Evolving Therapies for Liver Fibrosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

SPECIALTY MEDICATIONS Available Through Accredo Health Group, Inc., Medco’S Specialty Pharmacy Call Toll-Free (800) 803-2523, 8:00 A.M
SPECIALTY MEDICATIONS available through Accredo Health Group, Inc., Medco’s specialty pharmacy Call toll-free (800) 803-2523, 8:00 a.m. to 8:00 p.m., eastern time, Monday through Friday, to confirm that your medication is covered. Effective as of July 1, 2011 Abraxane® (paclitaxel protein-bound particles) Berinert® (C 1 esterase inhibitor [human])* (PA) (QD) Actemra ™ (tocilizumab) (PA) Betaseron® (interferon beta-1b) (PA) Actimmune® (interferon gamma-1b) (PA) Botox® (botulinum toxin type A) (PA) Adagen® (pegademase bovine) Carbaglu ™ (carglumic acid) Adcirca® (tadalafil) (ST) (QD) Carimune® NF (immune globulin intravenous [human]) (PA) Advate® (antihemophilic factor [recombinant]) (CPA) Cerezyme® (imiglucerase) (CPA) (ST) Afinitor® (everolimus) (PA) (QD) Cimzia® (certolizumab pegol) (ST) Aldurazyme® (laronidase) (CPA) Copaxone® (glatiramer acetate) (PA) Alphanate® (antihemophilic factor [human]) (CPA) Copegus® (ribavirin) (ST) AlphaNine® SD (coagulation factor IX [human]) (CPA) Corifact® (factor XIII [human]) (CPA) Amevive® (alefacept) (PA) Cystadane® (betaine) Ampyra ™ (dalfampridine) (PA) CytoGam® (cytomegalovirus immune globulin Apokyn® (apomorphine hydrochloride) (PA) (QD) intravenous [human])* (CPA) Aralast® (alpha[1]-proteinase inhibitor [human]) Cytovene® IV (ganciclovir sodium)* Aranesp® (darbepoetin alfa) (PA) Dacogen® (decitabine) Arcalyst® (rilonacept) (PA) (QD) Dysport® (abobotulinumtoxinA) (PA) Arixtra® (fondaparinux sodium)* Egrifta ™ (tesamorelin) (PA) Arranon® (nelarabine) Elaprase® (idursulfase) (CPA) Arzerra® (ofatumumab) -
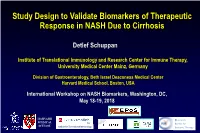
Study Design to Validate Biomarkers of Therapeutic Response in NASH Due to Cirrhosis
Study Design to Validate Biomarkers of Therapeutic Response in NASH Due to Cirrhosis Detlef Schuppan Institute of Translational Immunology and Research Center for Immune Therapy, University Medical Center Mainz, Germany Division of Gastroenterology, Beth Israel Deaconess Medical Center Harvard Medical School, Boston, USA International Workshop on NASH Biomarkers, Washington, DC, May 18-19, 2018 HARVARD Research MEDICAL Center for SCHOOL Institute for Translational Immunology Immune Therapy No Conflict of Interest to Declare Related to this Presentation Fibrosis Progression and Reversal in NASH Inflammation, the reparative response and evolution of fibrosis/cirrhosis in NASH Fibrogenesis • is a waxing and waning process A • follows inflammation (reparative response) inflammation fibrosis Severity Time B Severity Time Antifibrotic therapy C cirrhosis Severity Time Schuppan et al, J Hepatol 2018 Fibrogenesis in NASH Ox. stress, ROS normal liver macrophage Insulin resistance, FFA Toxins repetitive damage MF Toxic bile salts (multiple hits) T (Auto-) Immunity HBV, HCV genetic Microbiome, nutrients quiescent predisposition stellate cell (lipoapoptotic) hepatocytes activated cholangiocytes endothelium fibrotic liver portal or collagen- Cirrhosis perivascular synthesis fibroblast organ MMP-1/3/13 failure activated matrix accumulation myofibroblast TIMP-1 Cirrhosis and HCC HSC TIMP-2 Schuppan and Afdhal, Lancet 2008 common pathways & Schuppan and Kim, JCI 2013 immune environment ! Inhibition of fibrogenesis - induction of fibrolysis normal -
