Course Session
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Idiopathic Spiny Keratoderma: a Report of Two Cases and Literature Review
Idiopathic Spiny Keratoderma: A Report of Two Cases and Literature Review Jessica Schweitzer, DO,* Matthew Koehler, DO,** David Horowitz, DO*** *Intern, Largo Medical Center, Largo, FL **Dermatology Resident, Third Year, College Medical Center/Western University, Long Beach, CA ***Dermatology Residency Program Director, College Medical Center/Western University, Long Beach, CA Abstract Spiny keratoderma is a rare and likely underreported condition that presents with punctate hyperkeratotic growths localized to the palms and soles. We present two cases of clinically diagnosed spiny keratoderma. Although the lesions were asymptomatic, patients are at risk of an underlying internal malignancy with this condition, so diagnosis is crucial. Neither men were seeking treatment for the lesions when they were discovered, suggesting that this condition may be much more common than reported. Patients with histories of manual labor, increased UV exposure, and non-melanoma skin cancer (NMSC) may also be at higher risk for developing spiny keratoderma.1 The epidemiology, histopathologic features, differential diagnosis, and current treatments for spiny keratoderma are reviewed. Introduction Case 2 enthusiast for his entire life, spending significant Spiny keratoderma is a rare palmoplantar A 67-year-old Caucasian male presented with a time using his hands to maintain and fire his keratoderma that presents with keratotic, pinpoint one-year history of insidiously growing, pinpoint weapons and many hours outside without sun papules on the palms and soles. There are both hyperkeratotic papules projecting from his palms protection. The patient was referred back to his hereditary and acquired forms. When found, bilaterally (Figures 4-5). He presented to the clinic primary care physician for internal evaluation. -

Living with Mast Cell Activation Syndrome
Anne Maitland, MD, PhD Living with Medical Director, Comprehensive Allergy Mast Cell & Asthma Care Activation Asst Professor, Dept of Medicine – Clinical Immunology Syndrome Icahn School of Medicine at Mt Sinai, New York Got MCAS? Mast Cell mediated disorders are common u 1 out of 2 of us are coping with some chronic immune mediated disorder. o ‘allergies’(rhinitis), sinus infections, hives (urticaria),food allergy/intolerance, skin swelling (angioedema), Anaphylaxis Signs and Symptoms eczema (atopic dermatitis and contact dermatitis), asthma issues, and the prototype of immediate hypersensitivity syndromes, anaphylaxis Why the rise in hypersensitivity disorders? Our genes in this environment! The human race has come to dominate its environment so completely that any analysis of the increase or appearance of a disease has to take changes in our lifestyle into account. In the case of allergic disease [hypersensitivity disorders] changes in our environment, diet, water quality, and personal behavior over the last 150 years have played a dominant role in the specificity of these diseases, as well as in prevalence and severity… it is clear that the consequences of hygiene, indoor entertainment, and changes in diet or physical activity have never been predicted. Thomas A. E. Platts-Mills, MD, PhD, FRS, The allergy epidemics: 1870-2010; J Allergy Clin Immunol 2015;136:3-13. Why? Trauma Stress Infection Connective Tissue Chemical Disorder exposure PIDD -manufactured Autoimmune Dz. -mold, Mastocytosis mycotoxins Hypertryptasemia (naturally Atopic Disorders occuring) Mast cell activation syndrome is easily treated, if it's But most patients with recognized MCAD suffer for Patients with mast cell activation syndrome (MCAS) frequently go for years without an accurate diagnosis… Harding, Reuters Health-New York, 2011 years… It is very common for one hypersensitivity condition to progress/morph into another, be provoked by more triggers. -

Dissecting Cellulitis
Patient Information Leaflet Dr Paul Farrant FRCP Consultant Dermatologist Janet Dix (Secretary to Dr Paul Farrant) Tel 01444 412273 Fax 01444 657397 Email [email protected] Web drpaulfarrant.co.uk Dissecting Cellulitis What is dissecting cellulitis? Dissecting cellulitis is a type of scarring hair loss that presents with pustules, boggy swellings, and sinuses within the scalp. What causes dissecting cellulitis? The cause of dissecting cellulitis is not known. It is associated with severe cystic acne known as acne conglobata, and hidradenitis suppurativa, which causes cystic swellings in the armpits and groin. In all of these conditions the hair follicle becomes blocked, dilates and ruptures. This causes an inflammatory response in the skin, which leads to pus formation, swellings and sinus formation. It is not uncommon for bacteria to be isolated from the skin but this is likely to be secondary to the inflammatory process. Is dissecting cellulitis inherited? Dissecting cellulitis is most commonly seen in Afro-Caribbean men but the racial predilection is more likely to be due to the shape and structural differences of Afro-Caribbean hair than a genetic predisposition to the condition. Hair care practices, such as clipping, may also play a role. It is not thought to be an inherited condition. What are the symptoms? Patients with dissecting cellulitis often complain of pain, tenderness and fluid discharge from the affected area. It is associated with hair loss. What does dissecting cellulitis look like? Dissecting Cellulitis is characterised by a localised area of hair loss, pustules, boggy swellings and sinus formation. Gentle pressure on the boggy areas may lead to expression of pus or serous fluid. -

