM Braille, audio tape, large print, easy English, BSL video, video, BSL English, easy print, large tape, audio Braille, If you would like this information in another language, language, another in information this like would you If Southmead Hospital Southmead Clifton - Bristol Zoo - Redland - - Redland - Zoo Bristol - Clifton Postcode BS3 2HB BS3 Postcode - Ride & Park Ashton Long Ashton Long A370 Produced by Sustainable Transport. Sustainable by Produced Valid from January 2019 January from Valid Bus Service Bus Shepton Mallet Shepton contract by Bristol Community Transport. Community Bristol by contract 505 under operated is and Council City Bristol Service 505 is financially supported by by supported financially is 505 Service Bristol Somerset [email protected] e: M5 South M5 2910 922 0117 t: BS3 9FS BS3 2 M3 1 Bristol East 3176 Box PO Sustainable Transport (100TS) Transport Sustainable service the about questions or Comments est W (The Park & Ride is now solely run by Bristol City Council). City Bristol by run solely now is Ride & Park (The Site Location Site accept liability for vehicles or their contents. their or vehicles for liability accept vehicle when parked on site, Bristol City Council does not not does Council City Bristol site, on parked when vehicle Please note, whilst every effort is made to protect your your protect to made is effort every whilst note, Please Toilets and baby changing facilities changing baby and Toilets n Information Inside Information (Please note a callout charge will be made) be will charge callout a note (Please Dedicated parking for disabled drivers disabled for parking Dedicated n Timetable Bus 1550 903 0117 t: phone please it, retrieve to wish you and in locked Car park has CCTV CCTV has park Car n is vehicle your If permitted.