Paper SELECTIVE SHIELDING of BONE MARROW
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Radiation Risk Assessment
PS008-1 RISK ASSESSMENT POSITION STATEMENT OF THE HEALTH PHYSICS SOCIETY* Adopted: July 1993 Revised: April 1995 Contact: Brett Burk Executive Secretary Health Physics Society Telephone: 703-790-1745 Fax: 703-790-2672 Email: [email protected] http://www.hps.org Risk assessment is the process of describing and characterizing the nature and magnitude of a particular risk and includes gathering, assembling, and analyzing information on the risk. Risk assessment is a foundation of risk management and risk communication. In order to effectively manage risks and to communicate risks to the public, a clear understanding of the nature and magnitude of the risk at relevant exposure levels is necessary. The Health Physics Society has become increasingly concerned with the erratic application of risk assessment in the establishment of radiation protection regulations. These regulations are inconsistent, poorly coordinated among federal agencies, and inadequately communicated to the public. Examples of problem areas include (1) 100- to 1,000-fold discrepancies in permissible exposure levels among various regulations, all allegedly based on the same scientific risk-assessment data, and (2) proposed expenditures of billions of federal and private dollars to clean up radioactively contaminated federal and commercial sites without careful consideration of the actual public health benefits to be achieved. The Health Physics Society recognizes that there are many questions and uncertainties associated with the risk-assessment process and that data may be incomplete or missing. Accordingly, limitations in risk assessment must be fully recognized and made explicit in establishing regulations for the protection of the public health. The Health Physics Society supports risk assessments that are consistent, of high technical quality, unbiased, and based on sound, objective science. -

Radiation Risk in Perspective
PS010-1 RADIATION RISK IN PERSPECTIVE POSITION STATEMENT OF THE HEALTH HEALTH PHYSICS SOCIETY* PHYSICS SOCIETY Adopted: January 1996 Revised: August 2004 Contact: Richard J. Burk, Jr. Executive Secretary Health Physics Society Telephone: 703-790-1745 Fax: 703-790-2672 Email: [email protected] http://www.hps.org In accordance with current knowledge of radiation health risks, the Health Physics Society recommends against quantitative estimation of health risks below an individual dose of 5 rem1 in one year or a lifetime dose of 10 rem above that received from natural sources. Doses from natural background radiation in the United States average about 0.3 rem per year. A dose of 5 rem will be accumulated in the first 17 years of life and about 25 rem in a lifetime of 80 years. Estimation of health risk associated with radiation doses that are of similar magnitude as those received from natural sources should be strictly qualitative and encompass a range of hypothetical health outcomes, including the possibility of no adverse health effects at such low levels. There is substantial and convincing scientific evidence for health risks following high-dose exposures. However, below 5–10 rem (which includes occupational and environmental exposures), risks of health effects are either too small to be observed or are nonexistent. In part because of the insurmountable intrinsic and methodological difficulties in determining if the health effects that are demonstrated at high radiation doses are also present at low doses, current radiation protection standards and practices are based on the premise that any radiation dose, no matter how small, may result in detrimental health effects, such as cancer and hereditary genetic damage. -

HEALTH PHYSICS SOCIETY POLICY on EXPENDITURE of FUNDS for IONIZING RADIATION HEALTH EFFECTS STUDIES Approved by the Board of Directors: November 1998
HEALTH PHYSICS SOCIETY Specialists in Radiation Safety HEALTH PHYSICS SOCIETY POLICY ON EXPENDITURE OF FUNDS FOR IONIZING RADIATION HEALTH EFFECTS STUDIES Approved by the Board of Directors: November 1998 PREMISE: 1. Funding resources for studying the health effects of human exposure to ionizing radiation are limited. 2. The number of research and study activities related to studying and understanding the health effects of ionizing radiation exceeds the funding resources available. 3. The highest priority of funding work on ionizing radiation health effects should be work with a reasonable likelihood of defining, or significantly increasing the understanding of, the carcinogenic response in the range of occupational and public exposures. 4. A second priority of funding work on ionizing radiation health effects should be work assisting in the establishment of reasonable protection criteria which do not result in an inappropriate expenditure of public funds for purported protection. This is necessary for the period in which there is a lack of definitive knowledge or understanding of the dose response. 5. Epidemiological studies alone will not provide definitive evidence of the existence or non-existence of carcinogenic effects due to low dose or low dose-rate radiation. RECOMMENDATIONS: 1. Do not fund epidemiological studies of exposed populations which have low statistical power and are unable to detect health effects with a reasonable statistical confidence (e.g., 90% or higher) based on the current risk estimates. 2. Do not fund epidemiological studies on populations for which there is insufficient data to properly control for known confounding factors, such as smoking history, exposure to other carcinogens, genetic pre-disposition, etc. -