Guidelines of Care for the 10 Most Common Dermatologic Diseases
1 Guidelines of Care for the 10 most common dermatologic diseases: Copyright by the American Academy of Dermatology, Inc. Disclaimer Adherence to these guidelines will not ensure successful treatment in every situation. Further, these guidelines should not be deemed inclusive of all proper methods of care or exclusive of other methods of care reasonably directed to obtaining the same results. The ultimate judgment regarding the propriety of any specific procedure must be made by the physician in light of all the circumstances presented by the individual patient. For the benefit of members of the American Academy of Dermatology who practice in countries outside the jurisdiction of the United States, the listed treatments may include agents that not currently approved by the U.S. Food and Drug Administration. 1. Acne Vulgaris 2. Alopecia Areata 3. Atopic Dermatitis 4. Contact Dermatitis 5. Cutaneous Adverse Drug Reactions 6. Nail Disorders 7. Psoriasis 8. Superficial Mycotic Infections of the Skin: Mucocutaneous Candidiasis, Onychomycosis, Piedra, Pityriasis, Tinea Capitis , Tinea Barbae, Tinea Corporis, Tinea Cruris, Tinea Faciei, Tinea Manuum, and Tinea Pedis. 9. Vitiligo 10. Warts: Human Papillomavirus 1 2 1- Guidelines of Care for Acne Vulgaris* Reference: 1990 by the American Academy of Dermatology, Inc. I. Introduction The American Academy of Dermatology’s Committee on Guidelines of Care is developing guidelines of care for our profession. The development of guidelines will promote the continued delivery of quality care and assist those outside our profession in understanding the complexities and boundaries of care provided by dermatologists. II. Definition Acne vulgaris is a follicular disorder that affects susceptible pilosebaceous follicles, primarily of the face, neck, and upper trunk, and is characterized by both noninflammatory and inflammatory lesions. -

Palmoplantar Keratoderma with Progressive Gingivitis and Recurrent Pyodermas
Palmoplantar Keratoderma With Progressive Gingivitis and Recurrent Pyodermas Tyler A. Moss, DO; Anne P. Spillane, MD; Sam F. Almquist, MD; Patrick E. McCleskey, MD; Oliver J. Wisco, DO Practice Points Papillon-Lefèvre syndrome (PLS) is an autosomal-recessive inherited transgredient palmoplantar kerato- derma (PPK) that is associated with gingivitis and recurrent pyodermas. The symptoms associated with PLS are thought to be due to cathepsin C gene, CTSC, mutations. CTSC is expressed in epithelial regions commonly affected by PLS and also plays a role in the activation of immune and inflammatory responses. Papillon-Lefèvre syndrome must be differentiated from other conditions causing PPK, such as Haim-Munk syndrome, Greither syndrome, mal de Meleda, Clouston syndrome, Vohwinkel syndrome, and Olmsted syndrome. Treatment of PLS includesCUTIS keratolytics such as urea and/or salicylic acid comb ined with oral retinoids. Active gingivitis may be treated with combined use of amoxicillin and metronidazole. Papillon-Lefèvre syndrome (PLS) is a rare inher- Case Report ited palmoplantar keratoderma (PPK) that is asso- A 30-year-old woman presented to the dermatology ciated with progressive gingivitis and recurrent clinic with erythematous hyperkeratotic plaques on pyodermas.Do We present a caseNot exhibiting classic the palmsCopy and soles. The plaques extended onto features of this autosomal-recessive condition the dorsal aspects of the fingers, toes, hands, and and review the current understanding of its patho- feet (Figures 1 and 2). The patient had psoriasiform physiology, diagnosis, and treatment. Addition- plaques on the extensor surfaces of the knees and ally, a review of pertinent transgredient PPKs is elbows (Figure 3) along with a history of slow- undertaken, with key and distinguishing features progressing gingivitis and periodontal disease that of each syndrome highlighted. -