What Lessons Can We Learn from 20 Years of Chemokine T D Di ? Receptor
What lessons can we learn from 20 years of chemokine receptdtor drug discovery? John G. Cumming, PhD 5th RSC / SCI symposium on GPCRs in Medicinal Chemistry 15th-17th September 2014, Actelion, Allschwil, Basel, Switzerland Outline Background: chemokines and their receptors Chemokine receptor drug discovery and development Emerging opportunities for chemokine drug discovery Conclusions and learning Chemokines and chemokine receptors CXC(α) • Chemokines (chemoattractant cytokines) are 70-120 aa proteins • 44 chemokines in 4 major families and 22 chemokine receptors in human genome • ‘Cell positioning system’ in the body • Many receptors bind multiple ligands • Many ligands bind multiple receptors Chemotaxis Human monocytes + CCL2 (red) Volpe et al. PLoS ONE 2012, 7(5), e37208 CCR2 antagonists inhibit chemotaxis and infiltration Vasculature CCL2 release Spinal or Peripheral Tissue Recruited monocyte Site of CCL2 release CCR2 antagonists inhibit chemotaxis and infiltration CCR2 antagonist Circulating monocyte CCL2 release CCL2 release from peripheral injury site or central PAF terminals Role of chemokine system in pathophysiology • Potential role in inflammatory and autoimmune diseases: Multiple sclerosis, Rheumatoid arthritis, COPD, allergic asthma, IBD, psoriasis - Expression levels of chemokines and receptors in relevant tissues and organs of patients and animal disease models - Mouse knockout ppyphenotype in disease models • Established role in HIV infection Katschke et al., 2001 Arthritis Rheum, 44, 1022 - CCR5 and CXCR4 act as HIV-1 -

Supplementary Material Table of Contents
Supplementary M aterial Table of Contents 1 - Online S u pplementary Methods ………………………………………………...… . …2 1.1 Study population……………………………………………………………..2 1.2 Quality control and principal component analysis …………………………..2 1.3 Statistical analyses………………………………………… ………………...3 1.3.1 Disease - specific association testing ……………………………… ..3 1.3.2 Cross - phenotype meta - analysis …………………………………… .3 1.3.3 Model search ……………………………………………………… .4 1.3.4 Novelty of the variants …………………………………………… ..4 1.3.5 Functional Enrichment Analy sis ………………………………… ...4 1.3.6 Drug Target Enrichment Analysis ………………………………… 5 2 - Supplementary Figures………………………………………...………………… . …. 7 3 - Members of the Myositis Genetics Consortium (MYOGEN) ……………………. ..16 4 - Members of the Scleroderma Genetics Consortium ………………… ……………...17 5 - Supplementary References………………………………………………………… . .18 6 - Supplementary Tables………………………………………………………… . ……22 1 Online supplementary m ethods Study population This study was conducted using 12,132 affected subjects and 23 ,260 controls of European des cent population and all of them have been included in previously published GWAS as summarized in Table S1. [1 - 6] Briefly, a total of 3,255 SLE cases and 9,562 ancestry matched controls were included from six countrie s across Europe and North America (Spain, Germany, Netherlands, Italy, UK, and USA). All of the included patients were diagnosed based on the standard American College of Rheumatology (ACR) classification criteria. [7] Previously described GWAS data from 2,363 SSc cases and 5,181 ancestry -

Mozobil (Plerixafor Injection) AHM