Uranium Fact Sheet
Fact Sheet Adopted: December 2018 Health Physics Society Specialists in Radiation Safety 1 Uranium What is uranium? Uranium is a naturally occurring metallic element that has been present in the Earth’s crust since formation of the planet. Like many other minerals, uranium was deposited on land by volcanic action, dissolved by rainfall, and in some places, carried into underground formations. In some cases, geochemical conditions resulted in its concentration into “ore bodies.” Uranium is a common element in Earth’s crust (soil, rock) and in seawater and groundwater. Uranium has 92 protons in its nucleus. The isotope2 238U has 146 neutrons, for a total atomic weight of approximately 238, making it the highest atomic weight of any naturally occurring element. It is not the most dense of elements, but its density is almost twice that of lead. Uranium is radioactive and in nature has three primary isotopes with different numbers of neutrons. Natural uranium, 238U, constitutes over 99% of the total mass or weight, with 0.72% 235U, and a very small amount of 234U. An unstable nucleus that emits some form of radiation is defined as radioactive. The emitted radiation is called radioactivity, which in this case is ionizing radiation—meaning it can interact with other atoms to create charged atoms known as ions. Uranium emits alpha particles, which are ejected from the nucleus of the unstable uranium atom. When an atom emits radiation such as alpha or beta particles or photons such as x rays or gamma rays, the material is said to be undergoing radioactive decay (also called radioactive transformation). -

HPS Publications Style Guide
Health Physics Society Publications Style Guide January 2019 Table of Contents I. General Guidelines for HPS Documents and Web Pages ................................................... 2 A. Abbreviations ............................................................................................................. 2 B. Capitalization ............................................................................................................. 3 C. Format ........................................................................................................................ 3 D. Internet ....................................................................................................................... 4 E. Numbers, Units, and Symbols ................................................................................... 4 1. Numbers ............................................................................................................... 4 2. Units of measure .................................................................................................. 5 3. Symbols................................................................................................................ 6 F. Punctuation ................................................................................................................ 6 G. Radionuclides and Elements ...................................................................................... 8 H. References, Citations, Resources, Footnotes, and Press Releases ............................. 8 1. References -

Radiation and Risk: Expert Perspectives Radiation and Risk: Expert Perspectives SP001-1
Radiation and Risk: Expert Perspectives Radiation and Risk: Expert Perspectives SP001-1 Published by Health Physics Society 1313 Dolley Madison Blvd. Suite 402 McLean, VA 22101 Disclaimer Statements and opinions expressed in publications of the Health Physics Society or in presentations given during its regular meetings are those of the author(s) and do not necessarily reflect the official position of the Health Physics Society, the editors, or the organizations with which the authors are affiliated. The editor(s), publisher, and Society disclaim any responsibility or liability for such material and do not guarantee, warrant, or endorse any product or service mentioned. Official positions of the Society are established only by its Board of Directors. Copyright © 2017 by the Health Physics Society All rights reserved. No part of this publication may be reproduced or distributed in any form, in an electronic retrieval system or otherwise, without prior written permission of the publisher. Printed in the United States of America SP001-1, revised 2017 Radiation and Risk: Expert Perspectives Table of Contents Foreword……………………………………………………………………………………………………………... 2 A Primer on Ionizing Radiation……………………………………………………………………………... 6 Growing Importance of Nuclear Technology in Medicine……………………………………….. 16 Distinguishing Risk: Use and Overuse of Radiation in Medicine………………………………. 22 Nuclear Energy: The Environmental Context…………………………………………………………. 27 Nuclear Power in the United States: Safety, Emergency Response Planning, and Continuous Learning…………………………………………………………………………………………….. 33 Radiation Risk: Used Nuclear Fuel and Radioactive Waste Disposal………………………... 42 Radiation Risk: Communicating to the Public………………………………………………………… 45 After Fukushima: Implications for Public Policy and Communications……………………. 51 Appendix 1: Radiation Units and Measurements……………………………………………………. 57 Appendix 2: Half-Life of Some Radionuclides…………………………………………………………. 58 Bernard L. -