Pediatric and Adolescent Dermatology
Pediatric and adolescent dermatology Management and referral guidelines ICD-10 guide • Acne: L70.0 acne vulgaris; L70.1 acne conglobata; • Molluscum contagiosum: B08.1 L70.4 infantile acne; L70.5 acne excoriae; L70.8 • Nevi (moles): Start with D22 and rest depends other acne; or L70.9 acne unspecified on site • Alopecia areata: L63 alopecia; L63.0 alopecia • Onychomycosis (nail fungus): B35.1 (capitis) totalis; L63.1 alopecia universalis; L63.8 other alopecia areata; or L63.9 alopecia areata • Psoriasis: L40.0 plaque; L40.1 generalized unspecified pustular psoriasis; L40.3 palmoplantar pustulosis; L40.4 guttate; L40.54 psoriatic juvenile • Atopic dermatitis (eczema): L20.82 flexural; arthropathy; L40.8 other psoriasis; or L40.9 L20.83 infantile; L20.89 other atopic dermatitis; or psoriasis unspecified L20.9 atopic dermatitis unspecified • Scabies: B86 • Hemangioma of infancy: D18 hemangioma and lymphangioma any site; D18.0 hemangioma; • Seborrheic dermatitis: L21.0 capitis; L21.1 infantile; D18.00 hemangioma unspecified site; D18.01 L21.8 other seborrheic dermatitis; or L21.9 hemangioma of skin and subcutaneous tissue; seborrheic dermatitis unspecified D18.02 hemangioma of intracranial structures; • Tinea capitis: B35.0 D18.03 hemangioma of intraabdominal structures; or D18.09 hemangioma of other sites • Tinea versicolor: B36.0 • Hyperhidrosis: R61 generalized hyperhidrosis; • Vitiligo: L80 L74.5 focal hyperhidrosis; L74.51 primary focal • Warts: B07.0 verruca plantaris; B07.8 verruca hyperhidrosis, rest depends on site; L74.52 vulgaris (common warts); B07.9 viral wart secondary focal hyperhidrosis unspecified; or A63.0 anogenital warts • Keratosis pilaris: L85.8 other specified epidermal thickening 1 Acne Treatment basics • Tretinoin 0.025% or 0.05% cream • Education: Medications often take weeks to work AND and the patient’s skin may get “worse” (dry and red) • Clindamycin-benzoyl peroxide 1%-5% gel in the before it gets better. -

Erythrokeratodermia Variabilis Et Progressiva Allelic to Oculo-Dento
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector COMMENTARY See related article on pg 1540 translocated into the plasma membrane. Once expressed on the cell surface, the hemichannel docks with a connexon of an adjacent cell to form a channel that Erythrokeratodermia Variabilis et is termed gap junction. Connexons can form either homotypic (docking of two Progressiva Allelic to Oculo-Dento- identical connexons), heterotypic (docking of two dissimilar homomeric Digital Dysplasia connexons), or heteromeric (docking of two heteromeric connexons) channels Sabine Duchatelet1,2 and Alain Hovnanian1,2,3 (Mese et al., 2007). These diverse Erythrokeratodermia variabilis et progressiva (EKVP) is a genodermatosis with combinations of connexins create clinical and genetic heterogeneity, most often transmitted in an autosomal different types of channels, each having dominant manner, caused by mutations in GJB3 and GJB4 genes encoding unique properties (ionic conductance, connexins (Cx)31 and 30.3, respectively. In this issue, Boyden et al. (2015) report permeability, sensitivity to voltage, or for the first time de novo dominant mutations in GJA1 encoding the ubiquitous pH). Of note, several connexins may also Cx43 in patients with EKVP. These results expand the genetic heterogeneity of form functional nonjunctional hemi- EKVP and the human disease phenotypes associated with GJA1 mutations. They channels, although their physiological disclose that EKVP is allelic to oculo-dento-digital dysplasia, a rare syndrome relevance remains uncertain (Pfenniger previously known to be caused by dominant GJA1 mutations. et al., 2010). Mutations in 11 connexin genes cause a variety of genetic dis- Journal of Investigative Dermatology (2015) 135, 1475–1478. -