Mozobil (Plerixafor Injection) AHM Clinical Indications • Mozobil (Plerixafor Injection) in combination with granulocyte-colony stimulating factor (G-CSF) is considered medically necessary to mobilize hematopoietic stem cells to the peripheral blood for collection and subsequent autologous transplantation for patients who have failed a prior mobilization attempts with G-CSF with 1 or more of the following conditions o Lymphoma (i.e., Hodgkin's disease and non-Hodgkin's lymphoma) o Multiple myeloma o Germ cell tumors o WHIM (warts, hypogammaglobulinemia, infections and myelokathexis) syndrome • Current role remains uncertain. Based on review of existing evidence, there are currently no clinical indications for this technology. See Inappropriate Uses for more detailed analysis of the evidence base. Mozobil is considered investigational for all other indications Evidence Summary • Background • There has been a steady rise in the use of peripheral blood stem cells (PBSC) as a source of hematopoietic stem cells. In general, less than 0.05 % of white blood cells (WBC) are CD34+ cells. Chemotherapy results in a 5- to 15-fold increase of PBSC. Chemotherapy in combination with growth factors increases CD34+ cells up to 6 % of WBC. In the allogeneic setting, granulocyte-colony stimulating factor (G-CSF) is used alone for mobilization of PBSC. Several factors affect PBSC mobilization; including age, gender, type of growth factor, dose of the growth factor, and in the autologous setting, the patient's diagnosis, chemotherapy regimen and number of previous chemotherapy cycles or radiation. Muscle and bone pain are common side effects in allogeneic stem cell mobilization, but are usually tolerated with the use of analgesics. -

Outcome Measures in Coeliac Disease Trials
Downloaded from http://gut.bmj.com/ on March 30, 2018 - Published by group.bmj.com Gut Online First, published on February 13, 2018 as 10.1136/gutjnl-2017-314853 Coeliac disease ORIGINAL ARTICLE Outcome measures in coeliac disease trials: the Tampere recommendations Jonas F Ludvigsson,1,2 Carolina Ciacci,3 Peter HR Green,4 Katri Kaukinen,5,6 Ilma R Korponay-Szabo,7,8 Kalle Kurppa,9,10 Joseph A Murray,11 Knut Erik Aslaksen Lundin,12,13 Markku J Maki,14,15 Alina Popp,16,17 Norelle R Reilly,18,19 Alfonso Rodriguez-Herrera,20 David S Sanders,21 Detlef Schuppan,22,23 Sarah Sleet,24 Juha Taavela,25 Kristin Voorhees,26 Marjorie M Walker,27 Daniel A Leffler28 ► Additional material is ABSTRact published online only. To view, Objective A gluten-free diet is the only treatment Significance of this study please visit the journal online option of coeliac disease, but recently an increasing (http:// dx. doi. org/ 10. 1136/ What is already known about this subject? gutjnl- 2017- 314853). number of trials have begun to explore alternative treatment strategies. We aimed to review the literature ► A gluten-free diet is the only treatment option For numbered affiliations see of coeliac disease, but recently an increasing end of article. on coeliac disease therapeutic trials and issue recommendations for outcome measures. number of trials have begun to explore alternative treatment strategies. Correspondence to Design Based on a literature review of 10 062 Dr Jonas F Ludvigsson, references, we (17 researchers and 2 patient ► A large number of trials of non-dietary Department of Medical representatives from 10 countries) reviewed the use treatments for coeliac disease are ongoing or Epidemiology and Biostatistics, and suitability of both clinical and non-clinical outcome under way. -

Macrophages in Nonalcoholic Steatohepatitis: Friend Or Foe?