Health Physics Society 51St Annual Meeting
CENTER FOR NUCLEAR WASTE REGULATORY ANALYSES TRIP REPORT SUBJECT: Health Physics Society 51" Annual Meeting Project No. 20.6002.01.372 and 20.6002.01.01 1 AI No. 20.6002.01.372.602 DATWPLACE: June 25-29,2006 Providence, Rhode Island AUTHOR(S): James Durham and Ali Simpkins Center for Nuclear Waste Regulatory Analyses (CNWRA) DISTRIBUTION: DHLWRS RES G EDENW RA SwRl D. DeMarco S. Bush-Goddard W. Patrick Record Copy B, IQS V. Whipple H. Karagiannis 6. Sagar S. Kim GED Directors W. Reamer MSlB GED Managers L. Kokajko P. LaPlante E. Collins S. Sherbini R. Janetzke A. Campbell 0. Pensado K. Stablein J. Mancillas M. Bailey R. Benke J. Guttmann J. Durham W. Smith L. Howard T. McCartin 0. Osidele J. Rubenstone A. Simpkins K. Compton R. Nes M. Waters 0. Povetko B. Hill L. Gutierrez M. Shah J. Chen D. Brooks CENTER FOR NUCLEAR WASTE REGULATORY ANALYSES TRIP REPORT SUBJECT: Health Physics Society 51" Annual Meeting Project Nos. 20.6002.01.372 and 20.6002.01.01 1 AI No. 20.6002.01.372.602 DATWPLACE: June 25-29,2006 Providence, Rhode Island AUTHOR(S): James Durham and Ali Simpkins Center for Nuclear Waste Regulatory Analyses (CNWRA) PERSONS PRESENT: J. Durham, A. Simpkins, and over 1,000 other attendees from around the world. BACKGROUND AND PURPOSE OF TRIP: The Health Physics Society Annual Meeting is a premier forum that allows health physicists from around the world to interact and present their technical work. The format of this year's meeting included a plenary session followed by individual sessions to present work in different areas of health physics. -

Measuring Radioactivity
Health Physics Society Public Education Committee Fact Sheet MEASURING RADIOACTIVITY Because ionizing radiation cannot be detected with our human senses, we use various types of instruments and radiation detectors to measure the amount of radiation present. We usually measure both the amount of radioactivity in a radioisotope source, and the ionizing radiation field density being emitted by the source. We define radioactivity as the number of atoms which decay (disintegrate) in a radioisotope sample in a given period of time. The base unit is the Becquerel (Bq) or one disintegration per second (dps). This number is very small and therefore, not very useful. For this reason we use the Curie (Ci) which is 37 billion Bq. Because we often use very large or very small numbers when discussing radioactivity, we use a series o f prefixes which express multiples of 1000. The following table shows some of these prefixes: milli (m) = 1/1,000 kilo (k) = times 1,000 micro (u) = 1/1,000,000 mega (M) = times 1,000,000 nano (n) 1/1,000,000,000 giga (G) times 1,000,000,000 Pico (P) 1/1,000,000,000,000 tera (T) times 1,000,000,000,000 Using the table, a mCi = 1/1000 of a Curie and a GBq 1,000,000,000 Becquerels. To put this in perspective, a normal home smoke detector contains a small sealed source of about 10 uCi (370,000 Bq) of radioactivity. Ionizing radiation fields are expressed in units of Roentgens (R) which is equivalent to the number of atoms of a gas which are ionized. -

HPS Publications Style Guide
Health Physics Society Publications Style Guide February 2020 Table of Contents I. General Guidelines for HPS Documents and Web Pages ................................................... 2 A. Abbreviations .............................................................................................................................. 2 B. Capitalization ............................................................................................................................... 3 C. Format .......................................................................................................................................... 3 D. Internet ......................................................................................................................................... 4 E. Nuclides and Elements .............................................................................................................. 4 F. Numbers, Units, and Symbols ................................................................................................... 5 1. Numbers ............................................................................................................................. 5 2. Units of measure ............................................................................................................... 6 3. Symbols ............................................................................................................................. 6 G. Punctuation ................................................................................................................................ -