Palmoplantar Keratoderma: Rare Case Report
Case Report Journal of Volume 12:4, 2021 Cytology & Histology ISSN: 2157-7099 Open Access Palmoplantar Keratoderma: Rare Case Report Dr. Ayushi Bansal1, Dr. Hemlata Munde2*, Dr. Munish Gupta3 and Dr. Santosh Munde4 1Senior Resident, Department of Pathology, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 2Professor and Head of Department of Pathology, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 3Assistant Professor, Department of medicine, Kalpana Chawla Government Medical College, Karnal, Haryana, India. 4Professor and Head of Department of Orthopaedics, Kalpana Chawla Government Medical College, Karnal, Haryana, India. Abstract Palmoplantar keratodermas(PPK) are group of cornification disorders characterized by epidermal hyperkeratotic lesions involving the palms and soles. A 50years old healthy male, presented with history of multiple punctate hyperkeratotic papules since last 5 years. Keywords: Palmoplantar keratoderma • Punctate •Hyperkeratotic papules Abbreviations: PPK: Palmoplantar keratodermas • PUVA: Psoralen plus Ultraviolet A • PPPK: Punctate Palmoplantar keratodermas • USG: Ultrasound Sonography• VRDL: Venereal Disease Research Laboratory Test • ELISA: Enzyme-Linked Immunosorbent Assay Introduction Mucosal surfaces were not involved. Biopsy sample was received. On histopathological examination of biopsy revealed massive hyperkeratosis over sharply limited area with depression of malphigian layer below general Palmoplantar keratoderma (PPK), clinically and genetically comprises level of epidermis. There was increase in the thickness of granular layer. The of heterogenous group of disorders characterised by hyperkeratosis of dermis was free of inflammation. Compilation of clinical and laboratory data palms and soles [1]. It can be hereditary or acquired. Hereditary PPK can helped to conclude the diagnosis of Palmoplantar Keratoderma-Punctate be further divided into three major categories: diffuse, focal, and punctate type. -

RD-Action Matchmaker – Summary of Disease Expertise Recorded Under
Summary of disease expertise recorded via RD-ACTION Matchmaker under each Thematic Grouping and EURORDIS Members’ Thematic Grouping Thematic Reported expertise of those completing the EURORDIS Member perspectives on Grouping matchmaker under each heading Grouping RD Thematically Rare Bone Achondroplasia/Hypochondroplasia Achondroplasia Amelia skeletal dysplasia’s including Achondroplasia/Growth hormone cleidocranial dysostosis, arthrogryposis deficiency/MPS/Turner Brachydactyly chondrodysplasia punctate Fibrous dysplasia of bone Collagenopathy and oncologic disease such as Fibrodysplasia ossificans progressive Li-Fraumeni syndrome Osteogenesis imperfecta Congenital hand and fore-foot conditions Sterno Costo Clavicular Hyperostosis Disorders of Sex Development Duchenne Muscular Dystrophy Ehlers –Danlos syndrome Fibrodysplasia Ossificans Progressiva Growth disorders Hypoparathyroidism Hypophosphatemic rickets & Nutritional Rickets Hypophosphatasia Jeune’s syndrome Limb reduction defects Madelung disease Metabolic Osteoporosis Multiple Hereditary Exostoses Osteogenesis imperfecta Osteoporosis Paediatric Osteoporosis Paget’s disease Phocomelia Pseudohypoparathyroidism Radial dysplasia Skeletal dysplasia Thanatophoric dwarfism Ulna dysplasia Rare Cancer and Adrenocortical tumours Acute monoblastic leukaemia Tumours Carcinoid tumours Brain tumour Craniopharyngioma Colon cancer, familial nonpolyposis Embryonal tumours of CNS Craniopharyngioma Ependymoma Desmoid disease Epithelial thymic tumours in -