Macrophages in Nonalcoholic Steatohepatitis: Friend or Foe? Authors: Joel Grunhut,1 Wei Wang,1 Berk Aykut,1 Inderdeep Gakhal,1 Alejandro Torres-Hernandez,1 *George Miller1,2 1. S.A. Localio Laboratory, Department of Surgery, New York University School of Medicine, New York City, New York, USA 2. Department of Cell Biology, New York University School of Medicine, New York City, New York, USA *Correspondence to [email protected] Disclosure: The authors have declared no conflicts of interest. Received: 14.11.17 Accepted: 28.02.18 Keywords: Inflammation, macrophage, steatohepatitis. Citation: EMJ Hepatol. 2018;6[1]:100-109. Abstract Nonalcoholic steatohepatitis (NASH) is a subtype of nonalcoholic fatty liver disease that is characterised by steatosis, chronic inflammation, and hepatocellular injury with or without fibrosis. The role and activation of macrophages in the pathogenesis of NASH is complex and is being studied for possible therapeutic options to help the millions of people diagnosed with the disease. The purpose of this review is to discuss the pathogenesis of NASH through the activation and role of Kupffer cells and other macrophages in causing inflammation and progression of NASH. Furthermore, this review aims to outline some of the current therapeutic options targeting the pathogenesis of NASH. INTRODUCTION The progression to NASH from its less severe form of NAFLD can be predicted by the amount of inflammation present in hepatic tissue.2 Nonalcoholic steatohepatitis (NASH), a subtype Severe inflammation can contribute to the of nonalcoholic fatty liver disease (NAFLD), is progression of other liver diseases, such as one of the most prevalent ongoing liver diseases cirrhosis, fibrosis, and hepatocellular carcinoma. -

Documents Numérisés Par Onetouch
19 ORGANISATION AFRICAINE DE LA PROPRIETE INTELLECTUELLE 51 8 Inter. CI. C07D 471/04 (2018.01) 11 A61K 31/519 (2018.01) N° 18435 A61P 29/00 (2018.01) A61P 31/12 (2018.01) A61P 35/00 (2018.01) FASCICULE DE BREVET D'INVENTION A61P 37/00 (2018.01) 21 Numéro de dépôt : 1201700355 73 Titulaire(s): PCT/US2016/020499 GILEAD SCIENCES, INC., 333 Lakeside Drive, 22 Date de dépôt : 02/03/2016 FOSTER CITY, CA 94404 (US) 30 Priorité(s): Inventeur(s): 72 US n° 62/128,397 du 04/03/2015 CHIN Gregory (US) US n° 62/250,403 du 03/11/2015 METOBO Samuel E. (US) ZABLOCKI Jeff (US) MACKMAN Richard L. (US) MISH Michael R. (US) AKTOUDIANAKIS Evangelos (US) PYUN Hyung-jung (US) 24 Délivré le : 27/09/2018 74 Mandataire: GAD CONSULTANTS SCP, B.P. 13448, YAOUNDE (CM). 45 Publié le : 15.11.2018 54 Titre: Toll like receptor modulator compounds. 57 Abrégé : The present disclosure relates generally to toll like receptor modulator compounds, such as diamino pyrido [3,2 D] pyrimidine compounds and pharmaceutical compositions which, among other things, modulate toll-like receptors (e.g. TLR-8), and methods of making and using them. O.A.P.I. – B.P. 887, YAOUNDE (Cameroun) – Tel. (237) 222 20 57 00 – Site web: http:/www.oapi.int – Email: [email protected] 18435 TOLL LIKE RECEPTOR MODULATOR COMPOUNDS CROSS REFERENCE TO RELATED APPLICATIONS [0001] This application claims priority to U.S. Provisional Application Nos. 62/128397, filed March 4, 2015, and 62/250403, filed November 3, 2015, both of which are incorporated herein in their entireties for all purposes. -

Combined Phytochemistry and Chemotaxis Assays For