Environmental Radiation Fact Sheet
Fact Sheet Adopted: January 2010 Health Physics Society Specialists in Radiation Safety Environmental Radiation Linnea E. Wahl, Lawrence Berkeley National Laboratory The background level of radiation in the natural environment surrounds us at all times—it is ubiquitous. Since the Earth formed and life developed, background radiation* has been our constant companion. Sources of Background Radiation by space radiation are called cosmogenic radionuclides. Background radiation (which scientists call “ubiquitous They include tritium (hydrogen-3), beryllium-7, carbon- background radiation”) is emitted from both natural 14, and sodium-22. and human-made radioactive chemicals (radionuclides). Some naturally occurring radionuclides are found in the Terrestrial Radiation earth beneath our feet, while others are produced in the Radiation that originates on Earth is called terrestrial atmosphere by radiation from space. Human-made radi- radiation. Primordial radionuclides (radioactive chemi- onuclides have entered the environment from activities cals that were present when the Earth formed about 4.5 such as medical procedures that use radionuclides to billion years ago) are found around the globe in igneous image the body and electricity generation that uses radi- and sedimentary rock. From rocks, these radionuclides oactive uranium as fuel. migrate into soil, water, and even air. Human activities such as uranium mining have also redistributed these Humans are continuously irradiated by sources outside radionuclides. Primordial radionuclides include the se- and inside their bodies. Outside sources include space ries of radionuclides produced when uranium and tho- radiation and terrestrial radiation. Inside sources include rium decay, as well as potassium-40 and rubidium-87. the radionuclides that enter our bodies in the food and water people ingest and the air they breathe. -
Annual Meeting Program
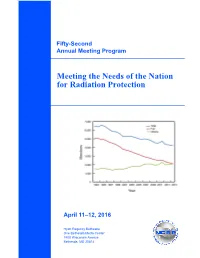
Fifty-Second Annual Meeting Program Meeting the Needs of the Nation for Radiation Protection April 11–12, 2016 Hyatt Regency Bethesda One Bethesda Metro Center 7400 Wisconsin Avenue Bethesda, MD 20814 Front cover: Membership of the U.S. Health Physics Society, 1993 to 2015 [NCRP Statement No. 12, Where are the Radiation Professionals (WARP)?, issued December 17, 2015]. Statement No. 12 is available for free at http://ncrpon- line.org/wp-content/themes/ncrp/PDFs/Statement_12.pdf. NCRP Mission: To support radiation protection by providing independent scientific analysis, information and recommendations that represent the consensus of leading scientists. NCRP Resource Development Committee is launching a series of efforts to increase the financial stability of NCRP. The first effort is to request Council members and friends who shop online at Amazon to make a simple (no cost) modification. Simply register at AmazonSmile (https://smile.amazon.com/), and the AmazonSmile Foundation will donate 0.5 % of the purchase price to NCRP at no charge to you! It’s easy! Follow the directions and be sure to select the National Council on Radiation Protection and Measure- ments (from the pull down list or searchable request) as the 501(c)(3) public charitable organization to receive the Amazon contribution for each purchase. Donations are anonymous. However, we would like to recognize your support and if you notify NCRP ([email protected]) we will add your name to the NCRP list of AmazonSmile contributors. Introduction Meeting the Needs of the Nation for Radiation Protection Fifty-Second Annual Meeting of the National Council on Radiation Protection and Measurements (NCRP) In June 2013, NCRP hosted a Workshop to address the consideration of the inexorable effects of population question of “where are the radiation professionals?” This demographics on the future radiological workforce. -

Health Physics Society Factsheet
HEALTH PHYSICS SOCIETY Specialists in Radiation Safety Web: http://www.hps.org 1313 Dolley Madison Blvd., Suite 402 Email: [email protected] McLean, VA 22101 Fax: 703-790-2672 Phone: 703-790-1745 The Health Physics Society, formed in 1956, is a scientific organization of professionals who specialize in radiation safety. Its mission is excellence in the science and practice of radiation safety. Today its nearly 5,000 members represent all scientific and technical areas related to radiation safety including academia, government, medicine, research and development, analytical services, consulting, and industry in all 50 states and the District of Columbia. The Society is chartered in the United States as an independent nonprofit scientific organization, and, as such, is not affiliated with any government or industrial organization or private entity. Its headquarters are in McLean, Virginia. The Society is dedicated to the development, dissemination, and application of scientific and practical knowledge regarding radiation safety and control. Expertise of the members of the Health Physics Society: Members of the Health Physics Society work in a variety of professional areas including research, industry, education, environmental protection, governmental activities, regulation, enforcement, and medicine. Research - Health physics researchers investigate principles by which radiation interacts with matter and living systems. The field also involves study of environmental transport of radioactivity and the effects of radiation on biological organisms. Research is used in many ways, ranging from designing radiation detection instrumentation to health risk assessments necessary for establishing radiation protection standards. Industry - Applied health physicists draw on their technical knowledge to advise, recommend, and implement methods and appropriate equipment for use in industrial work involving radionuclides and radiation.