Dermatologic Features of Smith–Magenis Syndrome
Pediatric Dermatology Vol. 32 No. 3 337–341, 2015 Dermatologic Features of Smith–Magenis Syndrome Morgane Guerin-Moreau, M.D.,*,** Estelle Colin, M.D.,†,** Sylvie Nguyen, M.D., Ph.D.,‡,** Joris Andrieux, M.D., Ph.D.,§ Helene de Leersnyder, M.D.,¶ Dominique Bonneau, M.D., Ph.D.,†,** and Ludovic Martin, M.D., Ph.D.*,** Departments of *Dermatology, †Biochemistry and Genetics, and ‡Pediatrics, University Hospital of Angers, Angers, France, §Department of Genetics, University Hospital of Lille, Lille, France, ¶Department of Pediatrics, Hopital^ Robert Debre, University of Paris VII, Paris, France, **L’UNAM University, Nantes, France Abstract: Smith–Magenis syndrome (SMS) is characterized by dis- tinctive facial and skeletal features, developmental delay, cognitive impairment, and behavioral abnormalities, including self-injurious behav- iors. We aimed to investigate whether cutaneous features are common in SMS. We performed a complete skin examination in 20 young SMS patients. Skin features secondary to self-injurious behavior, such as bites, abrasions, dystrophic scars, limited spots of hyperkeratosis, anomalies of the nails, and whitlows, were found in the majority of patients. Acral pachydermia and fissured plantar keratoderma were common. Xerosis was constant and associated with extensive keratosis pilaris in the majority of patients. Dermatofibromas were frequent in older patients. The hair was dense and shiny, with an unusual hairline. Eyelash trichomegaly and heavy brows were common, as well as folliculitis on the back. The skin features of SMS have rarely been reported in the literature. Some of these are the consequence of neurobehavioral features, but some cutaneous features and abnormalities of appendages have not been reported in other related syndromes. -
Spiny Keratoderma Thomas N
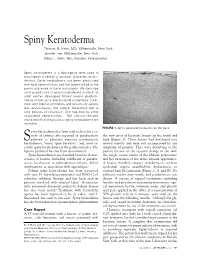
Spiny Keratoderma Thomas N. Helm, MD, Williamsville, New York Jennifer Lee, Williamsville, New York Klaus F. Helm, MD, Hershey, Pennsylvania Spiny keratoderma is a descriptive term used to encompass a variety of unusual, disparate kerato- dermas. Spiny keratoderma has been associated with lipid abnormalities and has been limited to the palms and soles in some individuals. We describe an acquired case of spiny keratoderma in which an adult woman developed filiform lesions predomi- nating on the trunk and proximal extremities. Treat- ment with topical emollients and keratolytic agents was unsuccessful, but topical tazarotene led to long periods of resolution. She has had no other associated abnormalities. The clinical features and differential diagnosis of spiny keratoderma are reviewed. FIGURE 1. Spiny keratoderma lesions on the back. piny keratoderma has been used to describe a va- riety of entities also reported as porokeratosis the new onset of keratotic lesions on the trunk and S palmaris et plantaris, punctate porokeratotic back (Figure 1). These lesions had developed over keratoderma, “music spine keratosis,” and, most re- several months and were not accompanied by any cently, spiny keratoderma of the palms and soles. Ma- symptoms of pruritus. They were disturbing to the lignant potential has not been documented. patient because of the textural change in the skin; Spiny keratodermas are classified based on charac- the rough, coarse nature of the filiform projections; teristics of lesions, including exhibition of paraker- and her awareness of her skin’s unusual appearance. atosis, localization to palmoplantar surfaces, diffuse A biopsy revealed compact orthokeratosis without involvement, or association with appendages.1 epidermal atypia, acantholytic dyskeratosis, or Palmar spiny keratoderma has been associated cornoid lamella formation (Figure 2, A and B). -

Early Diagnosis and Treatment of Discoid Lupus Erythematosus
J Am Board Fam Med: first published as 10.3122/jabfm.2009.02.080075 on 5 March 2009. Downloaded from BRIEF REPORT Early Diagnosis and Treatment of Discoid Lupus Erythematosus Suresh Panjwani, MD, MSc, FRACGP Discoid lupus erythematosus is a chronic dermatological disease that can lead to scarring, hair loss, and hyperpigmentation changes in skin if it is not treated early and promptly. It has a prolonged course and can have a considerable effect on quality of life. Early recognition and treatment improves the prog- nosis. The diagnosis is usually made by clinical examination. In some cases histopathology may be re- quired to confirm the diagnosis. The histology is that of an inflammatory interface dermatosis. There is insufficient evidence for which treatment is most effective. Because lesions are induced or exacerbated by ultraviolet exposure, photoprotective measures are important. Potent topical steroids and antima- larials are the mainstay of treatment. Some cases of discoid lupus erythematosus can be refractory to standard therapy; in these cases retinoids, thalidomide, and topical tacrolimus offer alternatives, as do immunosuppressives like azathioprine, cyclosporine, mycophenolate mofetil, and methotrexate. (J Am Board Fam Med 2009;22:206–213.) Lupus erythematosus (LE) is thought to be an 5% of patients with discoid lupus may develop autoimmune disease among other connective tissue SLE1 and 25% of patients with SLE may develop diseases like scleroderma, rheumatoid arthritis, typical chronic discoid lesions at some time during copyright.