Combined Phytochemistry and Chemotaxis Assays for Identification and Mechanistic Analysis of Anti-Inflammatory Phytochemicals in Fallopia japonica Ming-Yi Shen, Yan-Jun Liu, Ming-Jaw Don, Hsien-Yueh Liu, Zeng-Weng Chen, Clément Mettling, Pierre Corbeau, Chih-Kang Chiang, Yu-Song Jang, Tzu-Hsuan Li, et al. To cite this version: Ming-Yi Shen, Yan-Jun Liu, Ming-Jaw Don, Hsien-Yueh Liu, Zeng-Weng Chen, et al.. Combined Phy- tochemistry and Chemotaxis Assays for Identification and Mechanistic Analysis of Anti-Inflammatory Phytochemicals in Fallopia japonica. PLoS ONE, Public Library of Science, 2011, 6 (11), pp.e27480. 10.1371/journal.pone.0027480. hal-00645719 HAL Id: hal-00645719 https://hal.archives-ouvertes.fr/hal-00645719 Submitted on 25 May 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution| 4.0 International License Combined Phytochemistry and Chemotaxis Assays for Identification and Mechanistic Analysis of Anti- Inflammatory Phytochemicals in Fallopia japonica Ming-Yi Shen1, Yan-Jun Liu1,2, Ming-Jaw Don3, Hsien-Yueh Liu4, Zeng-Weng Chen1, Cle´ment Mettling5, Pierre Corbeau5, Chih-Kang Chiang6, Yu-Song Jang1, Tzu-Hsuan Li1, Paul Young1, Cicero L. -

Standard Specialty PA and QL List January 2015
Standard Specialty PA and QL List January 2015 Standard PA or PA with QL Programs Therapeutic Category Drug Name Quantity Limit Anti-infectives Antiretrovirals, Hepatitis B BARACLUDE (entecavir) 1 tab/day BARACLUDE (entecavir) Soln 630 ml/30days HEPSERA (adefovir) 1 tab/day TYZEKA (telbivudine ) 1 tab/day Antiretrovirals, HIV FUZEON (enfuvirtide) 60 vials or 1 kit/30 days SELZENTRY (maraviroc) None TRUVADA (emtricitabine/tenofovir) None Cardiology Antilipemic JUXTAPID (lomitapide) 20 mg 3 tabs/day JUXTAPID (lomitapide) 5 mg, 10 mg 1 tab/day KYNAMRO (mipomersen) 4 syringes/28 days Pulmonary Arterial Hypertension ADCIRCA (tadalafil) 2 tabs/day ADEMPAS (riociguat) 90 tabs/30 days FLOLAN (epoprostenol) None LETAIRIS (ambrisentan) 1 tab/day OPSUMIT (macitentan) 1 tab/day ORENITRAM (treprostinil diolamine) None REMODULIN (treprostinil) None REVATIO (sildenafil) 3 tabs or vials/day TRACLEER (bosentan) 2 tabs/day TYVASO (treprostinil) 1 ampule/day VELETRI (epoprostenol) None VENTAVIS (iloprost) 9 ampules/day Vasopressors NORTHERA (droxidopa) None Central Nervous System Anticonvulsants SABRIL (vigabatrin) None Depressant XYREM (sodium oxybate) 3 bottles (540 mL)/30 days Neurotoxins BOTOX (onabotulinumtoxinA) None DYSPORT (abobotulinumtoxinA) None MYOBLOC (rimabotulinumtoxinB) None XEOMIN (incobotulinumtoxinA) None Parkinson's APOKYN (apomorphine) None Sleep Disorder HETLIOZ (tasimelteon) 1 cap/day Dermatology Alkylating Agents VALCHLOR (mechlorethamine) Gel None Endocrinology & Metabolism Gonadotropins ELIGARD (leuprolide) 22.5 mg (3-month) 1 -

Antibodies Targeting Chemokine Receptors CXCR4 and ACKR3
1521-0111/96/6/753–764$35.00 https://doi.org/10.1124/mol.119.116954 MOLECULAR PHARMACOLOGY Mol Pharmacol 96:753–764, December 2019 Copyright ª 2019 by The Author(s) This is an open access article distributed under the CC BY-NC Attribution 4.0 International license. Special Section: From Insight to Modulation of CXCR4 and ACKR3 (CXCR7) Function – Minireview Antibodies Targeting Chemokine Receptors CXCR4 and ACKR3 Vladimir Bobkov, Marta Arimont, Aurélien Zarca, Timo W.M. De Groof, Bas van der Woning, Hans de Haard, and Martine J. Smit Division of Medicinal Chemistry, Amsterdam Institute for Molecules Medicines and Systems, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands (V.B., M.A., A.Z., T.W.M.D.G., M.J.S.); and argenx BVBA, Zwijnaarde, Belgium (V.B., B.W., H.H.) Downloaded from Received April 22, 2019; accepted July 3, 2019 ABSTRACT Dysregulation of the chemokine system is implicated in a number CXCR4 and ACKR3, formerly referred to as CXCR7. We of autoimmune and inflammatory diseases, as well as cancer. discuss their unique properties and advantages over small- molpharm.aspetjournals.org Modulation of chemokine receptor function is a very promising molecule compounds, and also refer to the molecules in approach for therapeutic intervention. Despite interest from preclinical and clinical development. We focus on single- academic groups and pharmaceutical companies, there are domain antibodies and scaffolds and their utilization in GPCR currently few approved medicines targeting chemokine recep- research. Additionally, structural analysis of antibody binding tors. Monoclonal antibodies (mAbs) and antibody-based mole- to CXCR4 is discussed. cules have been successfully applied in the clinical therapy of cancer and represent a potential new class of therapeutics SIGNIFICANCE STATEMENT targeting chemokine receptors belonging to the class of G Modulating the function of GPCRs, and particularly chemokine protein–coupled receptors (GPCRs). -

A Highly Selective and Potent CXCR4 Antagonist for Hepatocellular Carcinoma Treatment
A highly selective and potent CXCR4 antagonist for hepatocellular carcinoma treatment Jen-Shin Songa,1, Chih-Chun Changb,1, Chien-Huang Wua,1, Trinh Kieu Dinhb, Jiing-Jyh Jana, Kuan-Wei Huangb, Ming-Chen Choua, Ting-Yun Shiueb, Kai-Chia Yeha, Yi-Yu Kea, Teng-Kuang Yeha, Yen-Nhi Ngoc Tab, Chia-Jui Leea, Jing-Kai Huanga, Yun-Chieh Sungb, Kak-Shan Shiaa,2, and Yunching Chenb,2 aInstitute of Biotechnology and Pharmaceutical Research, National Health Research Institutes, Miaoli County 35053, Taiwan, Republic of China; and bInstitute of Biomedical Engineering and Frontier Research Center on Fundamental and Applied Sciences of Matters, National Tsing Hua University, 30013 Hsinchu, Taiwan, Republic of China Edited by Michael Karin, University of California San Diego, La Jolla, CA, and approved February 4, 2021 (received for review July 23, 2020) The CXC chemokine receptor type 4 (CXCR4) receptor and its ligand, advanced HCC (9, 17), the concept of which has been experimentally CXCL12, are overexpressed in various cancers and mediate tumor validated by the discovery of a CXCR4 antagonist, BPRCX807. progression and hypoxia-mediated resistance to cancer therapy. AMD3100 was the first Food and Drug Administration (FDA)- While CXCR4 antagonists have potential anticancer effects when approved CXCR4 antagonist used for peripheral blood stem cell combined with conventional anticancer drugs, their poor potency transplantation (PBSCT) (18); however, its application to solid against CXCL12/CXCR4 downstream signaling pathways and sys- tumors is limited by its poor pharmacokinetics and toxic adverse temic toxicity had precluded clinical application. Herein, BPRCX807, effects after long-term administration (19, 20). Thus, a CXCR4 known as a safe, selective, and potent CXCR4 antagonist, has been antagonist with higher safety and better pharmacological and designed and experimentally realized.